
Abstract
Background
Anterior cervical discectomy and fusion (ACDF) using stand-alone cages is an effective method of treating degenerative disease. However, stand-alone cages are reported to have a relatively high incidence of implant subsidence with secondary kyphotic deformity particularly after multilevel ACDF. The purpose of our article was to investigate clinical and radiological outcomes after ACDF using stand-alone cages, at two contiguous levels, with a particular focus on changes in regional alignment and the correlation between alignment of the operated cervical levels and the entire cervical spine.
Methods
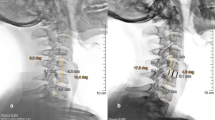
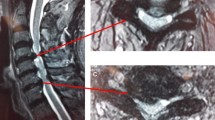
Twenty-seven patients with 54 levels and a mean age of 50.8 years were enrolled between January 2005 and August 2006. They underwent ACDF using polyetheretherketone cages packed with demineralized bone matrix without plate fixation at two contiguous levels. Mean follow-up period was 25.5 months (range, 13–60). Clinical outcome was evaluated using two Visual Analog Scales and the Neck Disability Index (NDI). We assessed fusion, regional alignment (RA) of the operated levels and cervical global alignment (GA) preoperatively in the immediate 1-week postoperative period and at the final follow-up. An interspinous distance ≥2 mm was used as an indicator of pseudoarthrosis at each level.
Findings
All patients showed improvements in clinical outcome, with 96% of patients showing mild NDI scores (<14). Radiological solid fusion was obtained at 48 of 54 levels (88.9%) and in 21 of 27 patients (77.8%). Lower cervical levels were significantly more vulnerable to pseudoarthrosis (100%). Fusion rate had no significant correlation with outcome (p > 0.05). RA of the operated levels was improved at the final follow-up compared with preoperatively in 76% of patients, although it had decreased compared with the immediate postoperative period due to subsidence in 84% of patients. In total, 80.8% of patients showed improvements in GA. Furthermore, improvements in RA showed a significant positive correlation with those in GA (p = 0.001), although improvement in RA and GA did not correlate significantly with clinical outcome (p > 0.05).
Conclusions
Though some degree of subsidence occurred in most cases, RA had improved at the last follow-up compared with preoperatively, which contributed to the significant improvement in GA. However, improvement of RA and GA was not correlated with outcomes.




Similar content being viewed by others
References
Barsa P, Suchomel P (2007) Factors affecting sagittal malalignment due to cage subsidence in standalone cage assisted anterior cervical fusion. Eur Spine J 16:1395–1400
Bartels RHMA, Donk R, Feuth T (2006) Subsidence of stand-alone cervical carbon fiber cages. Neurosurgery 58:502–508
Cannada LK, Scherping SC, Yoo JU, Jones PK, Emery SE (2003) Pseudoarthrosis of the cervical spine: a comparison of radiographic diagnostic measures. Spine (Phila Pa 1976) 28:46–51
Cho DY, Lee WY, Sheu PC (2004) Treatment of multilevel cervical fusion with cages. Surg Neurol 62:378–385, discussion 385-376
Cloward R (2007) The anterior approach for removal of ruptured cervical disks. 1958. J Neurosurg Spine 6:496–511
Demircan MN, Kutlay AM, Colak A, Kaya S, Tekin T, Kibici K, Ungoren K (2007) Multilevel cervical fusion without plates, screws or autogenous iliac crest bone graft. J Clin Neurosci 14:723–728
Etebar S, Cahill DW (1999) Risk factors for adjacent-segment failure following lumbar fixation with rigid instrumentation for degenerative instability. J Neurosurg 90:163–169
Fujibayashi S, Neo M, Nakamura T (2008) Stand-alone interbody cage versus anterior cervical plate for treatment of cervical disc herniation: sequential changes in cage subsidence. J Clin Neurosci 15:1017–1022
