
Abstract
Purpose
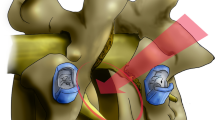
The lateral approach for anterior interbody fusion allows placement of a large footprint intervertebral spacer to indirectly decompress the neural elements through disc height restoration and resultant soft tissue changes. However, it is not well understood under what circumstances indirect decompression in lateral approach surgery is sufficient. This report aimed to evaluate clinical scenarios where indirect decompression was and was not sufficient in symptom resolution when using lateral interbody fusion.
Methods
A prospective study was undertaken of 122 consecutive patients treated with lateral interbody fusion without direct decompression. Pre- and postoperative symptomatology was assessed to evaluate the extent of neural decompression following implantation with a lateral polyetheretherketone spacer. Failure to improve or resolve preoperative radicular pain was considered a failure of indirect decompression and indicated these patients for additional posterior decompressive surgery.
Results
Unplanned second stage decompression was required in 11 patients. Of these patients, 7/11 early in this series had pathology that was underappreciated including spondylolisthesis from high grade facet arthropathy with instability (3), bony lateral recess stenosis (3) and both spondylolisthesis/stenosis (1). Three patients had iatrogenic leg pain through cage misplacement. There was one failure of indirect decompression that could not be explained through retrospective analysis of the patient’s record.
Conclusion
Indirect decompression clearly has a role in minimizing the amount of surgery that is required. However, it is important to consider the circumstances where this technique may be effective and preoperative considerations that may improve patient selection.




Similar content being viewed by others

References
Lurie JD, Tosteson AN, Tosteson TD et al (2008) Reliability of readings of magnetic resonance imaging features of lumbar spinal stenosis. Spine 33:1605–1610
Weinstein JN, Tosteson TD, Lurie JD et al (2008) Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 358:794–810
Smorgick Y, Park DK, Baker KC et al (2013) Single- versus multilevel fusion for single-level degenerative spondylolisthesis and multilevel lumbar stenosis: four-year results of the spine patient outcomes research trial. Spine 38:797–805
Burkus JK, Gornet MF, Dickman CA, Zdeblick TA (2002) Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. J Spinal Disord Tech 15:337–349
Than KD, Wang AC, Rahman SU et al (2011) Complication avoidance and management in anterior lumbar interbody fusion. Neurosurg Focus 31:E6
Arnold PM, Anderson KK, McGuire RA Jr (2011) The lateral transpsoas approach to the lumbar and thoracic spine: a review. Surg Neurol Int 3:S198–S215
Ozgur BM, Aryan HE, Pimenta L, Taylor WR (2006) Extreme lateral interbody fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J 6:435–443
Isaacs RE, Hyde J, Goodrich JA, Rodgers WB, Phillips FM (2010) A prospective, nonrandomized, multicenter evaluation of the extreme lateral interbody fusion for the treatment of adult degenerative scoliosis: perioperative outcomes and complications. Spine 35:S322–S330
Rodgers WB, Gerber EJ, Patterson J (2011) Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine 36:26–32
Malham GM, Ellis NJ, Parker RM, Seex KA (2012) Clinical outcome and fusion rates after the first 30 extreme lateral interbody fusions. Sci World J 2012:246989. doi:10.1100/2012/246989
Berjano P, Balsano M, Burie J, Petruzzi M, Lamartina C (2012) Direct lateral access lumbar and thoracolumbar fusion: preliminary results. Eur Spine J 21:S37–S42
Berjano P, Lamartina C (2013) Far lateral approaches (XLIF) in adult scoliosis. Eur Spine J 22:S242–S253
Khajavi K, Shen AY (2014) Two-year radiographic and clinical outcomes of a minimally invasive, lateral, transpsoas approach for anterior lumbar interbody fusion in the treatment of adult degenerative scoliosis. Eur Spine J 23:1215–1223
Malham GM, Ellis NJ, Parker RM, Seex KA (2014) Maintenance of segmental lordosis and disc height in standalone and instrumented extreme lateral interbody fusion (XLIF). J Spinal Disord Tech. doi:10.1097/BSD.0b013e3182aa4c94
Alimi M, Hofstetter CP, Cong GT et al (2014) Radiological and clinical outcomes following extreme lateral interbody fusion. J Neurosurg Spine 20:623–635
Oliveira L, Marchi L, Coutinho E, Pimenta L (2010) A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements. Spine 35:S331–S337
Uribe JS, Vale FL, Dakwar E (2010) Electromyographic monitoring and its anatomical implications in minimally invasive spine surgery. Spine 35:S368–S374
Tohmeh AG, Rodgers WB, Peterson MD (2011) Dynamically evoked, discrete-threshold electromyography in the extreme lateral interbody fusion approach. J Neurosurg Spine 14:31–37
Boden SD, Zdeblick TA, Sandhu HS, Heim SE (2000) The use of rhBMP-2 in interbody fusion cages. Definitive evidence of osteoinduction in humans: a preliminary report. Spine 25:376–381
Williams AL, Gornet MF, Burkus JK (2005) CT evaluation of lumbar interbody fusion: current concepts. AJNR Am J Neuroradiol 26:2057–2066
Malham GM, Parker RM, Goss B, Blecher CM, Ballok ZE (2014) Indirect foraminal decompression is independent of metabolically active fact arthropathy in extreme lateral interbody fusion. Spine 39:E1303–E1310
Kepler CK, Sharma AK, Huang RC et al (2012) Indirect foraminal decompression after lateral transpsoas interbody fusion. J Neurosurg Spine 16:329–333
Elowitz EH, Yanni DS, Chwajol M et al (2011) Evaluation of indirect decompression of the lumbar spinal canal following minimally invasive lateral transpsoas interbody fusion: radiographic and outcome analysis. Minim Invasive Neurosurg 54:201–206
Marchi L, Amaral R, Oliveira L et al (2012) Stand-alone lateral interbody fusion for the treatment of low-grade degenerative spondylolisthesis. Sci World J 2012:456346. doi:10.1100/2012/456346
Malham GM, Parker RM, Ballok ZE, Goss B, Diwan AD, Uribe JS (2014) Bone scans are reliable for the identification of lumbar disk and facet pathology. Glob Spine J. doi:10.1055/s-0034-1394298
Conflict of interest
No funds were received in support of this work. BG is employed by NuVasive Australia & NZ Pty Ltd. The authors have full control of all primary data and agree to allow the journal to review the data if requested.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Malham, G.M., Parker, R.M., Goss, B. et al. Clinical results and limitations of indirect decompression in spinal stenosis with laterally implanted interbody cages: results from a prospective cohort study. Eur Spine J 24 (Suppl 3), 339–345 (2015). https://doi.org/10.1007/s00586-015-3807-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-3807-3