
Abstract
Objectives
This study aimed to compare the learning curves of percutaneous endoscopic lumbar discectomy (PELD) in a transforaminal approach at the L4/5 and L5/S1 levels.
Methods
We retrospectively reviewed the first 60 cases at the L4/5 level (Group I) and the first 60 cases at the L5/S1 level (Group II) of PELD performed by one spine surgeon. The patients were divided into subgroups A, B, and C (Group I: A cases 1–20, B cases 21–40, C cases 41–60; Group II: A cases 1–20, B cases 21–40, C cases 41–60). Operation time was thoroughly analyzed.
Results
Compared with the L4/5 level, the learning curve of transforaminal PELD at the L5/S1 level was flatter. The mean operation times of Groups IA, IB, and IC were (88.75±17.02), (67.75±6.16), and (64.85±7.82) min, respectively. There was a significant difference between Groups A and B (P<0.05), but no significant difference between Groups B and C (P=0.20). The mean operation times of Groups IIA, IIB, and IIC were (117.25±13.62), (109.50±11.20), and (92.15±11.94) min, respectively. There was no significant difference between Groups A and B (P=0.06), but there was a significant difference between Groups B and C (P<0.05). There were 6 cases of postoperative dysesthesia (POD) in Group I and 2 cases in Group IIA (P=0.27). There were 2 cases of residual disc in Group I, and 4 cases in Group II (P=0.67). There were 3 cases of recurrence in Group I, and 2 cases in Group II (P>0.05).
Conclusions
Compared with the L5/S1 level, the learning curve of PELD in a transforaminal approach at the L4/5 level was steeper, suggesting that the L4/5 level might be easier to master after short-term professional training.
中文概要
目 的
探讨经皮椎间孔镜技术治疗腰4/5 和腰5 骶1 椎间盘突出症学习曲线之间的差异。
创新点
本文第一次比较了经皮椎间孔镜治疗腰4/5 和腰5/骶1 椎间盘突出症的学习曲线,得出经皮椎间孔镜治疗腰4/5 椎间盘突出症的学习曲线更加陡峭,经过专业化培训更加容易掌握,为初学者提供了指导方向。
方 法
回顾性分析2011 年6 月至2013 年8 月于上海市第十人民医院行经皮椎间孔镜治疗的120 例腰4/5 和腰5 骶1椎间盘突出症患者的临床资料。120例患者由同一术者实行手术操作,根据突出节段不同分为两组:腰4/5 组(组I)60 例和腰5 骶1组(组II)60 例。每组又分成三个亚组:组IA 1∼20、IB 21∼40、IC 41∼60;组IIA 1∼20、IIB 21∼40、IIC 41∼60。分别记录每位患者的手术时间。
结 论
实验结果显示:组IA、IB、IC 平均手术时间分别为(88.75±17.02) 、(67.75±6.16) 和(64.85±7.82) min,组IA 与组IB 之间的差异有统计学意义,组IB 与组IC 之间的差异无统计学意义;组IIA、IIB、IIC 平均手术时间分别为(117.25±13.62)、(109.50±11.20)和(92.15±11.94) min,组IIA 与组IIB之间的差异无统计学意义,组IIB 与组IIC 之间的差异有统计学意义。术后8 例患者出现术后感觉减退(POD),其中组I 有6 例,组II 有2 例。术后磁共振成像(MRI)检查有6 例患者有椎间盘残留,其中组I 有2 例,组II 有4 例。术后随访5 例患者复发,其中组I 有3 例,组II 有2 例,但差异无统计学意义。与腰5 骶1 学习曲线相比,经皮椎间孔镜治疗腰4/5 椎间盘突出的学习曲线更加陡峭,经过专业化培训更加容易掌握。
Similar content being viewed by others


1 Introduction
Lumbar disc herniation (LDH) is considered to be the most common reason for lumbar spinal surgery (Cheng et al., 2014), which often occurs at the L4/5 or L5/S1 level. Among lumbar surgery procedures, microdiscectomy is a practical technique to surgically manage LDH and results in favorable clinical out-comes (Brouwer et al., 2015). However, microdiscectomy often requires muscle retraction, bone resection of the lamina and facet joint, and dural sac and nerve retraction. This can cause muscular injury and scarring of the epidural space, which is regarded as the main post-discectomy problem (Bokov et al., 2011). For decades, minimally invasive techniques have been widely used to minimize these disadvantages (Fan et al., 2015d). Percutaneous endoscopic lumbar discectomy (PELD) in a transforaminal approach has been validated as a potential alternative to microdiscectomy or open discectomy (Ahn, 2012; Gibson et al., 2012). PELD has numerous advantages over open discectomy, such as the preservation of normal paraspinal structures, minimal postoperative pain, and low risk of epidural scarring and iatrogenic instability (Ahn et al., 2003; Lee D.Y. et al., 2006; 2009; Lee S.H. et al., 2006).
