Chronic Kidney Disease-Associated Inflammation Increases the Risks of Acute Kidney Injury and Mortality after Cardiac Surgery

 , , , and
, , , and 
Abstract
:1. Introduction
2. Results
2.1. CKD Is Associated with Increased Risk of Cardiac Surgery–Associated Acute Kidney Injury (CSA-AKI) and 30-Day Mortality after Cardiac Surgery Cardiovascular Outcome
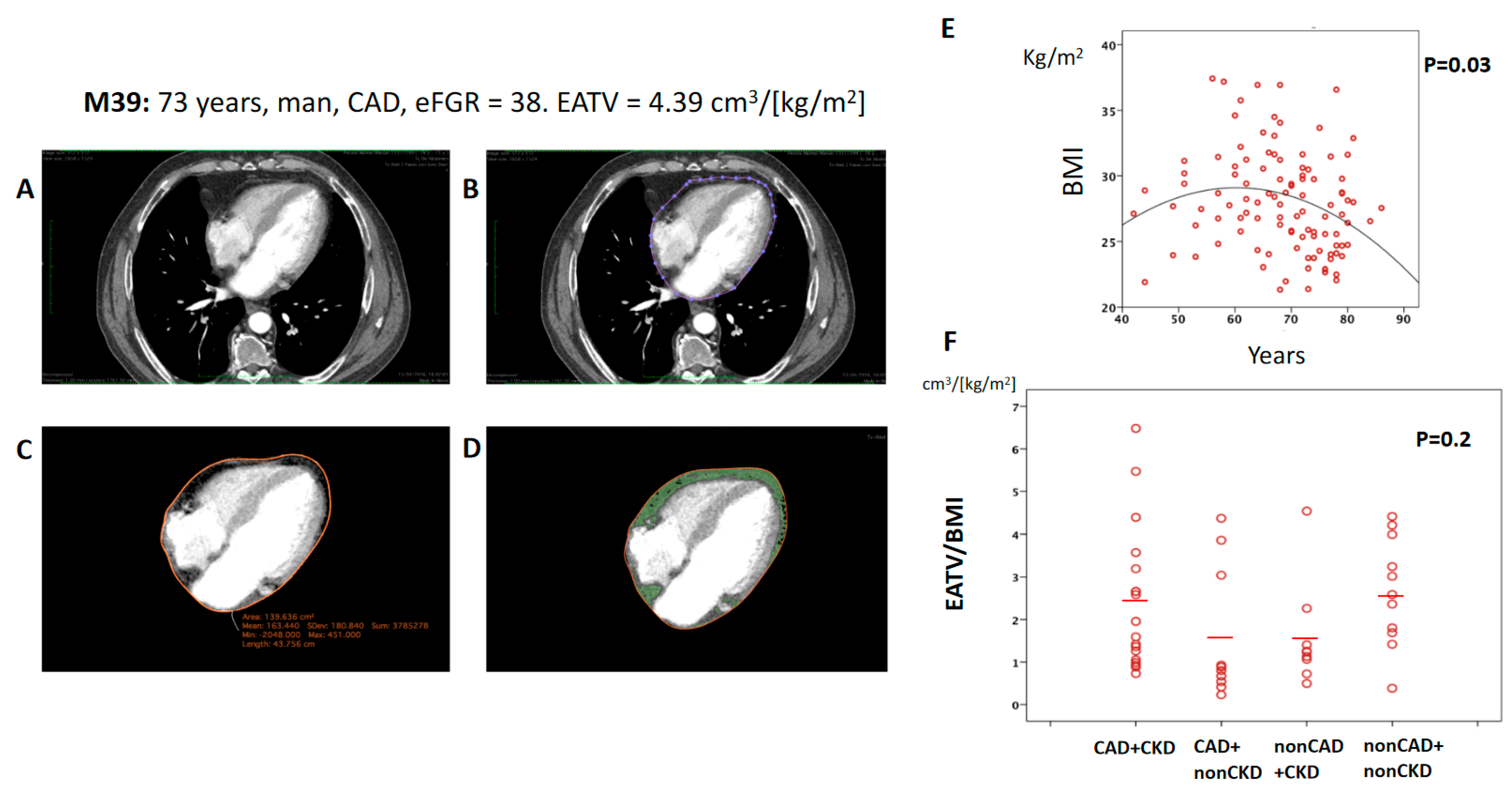