Gercek E, Arlet V, Delisle J, Marchesi D (2003) Subsidence of stand-alone cervical cages in anterior interbody fusion: warning. Eur Spine J 12:513–516
Heidecke V, Rainov NG, Marx T, Burkert W (2000) Outcome in Cloward anterior fusion for degenerative cervical spinal disease. Acta Neurochir Wien 142:283–291
Jackson RP, McManus AC (1994) Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine (Phila Pa 1976) 19:1611–1618
Kaiser M, Mummaneni P, Matz P, Anderson P, Groff M, Heary R, Holly L, Ryken T, Choudhri T, Vresilovic E, Resnick D (2009) Radiographic assessment of cervical subaxial fusion. J Neurosurg Spine 11:221–227
Kaiser MG, Haid RW Jr, Subach BR, Barnes B, Rodts GE Jr (2002) Anterior cervical plating enhances arthrodesis after discectomy and fusion with cortical allograft. Neurosurgery 50:229–236, discussion 236-228
Katsuura A, Hukuda S, Imanaka T, Miyamoto K, Kanemoto M (1996) Anterior cervical plate used in degenerative disease can maintain cervical lordosis. J Spinal Disord 9:470–476
Katsuura A, Hukuda S, Saruhashi Y, Mori K (2001) Kyphotic malalignment after anterior cervical fusion is one of the factors promoting the degenerative process in adjacent intervertebral levels. Eur Spine J 10:320–324
Kulkarni A, Hee H, Wong H (2007) Solis cage (PEEK) for anterior cervical fusion: preliminary radiological results with emphasis on fusion and subsidence. Spine J 7:205–209
Kumar MN, Baklanov A, Chopin D (2001) Correlation between sagittal plane changes and adjacent segment degeneration following lumbar spine fusion. Eur Spine J 10:314–319
Lee H, Nicholson L, Adams R, Maher C, Halaki M, Bae S-S (2006) Development and psychometric testing of Korean language versions of 4 neck pain and disability questionnaires. Spine (Phila Pa 1976) 31:1841–1845
Oda I, Cunningham BW, Buckley RA, Goebel MJ, Haggerty CJ, Orbegoso CM, McAfee PC (1999) Does spinal kyphotic deformity influence the biomechanical characteristics of the adjacent motion segments? An in vivo animal model. Spine (Phila Pa 1976) 24:2139–2146
Park P, Garton H, Gala V, Hoff J, McGillicuddy J (2004) Adjacent segment disease after lumbar or lumbosacral fusion: review of the literature. Spine (Phila Pa 1976) 29:1938–1944
Smith GW, Robinson RA (1958) The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg 40A:607–624
Thom C, Leheta O, Krauss J, Zevgaridis D (2006) A prospective randomized comparison of rectangular titanium cage fusion and iliac crest autograft fusion in patients undergoing anterior cervical discectomy. J Neurosurg Spine 4:1–9
Topuz K, Colak A, Kaya S, Simşek H, Kutlay M, Demircan M, Velioğlu M (2009) Two-level contiguous cervical disc disease treated with peek cages packed with demineralized bone matrix: results of 3-year follow-up. Eur Spine J 18:238–243
Vavruch L, Hedlund R, Javid D, Leszniewski W, Shalabi A (2002) A prospective randomized comparison between the cloward procedure and a carbon fiber cage in the cervical spine: a clinical and radiologic study. Spine (Phila Pa 1976) 27:1694–1701
Wang JC, McDonough PW, Endow KK, Delamarter RB (2000) Increased fusion rates with cervical plating for two-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976) 25:41–45
Wang JC, McDonough PW, Kanim LE, Endow KK, Delamarter RB (2001) Increased fusion rates with cervical plating for three-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976) 26:643–646
Wright IP, Eisenstein SM (2007) Anterior cervical discectomy and fusion without instrumentation. Spine (Phila Pa 1976) 32:772–774, discussion 775
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Moon, H.J., Kim, J.H., Kim, JH. et al. The effects of anterior cervical discectomy and fusion with stand-alone cages at two contiguous levels on cervical alignment and outcomes. Acta Neurochir 153, 559–565 (2011). https://doi.org/10.1007/s00701-010-0879-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-010-0879-z