However, PELD poses challenges to surgeons and the difficulty of the approach is daunting to many potential users (Ruetten et al., 2007). Fortunately, the learning curve of the PELD technique can be managed by standard training and eligible subject selection (Kafadar et al., 2006). Many studies have discussed different aspects of the learning curve of PELD (Lee and Lee, 2008; Wang B. et al., 2011; Chaichankul et al., 2012; Hsu et al., 2013; Wang H. et al., 2013). However, no papers have compared the learning curve of PELD in a transforaminal approach at the L4/5 and L5/S1 levels. In contrast to L4/5, the L5/S1 level presents unique anatomical limitations to the transforaminal approach, such as a high iliac crest, large facet joint, large L5 transverse process, narrowed disc space, and narrow foramen (Mirkovic et al., 1995; Reulen et al., 1996). Due to these anatomical limitations, the transforaminal approach for L5/S1 may be more difficult in some aspects, such as puncture and indwelling the channel. Therefore, we retrospectively reviewed our experience with PELD in transforaminal approach for the L4/5 and L5/S1 levels to determine the learning curve for a single surgeon learning this technique.
2 Materials and methods
2.1 Patients and groupings
This study was approved by the Human Research Ethics Board of an affiliated Tenth People’s Hospital of Tongji University in Shanghai, China. We conducted a retrospective review of 120 medical records of those who had buttock and leg pain due to single-level disc herniation and underwent PELD by one surgeon in our department between June 2011 and August 2013. Baseline characteristics for clinical information including age, gender, conservative treatment time, pain location, and follow-up were collected. The surgeon GU had more than ten-year experience of open spine surgery but no previous experience with percutaneous endoscopic procedures. Before attempting full-endoscopic discectomy, the surgeon practiced PELD on a cadaver and had one year of PELD training from surgeon HE. The surgeon GU then conducted PELD on patients with L4/5 LDH and L5/S1 LDH under the supervision of surgeon HE during the same period. Consent forms were obtained from the patients before the operation. The surgeon’s first 60 PELD cases of L4/5 LDH and first 60 PELD cases of L5/S1 LDH were included in the analysis. The two types of operation were conducted alternately during the same period. The patients were regarded as two groups (Group I: 60 patients of L4/5 LDH; Group II: 60 patients of L5/S1 LDH) and each group was subdivided into three subgroups, A, B, and C (Group I: A cases 1–20, B cases 21–40, C cases 41–60; Group II: A cases 1–20, B cases 21–40, C cases 41–60).
2.2 Inclusion and exclusion criteria
Inclusion criteria for the study were paracentral LDH, central LDH, foraminal LDH, or combinations of two or three of these conditions. Patients assigned to Group I were: (1) patients complaining of low back pain with lower limb pain or numbness, especially in the area of the anterolateral crus; (2) examination showed a positive response to a straight-leg raising test (<60°) and an augmentation test, and hypoesthesia and decreased muscle force in the legs; (3) magnetic resonance imaging (MRI)/computed tomography (CT) confirmed disc herniation and nerve compression. Patients assigned to Group II had the same inclusion criteria as those assigned to Group I except that the pain or numbness was mainly in the area of the posterior crus.