2.2. CKD Was Not Associated with an Increase in Total Volume of Epicardial Adipose Tissue (EATV)
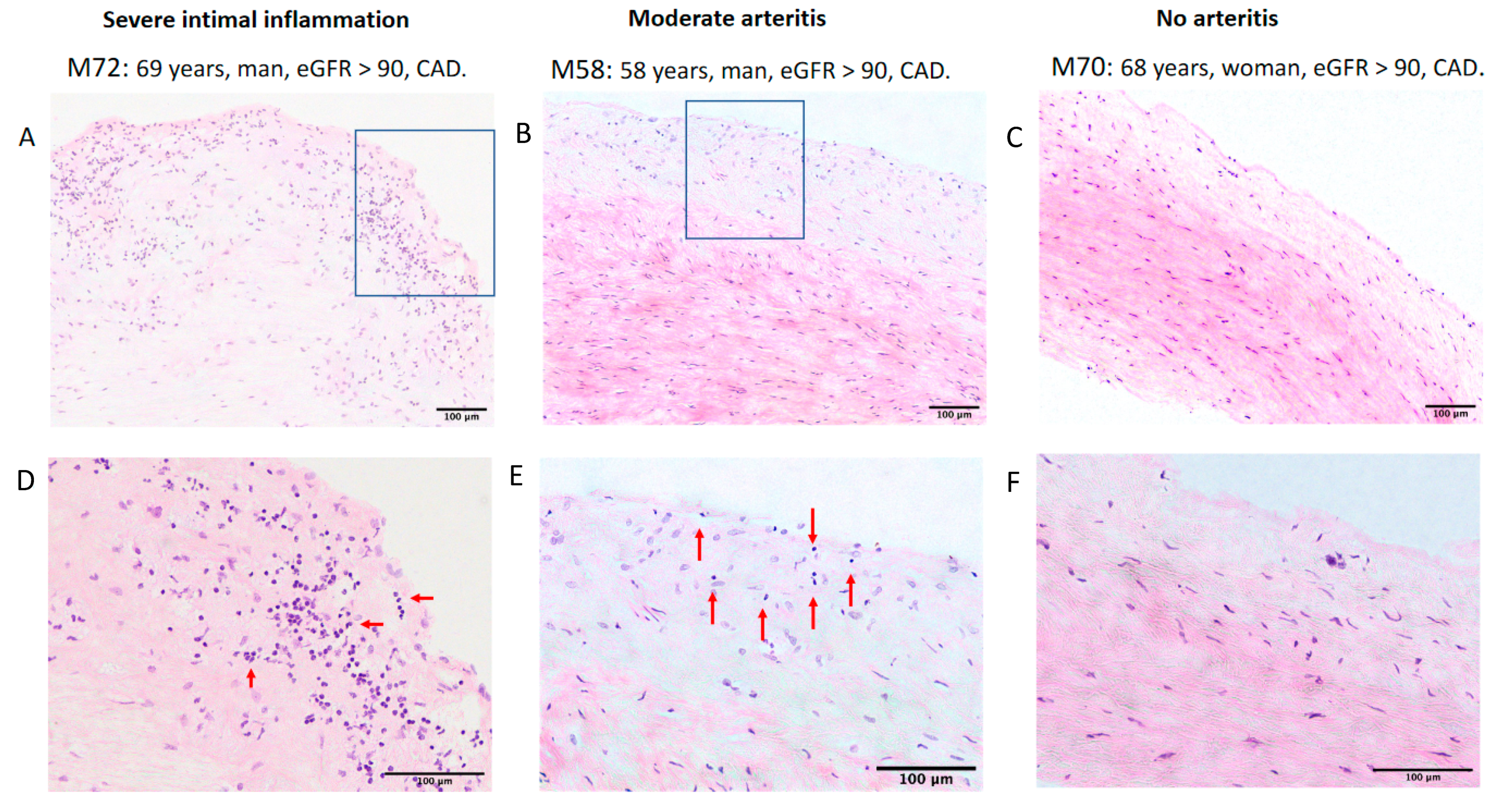
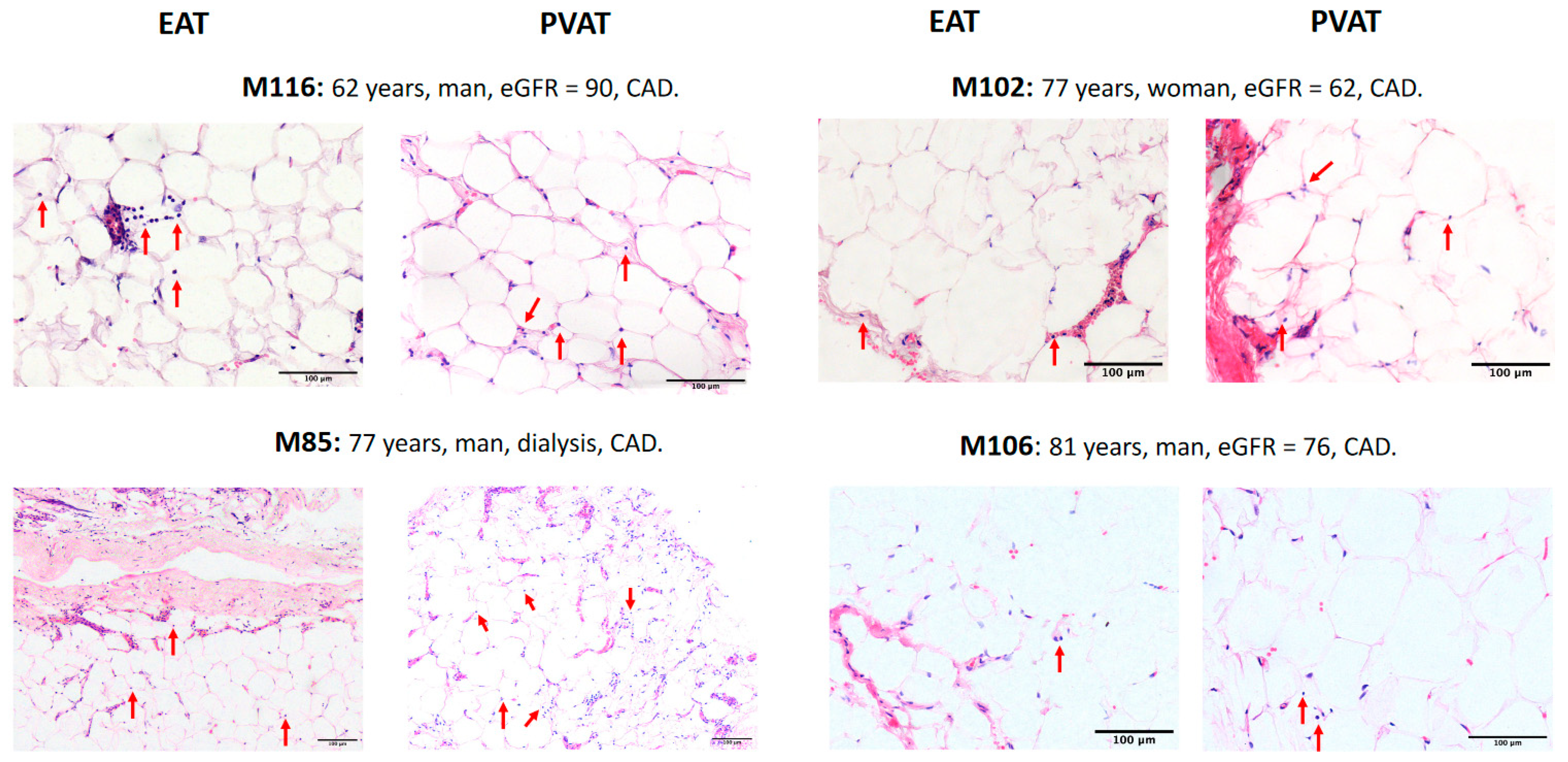
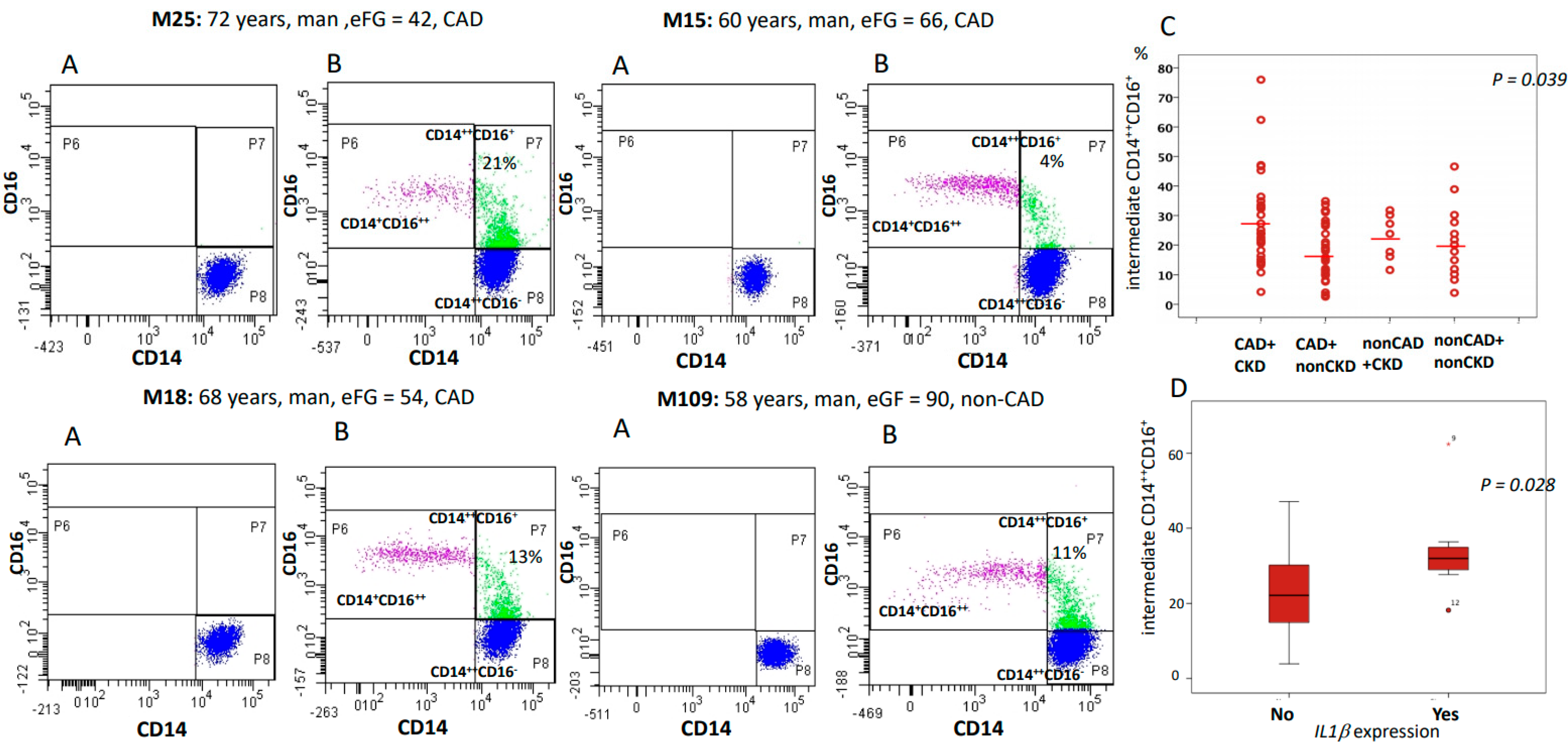
2.3. CKD Was Associated with the Increased Expression of Inflammatory Markers and with a Higher Proportion of Intermediate CD14++CD16+ Monocytes
3. Discussion
- CKD patients with severe CAD disease have higher susceptibility to acute kidney injury (CSA-AKI) and death after CABG surgery and require a deep evaluation prior to heart surgery.
- The inflammation associated with CKD maybe one of the mechanisms responsible for the increase in the mortality of these patients.
4. Materials and Methods
4.1. Subjects
4.2. Definition of Variables
4.3. Reagents
- IL1α (Hs_00174092_m1),
- IL6 (Hs_00174131_m1),
- TNFα(Hs_00174129_m1),
- CCR5 (Hs_00152917_m1),
- Cx3CR1 (Hs_01922583_m1),
- MAPK1 (Hs_01046830_m1),
- MAP2K1 (Hs_05512159_s1),
- MAPK9 (Hs_01558224_m1)
- ACTIN (Hs_01060665-g1)
- hsa_miR30a-5p (Assay ID:000417)
- hsa-miR16-3p (Assay ID:002171), and
- cel-miR-54-3p (Assay ID:001361).