Exclusion criteria were: (1) symptoms and radiography assessments did not meet the abovementioned criteria; (2) CT scans confirmed evident disc calcification; (3) previous surgery history for segmental lesions; (4) dynamic imaging X-ray indicated lumbar spinal instability; (5) extraforaminal disc herniation; (6) sacralization in L5/S1 disc herniation; (7) cases with concomitant disc herniations at L4/5 and L5/S1.
2.3 Surgical technique
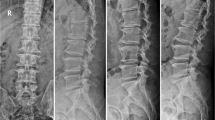
The patients were asked to lie on the operating table and all received local anesthesia. They were routinely informed about all PELD procedures. Communication between the surgeon and patients was maintained intraoperatively. Biplane fluoroscopy was used. Depending on the patient’s weight, gender, and surgical level, the entry point was selected 12–16 cm from the midline at the L5/S1 level, and 11–14 cm from the midline at the L4/5 level (Fig. 1).

Comparative traces of the cannula in cases with L4/5 and L5/S1 disc herniations
(a) Lateral view; (b) Posterior view
For L4/5 level LDH patients, transforaminal PELD was conducted according to the standard procedure described by Ruetten et al. (2007). After local anesthetics at the entry point, an 18-gauge needle was inserted posterolaterally under intraoperative fluoroscopic guidance and aimed at the desired foramen. Then, a guidewire was inserted through the needle into the target foramen and the needle was removed. Over the guidewire, an incision of 8 mm was made, and stepwise dilatation tubes were put in place. Then, a cannulated dilator was inserted and the guidewire was removed. A working channel was directly placed in the herniation spot. Next, an endoscope was placed through the working channel. The extruding disc was removed using endoscopic forceps and radio frequency. The nerve root was regarded as free and mobile when we frequently stopped and opened saline infusion. After the herniated disc was completely removed, the endoscope and cannula were withdrawn, and the skin was closed with one stitch. For patients with L4/5 lumbar foraminal stenosis or L5/S1 LDH, the PELD was performed according to the standard procedure described by Hoogland et al. (2008). Preoperative location and anesthesia were conducted according to the procedure described by Ruetten et al. (2007).
2.4 Observational outcomes
Operation time, duration of hospital stay, one-year recurrence rate, postoperative complications, Oswestry disability index (ODI), and the visual analogue scale (VAS) were recorded and analyzed.
2.5 Statistical analysis
The analysis of variance (ANOVA) test, Chisquare test, Kruskal-Wallis test, Wilcoxon rank sum test, and Fisher’s exact test were used to compare the differences in each parameter between the two groups. All analyses were performed using SPSS Version 19.0 with P<0.05 as the significance level.
3 Results
A total of 120 patients were included in our study, namely 60 with L4/5 LDH and another 60 with L5/S1 LDH. There were 24 males and 36 females in Group I with an average age of (39.48±11.57) years. There were 32 males and 28 females in Group II with an average age of (41.03±13.82) years. The conservative treatment time was (4.82±2.43) months for Group I and (4.50±2.02) months for Group II. All patients were followed up without loss for at least 12 months via phone or outpatient rechecks. No significant differences in age, gender, conservative treatment time, follow-up, or pain location were identified (Table 1). The mean hospital stay was (1.53±0.77) d for Group I and (1.60±0.79) d for Group II (P=0.64).