4.4. Measurement of the Epicardial Adipose Tissue Volume (EATV)
4.5. Specimen Details
4.6. Measurement of Adipocyte Size and Inflammation
4.7. Flow Cytometry Analysis
4.8. Identification Strategy of Monocyte Subsets
4.9. Total RNA Isolation and Quantitative Real-Time PCR
4.10. Statistics
5. Conclusions
- CKD is a risk factor for CSA-AKI and death after cardiac surgery.
- CKD patients with CAD present a proinflammatory environment that can be detected in the blood (increased C-reactive protein, fibrinogen levels, intermediate CD14++CD16+ monocytes, and IL1β) and could be useful to stratify the cardiovascular risk of patients with CKD.
- We suggest a link between microvascular network density and inflammation since we observed a link between has-miR30a-5p and IL1β expression.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ATH | Atherosclerosis |
| CABG | Coronary Artery Bypass Graft |
| CAD | Coronary Arterial Disease |
| CKD | Chronic Kidney Disease |
| CSA-AKI | Cardiac Surgery–Associated Acute Kidney Injury |
| EATV | Epicardial Adipose Tissue Volume |
| eGFR | estimated Glomerular Filtration Rate |
| FSC | Forward Scatter |
| ITD | Intermediate CD14++CD16+ monocytes |
| LPS | Lipopolysaccharide |
| MAP | Mitogen-Activated Protein Kinase |
| NK | Natural Killer cells |
| NKT | Natural Killer T cells |
| PBMCs | Peripheral Blood Mononuclear Cells |
| PVAT | Perivascular Adipose Tissue |
| SSC | Side Scatter |
References
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Tonelli, M.; Wiebe, N.; Culleton, B.; House, A.; Rabbat, C.; Fok, M.; McAlister, F.; Garg, A.X. Chronic Kidney Disease and Mortality Risk: A Systematic Review. J. Am. Soc. Nephrol. 2006, 17, 2034–2047. [Google Scholar] [CrossRef] [Green Version]
- Stenvinkel, P.; Pecoits-Filho, R.; Lindholm, B. Coronary Artery Disease in End-Stage Renal Disease: No Longer a Simple Plumbing Problem. J. Am. Soc. Nephrol. 2003, 14, 1927–1939. [Google Scholar] [CrossRef] [Green Version]
- Packard, R.R.S.; Libby, P. Inflammation in Atherosclerosis: From Vascular Biology to Biomarker Discovery and Risk Prediction. Clin. Chem. 2008, 54, 24–38. [Google Scholar] [CrossRef] [Green Version]
- Massy, Z.A.; Ivanovski, O.; Nguyen-Khoa, T.; Angulo, J.; Szumilak, D.; Mothu, N.; Phan, O.; Daudon, M.; Lacour, B.; Drüeke, T.B.; et al. Uremia Accelerates both Atherosclerosis and Arterial Calcification in Apolipoprotein E Knockout Mice. J. Am. Soc. Nephrol. 2004, 16, 109–116. [Google Scholar] [CrossRef]
- Hueso, M.; De Ramon, L.; Navarro, E.; Ripoll, E.; Cruzado, J.M.; Grinyo, J.M.; Torras, J. Silencing of CD40 in vivo reduces progression of experimental atherogenesis through an NF-κB/miR-125b axis and reveals new potential mediators in the pathogenesis of atherosclerosis. Atherosclerosis 2016, 255, 80–89. [Google Scholar] [CrossRef]
- Heine, G.H.; Ulrich, C.M.; Seibert, E.; Seiler, S.; Marell, J.; Reichart, B.; Krause, M.; Schlitt, A.; Köhler, H.; Girndt, M. CD14++CD16+ monocytes but not total monocyte numbers predict cardiovascular events in dialysis patients. Kidney Int. 2008, 73, 622–629. [Google Scholar] [CrossRef] [Green Version]
- Hueso, M.; Torras, J.; Carrera, M.; Vidal, A.A.; Navarro, E.; Grinyó, J.M. Chronic Kidney Disease is associated with an increase of Intimal Dendritic cells in a comparative autopsy study. J. Inflamm. 2015, 12, 26. [Google Scholar] [CrossRef] [Green Version]