The mean operation times of Groups IA, IB, and IC were (88.75±17.02), (67.75±6.16), and (64.85± 7.82) min, respectively (Table 2). The operation time of Group IA was significantly different from those of Groups IB and IC (P<0.05), but there was no significant difference between the operation times of Groups IB and IC (P=0.20). The mean operation times of Groups IIA, IIB, and IIC were (117.25±13.62), (109.50±11.20), and (92.15±11.94) min, respectively. No significant difference was detected between the operation times of Groups IIA and IIB (P=0.06). However, a significant difference was observed between Groups IIB and IIC (P<0.05). Compared with L5/S1, the learning curve of PELD in transforaminal approach at L4/5 level was steeper (Fig. 2).

Learning curves of percutaneous endoscopic lumbar discectomy in the transforaminal approach
(a) L4/5 level; (b) L5/S1 level
The preoperative and one-year postoperative back pain VAS measurements were 6.03±1.07 and 1.20±0.95, respectively (P<0.01) for Group I, and 6.33±1.13 and 1.35±0.85, respectively (P<0.01) for Group II (Table 3). The preoperative and one-year postoperative leg pain VAS measurements were 5.97±1.18 and 1.08±0.98, respectively (P<0.01) for Group I, and 6.33±1.28 and 1.53±1.00, respectively (P<0.01) for Group II. The preoperative and postoperative one-year ODI scores were 33.67±5.55 and 7.30±2.48, respectively (P<0.01) for Group I and 32.17±4.87 and 6.27±2.39, respectively (P<0.01) for Group II.
In Group I, all 60 patients underwent PELD without transfer to microendoscopic discectomy (MED) or microdiscectomy, but two of the 60 patients in Group II were transferred to MED due to a difficult puncture or channel indwelling. There were six cases (10%) of postoperative dysesthesia (POD) in Group I, four in Group IA and two in Group IB. Among these six cases, four patients complained of POD on the anterolateral crus and interior thigh due to L4 root injury, which improved one week after the surgery; one patient suffered from drop foot due to L5 injury, but dorsal hallux force improved from Grade II to Grade IV three months after the operation; one patient complained of residual numbness 12 months after the operation. There were two cases (3.3%) of POD in Group IIA after the operation: one patient complained of postoperative hyperesthesia on the lateral thigh, but the symptoms were relieved two weeks later; the other complained of residual numbness 12 months later.
There were two cases (3.3%) of symptomatic residual disc in Group I, one in Group IA and one in Group IB. One of these patients received MED to clear the disc residue and achieved complete relief; the other received conservative treatment and obtained symptom relief three months after the operation. There were four cases (6.7%) of residual disc in Group II, three in Group IIA, and one in Group IIB. Two received MED to clear disc residue, one received fusion surgery and achieved complete relief, and one received conservative treatment, and symptoms were relieved one month after the operation. There were three cases with recurrence in Group I, and two in Group II. The mean time of recurrence was 6.4 months. Two cases received conservative treatment with partial relief, and the other three received fusion surgery. There were no significant differences in complication rate or recurrence rate between the two groups (P>0.05).
4 Discussion
The clinical efficacy of PELD has been confirmed by many studies (Hoogland et al., 2008; Nellensteijn et al., 2010; Jasper et al., 2013), but learning curve evaluation is essential in this regard (Benzel and Orr, 2011). To the best of our knowledge, this is the first study to compare the learning curves of PELD in a transforaminal approach at the L4/5 and L5/S1 levels. Our study confirmed the hypothesis that PELD in a transforaminal approach was more difficult to learn at the L5/S1 level than at the L4/5 level.
The learning curve is defined as a graphic interpretation of the theory that more experience is accumulated, the more a task is repeated (Benzel and Orr, 2011). The aim of our investigation of PELD was to explore how many cases should be performed to master the technique. Lee and Lee (2008) reported their first 51 consecutive PELD cases and found that the learning curve seemed to be acceptable with standard training. However, Hsu et al. (2013) compared the learning curve of a transforaminal approach with that of an interlaminar approach for a single surgeon learning this technique. They demonstrated that the learning curve of the transforaminal approach was steep while that of the interlaminar approach was flat, which indicated that the transforaminal approach was easier to learn than the interlaminar approach. In addition, Wang et al. (2013) found that the training level of minimally invasive spine surgery played a role in increasing the rate of learning. In our study, the learning curve of transforaminal PELD at the L5/S1 level was shallower than that at the L4/5 level (Fig. 1). Specifically, significant differences were observed when the operation time of Group IA was compared with Groups IB and IC, but no significant differences were detected between Groups IB and IC. No significant differences were observed when the operation time of Group IIA was compared with that of Group IIB. However, significant differences in operation time were observed between Groups IIA and IIC, and similarly, between Groups IIB and IIC. These findings indicated that the surgeon had mastered the technical skills of L4/5 transforaminal PELD during the first 20 cases, but had to work through 40 cases of L5/S1 to shorten the operation time and minimize the complications. These differences can be explained by the surgical procedure of transforaminal PELD. At the L4/5 level, the puncture and channel indwelling is relatively simple because there are no problems with the iliac crest or transverse process. At the L5/S1 level, however, the unique anatomy of a high iliac crest, large facet joint, large L5 transverse process, narrowed disc space, and narrow foramen complicates the process of puncture and channel indwelling. Thus, it will take a long time for beginners to master the transforaminal PELD at the L5/S1 level.
The rapid spread of PELD has been limited by difficult puncture, potential damage to neural and vascular structures, abdominal organs and reoperation of the surgery. In our study, there were two cases intended to receive transforaminal PELD at L5/S1 level, which were transferred to MED due to difficult puncture and channel indwelling. The rate of nerve injury has been reported to vary from 1.0% to 8.9% (Sairyo et al., 2014). Although exiting root injury is not a life-threatening complication, patients cannot return to their daily life rapidly. In our study, the occurrence of POD was 10% in Group I, and 3.3% in Group II. The difference might be correlated with the anatomical features. Our previous study found that the exit root at the L4/5 level has a steeper slope than that at the L5/S1 level, and the distance between the exit root and the posterior disc is shorter (Gu et al., 2013; Guan et al., 2015). This anatomical difference might lead to a higher risk of compression of the working channel at the L4/5 exit, which would injure the dorsal root ganglia and increase the rate of occurrence of POD. Postoperative intervertebral disc residue is another common complication of PELD. In our study, there were six cases of disc residue confirmed by MRI, two in Group I and four in Group II. This difference may also be explained by the special anatomy of L5/S1. At the L5/S1 level, the puncture and locating were complicated by a high iliac crest and large L5 transverse process. As a result, when the puncture location was inappropriate, the herniated disc could not be exposed adequately in the working channel. Furthermore, the L5/S1 nerve root was not exposed adequately and may have adhered to the disc, resulting in inadequate disc separation. Finally, the recurrence of PELD should also be noted. Choi et al. (2015) found 78 patients with recurrence in 10288 PELD cases (0.8%), which was lower than the numbers we found (4/60 and 3/60). This difference might be explained by unskilled performance of transforaminal PELD at the start of our study. Our study also indicated that the operation section did not correlate with the recurrence rate, which was thought to be correlated with age, body mass index, protrusion and Modic change (Kim et al., 2007).
The reasons that PELD is difficult to learn can be explained as follows. PELD in a transforaminal approach is a novel technique. Spine surgeons are familiar with the posterior anatomy because they have performed posterior surgery for decades. For a posterolateral approach, however, the anatomical structure of the intervertebral foramen is strange to them, so it is understandable that it may take more time to master this novel technique. Additionally, some aspects of the transforaminal approach for L5/S1 may be more difficult to learn, such as the puncture and indwelling the working channel, with high postoperative complication rates and longer operation time. This may cause new learners to give up halfway. In our view, there are two solutions to overcoming difficulties in learning PELD in a transforaminal approach, in addition to practicing on cadavers and receiving demonstration teaching from senior surgeons. Firstly, it would be very beneficial to use our HE’s lumbar location (HELLO) system to guide the puncture. This system has been shown to reduce the puncture time and minimize radiation exposure (Fan et al., 2015a; 2015b; 2015c). Lastly, it has been widely accepted that foraminoplasty may be conducted during transforaminal PELD. This would be very helpful because the enlargement of intervertebral foramen will allow the working channel to optimize the location.