- Rogacev, K.S.; Cremers, B.; Zawada, A.M.; Seiler, S.; Binder, N.; Ege, P.; Große-Dunker, G.; Heisel, I.; Hornof, F.; Jeken, J.; et al. CD14++CD16+ monocytes independently predict cardiovascular events: A cohort study of 951 patients referred for elective coronary angiography. J. Am. Coll. Cardiol. 2012, 60, 1512–1520. [Google Scholar] [CrossRef] [Green Version]
- Tacke, F.; Alvarez, D.; Kaplan, T.J.; Jakubzick, C.; Spanbroek, R.; Llodra, J.; Garin, A.; Liu, J.; Mack, M.; Van Rooijen, N.; et al. Monocyte subsets differentially employ CCR2, CCR5, and CX3CR1 to accumulate within atherosclerotic plaques. J. Clin. Investig. 2007, 117, 185–194. [Google Scholar] [CrossRef] [Green Version]
- Ziegler-Heitbrock, L.; Ancuta, P.; Crowe, S.; Dalod, M.; Grau, V.; Hart, D.N.; Leenen, P.J.M.; Liu, Y.-J.; MacPherson, G.; Randolph, G.J.; et al. Nomenclature of monocytes and dendritic cells in blood. Blood 2010, 116, e74–e80. [Google Scholar] [CrossRef]
- Hijdra, D.; Platteel, A.C.; Grutters, J.C.; Claessen, A.M.E.; Rijkers, G.T. Phenotypic Characterization of Human Intermediate Monocytes. Front. Immunol. 2013, 4, 339. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Hofer, T.P.; Zawada, A.M.; Rotter, B.; Krezdorn, N.; Noessner, E.; Devaux, Y.; Heine, G.; Eziegler-Heitbrock, L. Epigenetics in non-classical monocytes support their pro-inflammatory gene expression. Immunobiology 2020, 225, 151958. [Google Scholar] [CrossRef]
- Rogacev, K.S.; Seiler, S.; Zawada, A.M.; Reichart, B.; Herath, E.; Roth, D.; Ulrich, C.; Fliser, D.; Heine, G.H. CD14++CD16+ monocytes and cardiovascular outcome in patients with chronic kidney disease. Eur. Hear. J. 2010, 32, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Rosito, G.A.; Massaro, J.M.; Hoffmann, U.; Ruberg, F.L.; Mahabadi, A.A.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample: The Framingham Heart Study. Circulation 2008, 117, 605–613. [Google Scholar] [CrossRef] [Green Version]
- Silaghi, A.; Piercecchi-Marti, M.-D.; Grino, M.; Leonetti, G.; Alessi, M.C.; Clement, K.; Dadoun, F.; Dutour, A. Epicardial Adipose Tissue Extent: Relationship With Age, Body Fat Distribution, and Coronaropathy. Obesity 2008, 16, 2424–2430. [Google Scholar] [CrossRef]
- Libby, P. Interleukin-1 Beta as a Target for Atherosclerosis Therapy. J. Am. Coll. Cardiol. 2017, 70, 2278–2289. [Google Scholar] [CrossRef]
- Jiang, Q.; Lagos-Quintana, M.; Liu, D.; Shi, Y.; Helker, C.; Herzog, W.; Le Noble, F. miR-30a Regulates Endothelial Tip Cell Formation and Arteriolar Branching. Hypertension 2013, 62, 592–598. [Google Scholar] [CrossRef] [Green Version]
- James, M.T.; Grams, M.E.; Woodward, M.; Elley, C.R.; Green, J.A.; Wheeler, D.C.; de Jong, P.; Gansevoort, R.T.; Levey, A.S.; Warnock, D.G.; et al. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Diabetes Mellitus, and Hypertension with Acute Kidney Injury. Am. J. Kidney Dis. 2015, 66, 602–612. [Google Scholar] [CrossRef] [Green Version]
- Matsuura, R.; Iwagami, M.; Moriya, H.; Ohtake, T.; Hamasaki, Y.; Nangaku, M.; Doi, K.; Kobayashi, S.; Noiri, E. The Clinical Course of Acute Kidney Disease after Cardiac Surgery: A Retrospective Observational Study. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Vives, M.; Hernandez, A.; Parramon, F.; Estanyol, N.; Pardina, B.; Muñoz, A.; Alvarez, P.; Hernandez, C. Acute kidney injury after cardiac surgery: Prevalence, impact and management challenges. Int. J. Nephrol. Renov. Dis. 2019, 12, 153–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coca, S.G.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and meta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, V.C.; Huang, T.M.; Lai, C.F.; Shiao, C.C.; Lin, Y.F.; Chu, T.S.; Wu, P.C.; Chao, C.T.; Wang, J.Y.; Kao, T.W.; et al. Acute-on-chronic kidney injury at hospital discharge is associated with long-term dialysis and mortality. Kidney Int. 2011, 80, 1222–1230. [Google Scholar] [CrossRef] [Green Version]