This retrospective study had some limitations. Firstly, there might be a potential mutual impact on the learning process between the L4/5 and L5/S1 levels. However, this inherent limitation could not be avoided as we aimed to compare the learning curves of transforaminal PELD at the L4/5 and L5/S1 levels by one surgeon. Secondly, the study sample was relatively small, but we considered that the first 120 PELD cases in the transforaminal approach would be adequate to clarify the issue. Lastly, the hospital stay was a little longer than those receiving PELD in American or European countries. This was because in China this technique is not classified as outpatient surgery. In the future, we may conduct a prospective study to compare cases of upper LDH with cases of lower LDH. The upper lumbar is between the lower thoracic vertebrae and the lower lumbar, which is an area between kyphosis and lordosis (Kim et al., 2010). As a result, the space between the dura and disc is narrow, and the root is short and near the lumbosacral enlargement (Sanderson et al., 2004). Due to these anatomical features, transforaminal PELD is a technical challenge with a higher risk of nerve injury and a lower success rate. Therefore, it would be interesting to investigate the learning curve of PELD at the upper lumbar level.
5 Conclusions
The learning curve of PELD in the transforaminal approach was steeper and easier to master at the L4/5 level than at the L5/S1 level. Professional training is essential for junior surgeons to master transforaminal PELD.
Contributors
Xin-bo WU, Guo-xin FAN, Xin GU, and Tu-gang SHEN designed the study and wrote the manuscript. Xiao-fei GUAN and An-nan HU were involved in the data collection and analysis. Hai-long ZHANG provided critical advice. Shi-sheng HE approved the final version.
Compliance with ethics guidelines
Xin-bo WU, Guo-xin FAN, Xin GU, Tu-gang SHEN, Xiao-fei GUAN, An-nan HU, Hai-long ZHANG, and Shisheng HE declare that they have no conflict of interest.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
References
Ahn, Y., 2012. Transforaminal percutaneous endoscopic lumbar discectomy: technical tips to prevent complications. Expert Rev. Med. Devices, 9(4):361–366. http://dx.doi.org/10.1586/erd.12.23
Ahn, Y., Lee, S.H., Park, W.M., et al., 2003. Posterolateral percutaneous endoscopic lumbar foraminotomy for L5-S1 foraminal or lateral exit zone stenosis. Technical note. J. Neurosurg., 99(3 Suppl.):320–323. http://dx.doi.org/10.3171/spi.2003.99.3.0320
Benzel, E.C., Orr, R.D., 2011. A steep learning curve is a good thing! Spine J., 11(2):131–132. http://dx.doi.org/10.1016/j.spinee.2010.12.012
Bokov, A., Isrelov, A., Skorodumov, A., et al., 2011. An analysis of reasons for failed back surgery syndrome and partial results after different types of surgical lumbar nerve root decompression. Pain Physician, 14(6):545–557.
Brouwer, P.A., Brand, R., van den Akker-van Marle, M.E., et al., 2015. Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. Spine J., 15(5):857–865. http://dx.doi.org/10.1016/j.spinee.2015.01.020
Chaichankul, C., Poopitaya, S., Tassanawipas, W., 2012. The effect of learning curve on the results of percutaneous transforaminal endoscopic lumbar discectomy. J. Med. Assoc. Thai, 95(Suppl. 10):S206–S212.
Cheng, Y.P., Lee, K.W., Lin, P.Y., et al., 2014. Full-endoscopic interlaminar removal of chronic lumbar epidural hematoma after spinal manipulation. Surg. Neurol. Int., 5(1):55. http://dx.doi.org/10.4103/2152-7806.131106
Choi, K.C., Lee, J.H., Kim, J.S., et al., 2015. Unsuccessful percutaneous endoscopic lumbar discectomy: a singlecenter experience of 10228 cases. Neurosurgery, 76(4): 372–381. http://dx.doi.org/10.1227/neu.0000000000000628
Fan, G., Guan, X., Sun, Q., et al., 2015a. Puncture reduction in percutaneous transforaminal endoscopic discectomy with HE’s Lumbar LOcation (HELLO) system: a cadaver study. PLoS ONE, 10(12):e0144939. http://dx.doi.org/10.1371/journal.pone.0144939
Fan, G., Fu, Q., Gu, G., et al., 2015b. Radiation exposure to surgeon in minimally invasive transforaminal lumbar interbody fusion with novel spinal locators. J. Spinal Disord. Tech., 28(3):E173–E180. http://dx.doi.org/10.1097/bsd.0000000000000210
Fan, G., Guan, X., Zhang, H., et al., 2015c. Significant improvement of puncture accuracy and fluoroscopy reduction in percutaneous transforaminal endoscopic discectomy with novel lumbar location system: preliminary report of prospective HELLO study. Medicine (Baltimore), 94(49):e2189. http://dx.doi.org/10.1097/md.0000000000002189
Fan, G., Han, R., Zhang, H., et al., 2015d. Worldwide research productivity in the field of minimally invasive spine surgery: a 20-year survey of publication activities. Spine (Phila Pa 1976), Epub ahead of print. http://dx.doi.org/10.1097/brs.0000000000001393
Gibson, J.N.A., Cowie, J.G., Iprenburg, M., 2012. Transforaminal endoscopic spinal surgery: the future ‘gold standard’ for discectomy? A review. Surgeon, 10(5):290–296. http://dx.doi.org/10.1016/j.surge.2012.05.001
Gu, X., He, S.S., Zhang, H.L., 2013. Morphometric analysis of the YESS and TESSYS techniques of percutaneous transforaminal endoscopic lumbar discectomy. Clin. Anat., 26(6):728–734. http://dx.doi.org/10.1002/ca.22286
Guan, X., Gu, X., Zhang, L., et al., 2015. Morphometric analysis of the working zone for posterolateral endoscopic lumbar discectomy based on magnetic resonance neurography. J. Spinal Disord. Tech., 28(2):E78–E84. http://dx.doi.org/10.1097/bsd.0000000000000145
Hoogland, T., van den Brekel-Dijkstra, K., Schubert, M., et al., 2008. Endoscopic transforaminal discectomy for recurrent lumbar disc herniation: a prospective, cohort evaluation of 262 consecutive cases. Spine (Phila Pa 1976), 33(9):973–978. http://dx.doi.org/10.1097/BRS.0b013e31816c8ade
Hsu, H.T., Chang, S.J., Yang, S.S., et al., 2013. Learning curve of full-endoscopic lumbar discectomy. Eur. Spine J., 22(4):727–733. http://dx.doi.org/10.1007/s00586-012-2540-4
Jasper, G.P., Francisco, G.M., Telfeian, A.E., 2013. Clinical success of transforaminal endoscopic discectomy with foraminotomy: a retrospective evaluation. Clin. Neurol. Neurosurg., 115(10):1961–1965. http://dx.doi.org/10.1016/j.clineuro.2013.05.033
Kafadar, A., Kahraman, S., Akbörü, M., 2006. Percutaneous endoscopic transforaminal lumbar discectomy: a critical appraisal. Minim. Invasive Neurosurg., 49(2):74–79. http://dx.doi.org/10.1055/s-2006-932184
Kim, D.S., Lee, J.K., Jang, J.W., et al., 2010. Clinical features and treatments of upper lumbar disc herniations. J. Korean Neurosurg. Soc., 48(2):119–124. http://dx.doi.org/10.3340/jkns.2010.48.2.119
Kim, J.M., Lee, S.H., Ahn, Y., et al., 2007. Recurrence after successful percutaneous endoscopic lumbar discectomy. Minim. Invasive Neurosurg., 50(2):82–85. http://dx.doi.org/10.1055/s-2007-982504
Lee, D.Y., Lee, S.H., 2008. Learning curve for percutaneous endoscopic lumbar discectomy. Neurol. Med. Chir. (Tokyo), 48(9):383–388, discussion 388–389.