- Tonelli, M.; Sacks, F.; Pfeffer, M.; Jhangri, G.S.; Curhan, G. Biomarkers of inflammation and progression of chronic kidney disease. Kidney Int. 2005, 68, 237–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leelahavanichkul, A.; Huang, Y.; Hu, X.; Zhou, H.; Tsuji, T.; Chen, R.; Kopp, J.B.; Schnermann, J.; Yuen, P.S.; Star, R.A. Chronic kidney disease worsens sepsis and sepsis-induced acute kidney injury by releasing High Mobility Group Box Protein-1. Kidney Int. 2011, 80, 1198–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, L.; Wei, Q.; Liu, J.; Yi, M.; Liu, Y.; Liu, H.; Sun, L.; Peng, Y.; Liu, F.; Venkatachalam, M.A.; et al. AKI on CKD: Heightened injury, suppressed repair, and the underlying mechanisms. Kidney Int. 2017, 92, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- Pugh, D.; Gallacher, P.J.; Dhaun, N. Management of Hypertension in Chronic Kidney Disease. Drugs 2019, 79, 365–379. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Iturbe, B.; Pons, H.; Johnson, R.J. Role of the Immune System in Hypertension. Physiol. Rev. 2017, 97, 1127–1164. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Heimbürger, O.; Paultre, F.; Diczfalusy, U.; Wang, T.; Berglund, L.; Jogestrand, T. Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure. Kidney Int. 1999, 55, 1899–1911. [Google Scholar] [CrossRef] [Green Version]
- Loperena, R.; Van Beusecum, J.P.; Itani, A.; Engel, H.; Laroumanie, N.; Xiao, F.; Elijovich, L.; Laffer, F.; Gnecco, C.L.; Noonan, J.S.; et al. Hypertension and increased endothelial mechanical stretch promote monocyte differentiation and activation: Roles of STAT3, interleukin 6 and hydrogen peroxide. Cardiovasc. Res. 2018, 114, 1547–1563. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Polichnowski, A.J.; Lan, R.; Geng, H.; Griffin, K.A.; Venkatachalam, M.A.; Bidani, A.K. Severe renal mass reduction impairs recovery and promotes fibrosis after AKI. J. Am. Soc. Nephrol. 2014, 25, 1496–1507. [Google Scholar] [CrossRef] [Green Version]
- Picken, M.; Long, J.; Williamson, G.A.; Polichnowski, A.J. Progression of Chronic Kidney Disease after Acute Kidney Injury: Role of Self-Perpetuating Versus Hemodynamic-Induced Fibrosis. Hypertension 2016, 68, 921–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hueso, M.; Casas, A.; Mallén, A.; De Ramón, L.; Bolaños, N.; Varela, C.; Cruzado, J.M.; Torras, J.; Navarro, E. The double edge of anti-CD40 siRNA therapy: It increases renal microcapillar density but favours the generation of an inflammatory milieu in the kidneys of ApoE−/− mice. J. Inflamm. 2019, 16, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishizawa, A.; Suemoto, C.K.; Farias-Itao, D.S.; Campos, F.M.; Silva, K.C.S.; Bittencourt, M.S.; Grinberg, L.T.; Leite, R.E.P.; Ferretti-Rebustini, R.E.L.; Farfel, J.M.; et al. Morphometric measurements of systemic atherosclerosis and visceral fat: Evidence from an autopsy study. PLoS ONE 2017, 12, e0186630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merah-Mourah, F.; Cohen, S.O.; Charron, D.; Mooney, N.; Haziot, A. Identification of Novel Human Monocyte Subsets and Evidence for Phenotypic Groups Defined by Interindividual Variations of Expression of Adhesion Molecules. Sci. Rep. 2020, 10, 4397. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Levey, A.S.; Eckardt, K.-U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; Zeeuw, D.D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef] [Green Version]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Abeles, R.D.; McPhail, M.J.; Sowter, D.; Antoniades, C.G.; Vergis, N.; Vijay, G.K.; Xystrakis, E.; Khamri, W.; Shawcross, D.L.; Ma, Y.; et al. CD14, CD16 and HLA-DR reliably identifies human monocytes and their subsets in the context of pathologically reduced HLA-DR expression by CD14(hi) /CD16(neg) monocytes: Expansion of CD14(hi) /CD16(pos) and contraction of CD14(lo) /CD16(pos) monocytes in acute liver failure. Cytom. A 2012, 81, 823–834. [Google Scholar]
- Marimuthu, R.; Francis, H.; Dervish, S.; Li, S.C.; Medbury, H.; Williams, H. Characterization of Human Monocyte Subsets by Whole Blood Flow Cytometry Analysis. J. Vis. Exp. 2018, 2018, e57941. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CAD + CKD | CAD + NonCKD | NonCAD + CKD | NonCAD + NonCKD | p | |
|---|---|---|---|---|---|
| n | 51 | 59 | 15 | 26 | |
| Gender (F/M) | 12/39 | 13/46 | 3/12 | 9/17 | 0.6 |
| Age (years) | 70 (10) | 66(9) | 71 (9) | 63 (10) | 0.003 |
| BMI (kg/m2) | 27.8 (4) | 28.3 (3) | 29.1 (4) | 29 (5) | 0.6 |
| Cr (µmol/L) | 239 (212) | 81 (14) | 192 (171) | 73 (15) | 0.0001 |
| Diabetes (yes/no) | 32/19 | 32/27 | 5/10 | 9/17 | 0.05 |
| Cholesterol (mmol/L) | 4.1 (1.5) | 4.2 (1.4) | 4.5 (1.4) | 4.8 (1.2) | 0.14 |
| Triglycerides | 1.9 (1.1) | 2.03 (0.9) | 2.03 (0.9) | 2.9 (2.05) | 0.25 |
| SBP (mmHg) | 129 (21) | 123 (13) | 121 (20) | 119 (11) | 0.02 |
| DBP (mmHg) | 70 (9) | 69 (10) | 69 (11) | 68 (9) | 0.6 |
| CAD + CKD | CAD + NonCKD | NonCAD + CKD | NonCAD + NonCKD | p | |
|---|---|---|---|---|---|
| n | 27 | 30 | 7 | 13 | |
| CD14++CD16− | 65.0 (17.8) | 71.2 (12.5) | 71.0 (7.7) | 72.1 (13.2) | 0.25 |
| CD14++CD16+ | 28.2 (16.1) | 18.5 (9.8) | 22.6 (7.6) | 21.2 (12.2) | 0.039 |
| CD14+CD16++ | 6.8 (3.9) | 10.3 (9.1) | 6.4 (6.2) | 6.7 (6.6) | 0.14 |
| CD16+ | 35 (15.6) | 28.8 (12.7) | 29 (7.8) | 28 (15.2) | 0.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casas, A.; Mallén, A.; Blasco-Lucas, A.; Sbraga, F.; Guiteras, J.; Bolaños, N.; Castaño, E.; Torras, J.; Cruzado, J.M.; Navarro, E.; et al. Chronic Kidney Disease-Associated Inflammation Increases the Risks of Acute Kidney Injury and Mortality after Cardiac Surgery. Int. J. Mol. Sci. 2020, 21, 9689. https://doi.org/10.3390/ijms21249689
Casas A, Mallén A, Blasco-Lucas A, Sbraga F, Guiteras J, Bolaños N, Castaño E, Torras J, Cruzado JM, Navarro E, et al. Chronic Kidney Disease-Associated Inflammation Increases the Risks of Acute Kidney Injury and Mortality after Cardiac Surgery. International Journal of Molecular Sciences. 2020; 21(24):9689. https://doi.org/10.3390/ijms21249689
Chicago/Turabian StyleCasas, Angela, Adrián Mallén, Arnau Blasco-Lucas, Fabrizio Sbraga, Jordi Guiteras, Núria Bolaños, Esther Castaño, Joan Torras, Josep M. Cruzado, Estanislao Navarro, and et al. 2020. "Chronic Kidney Disease-Associated Inflammation Increases the Risks of Acute Kidney Injury and Mortality after Cardiac Surgery" International Journal of Molecular Sciences 21, no. 24: 9689. https://doi.org/10.3390/ijms21249689