Lee, D.Y., Ahn, Y., Lee, S.H., 2006. Percutaneous endoscopic lumbar discectomy for adolescent lumbar disc herniation: surgical outcomes in 46 consecutive patients. Mt. Sinai J. Med., 73(6):864–870.
Lee, D.Y., Shim, C.S., Ahn, Y., et al., 2009. Comparison of percutaneous endoscopic lumbar discectomy and open lumbar microdiscectomy for recurrent disc herniation. J. Korean Neurosurg. Soc., 46(6):515–521. http://dx.doi.org/10.3340/jkns.2009.46.6.515
Lee, S.H., Chung, S.E., Ahn, Y., et al., 2006. Comparative radiologic evaluation of percutaneous endoscopic lumbar discectomy and open microdiscectomy: a matched cohort analysis. Mt. Sinai J. Med., 73(5):795–801.
Mirkovic, S.R., Schwartz, D.G., Glazier, K.D., 1995. Anatomic considerations in lumbar posterolateral percutaneous procedures. Spine (Phila Pa 1976), 20(18):1965–1971.
Nellensteijn, J., Ostelo, R., Bartels, R., et al., 2010. Transforaminal endoscopic surgery for symptomatic lumbar disc herniations: a systematic review of the literature. Eur. Spine J., 19(2):181–204. http://dx.doi.org/10.1007/s00586-009-1155-x
Reulen, H.J., Muller, A., Ebeling, U., 1996. Microsurgical anatomy of the lateral approach to extraforaminal lumbar disc herniations. Neurosurgery, 39(2):345–350, discussion 350–351.
Ruetten, S., Komp, M., Merk, H., et al., 2007. Use of newly developed instruments and endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J. Neurosurg. Spine, 6(6):521–530. http://dx.doi.org/10.3171/spi.2007.6.6.2
Sairyo, K., Matsuura, T., Higashino, K., et al., 2014. Surgery related complications in percutaneous endoscopic lumbar discectomy under local anesthesia. J. Med. Invest., 61(3–4):264–269. http://dx.doi.org/10.2152/jmi.61.264
Sanderson, S.P., Houten, J., Errico, T., et al., 2004. The unique characteristics of “upper” lumbar disc herniations. Neurosurgery, 55(2):385–389, discussion 389.
Wang, B., Lü, G., Patel, A.A., et al., 2011. An evaluation of the learning curve for a complex surgical technique: the full endoscopic interlaminar approach for lumbar disc herniations. Spine J., 11(2):122–130. http://dx.doi.org/10.1016/j.spinee.2010.12.006
Wang, H., Huang, B., Li, C., et al., 2013. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon’s training level of minimally invasive spine surgery. Clin. Neurol. Neurosurg., 115(10):1987–1991. http://dx.doi.org/10.1016/j.clineuro.2013.06.008
Author information
Authors and Affiliations
Corresponding authors
Additional information
The two authors contributed equally to this work
ORCID: Xin-bo WU, http://orcid.org/0000-0002-9846-2857
Rights and permissions
About this article

Cite this article
Wu, Xb., Fan, Gx., Gu, X. et al. Learning curves of percutaneous endoscopic lumbar discectomy in transforaminal approach at the L4/5 and L5/S1 levels: a comparative study. J. Zhejiang Univ. Sci. B 17, 553–560 (2016). https://doi.org/10.1631/jzus.B1600002
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1631/jzus.B1600002