
Morbidity and Mortality in Patients over 90 Years of Age Following Posterior Stabilization for Acute Traumatic Odontoid Type II Fractures: A Retrospective Study with a Mean Follow-Up of Three Years

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
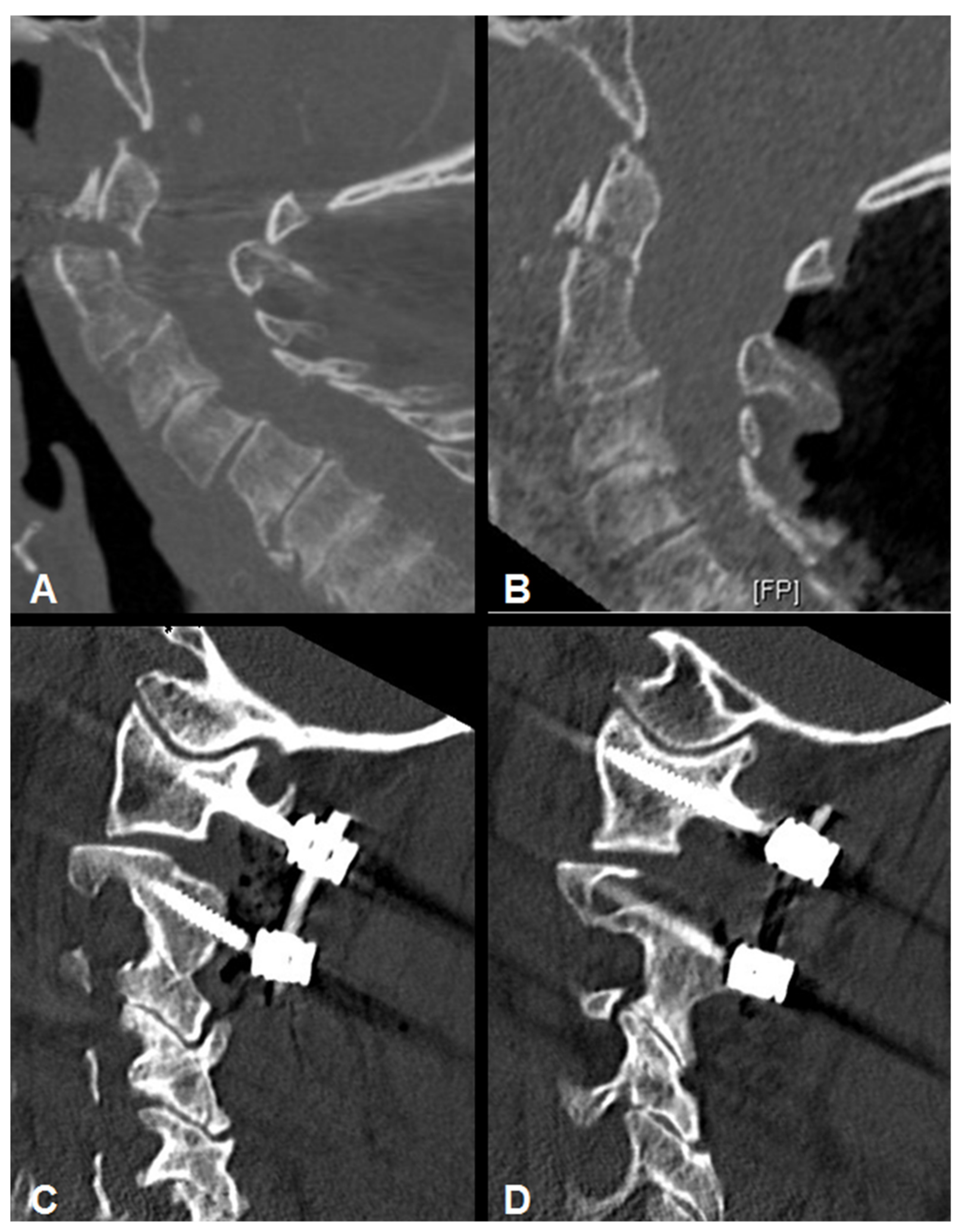
2.2. Surgical Technique
2.3. Outcome Parameters
2.4. Comparison of Complication Rates with Patients under 90 Years of Age
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Mortality
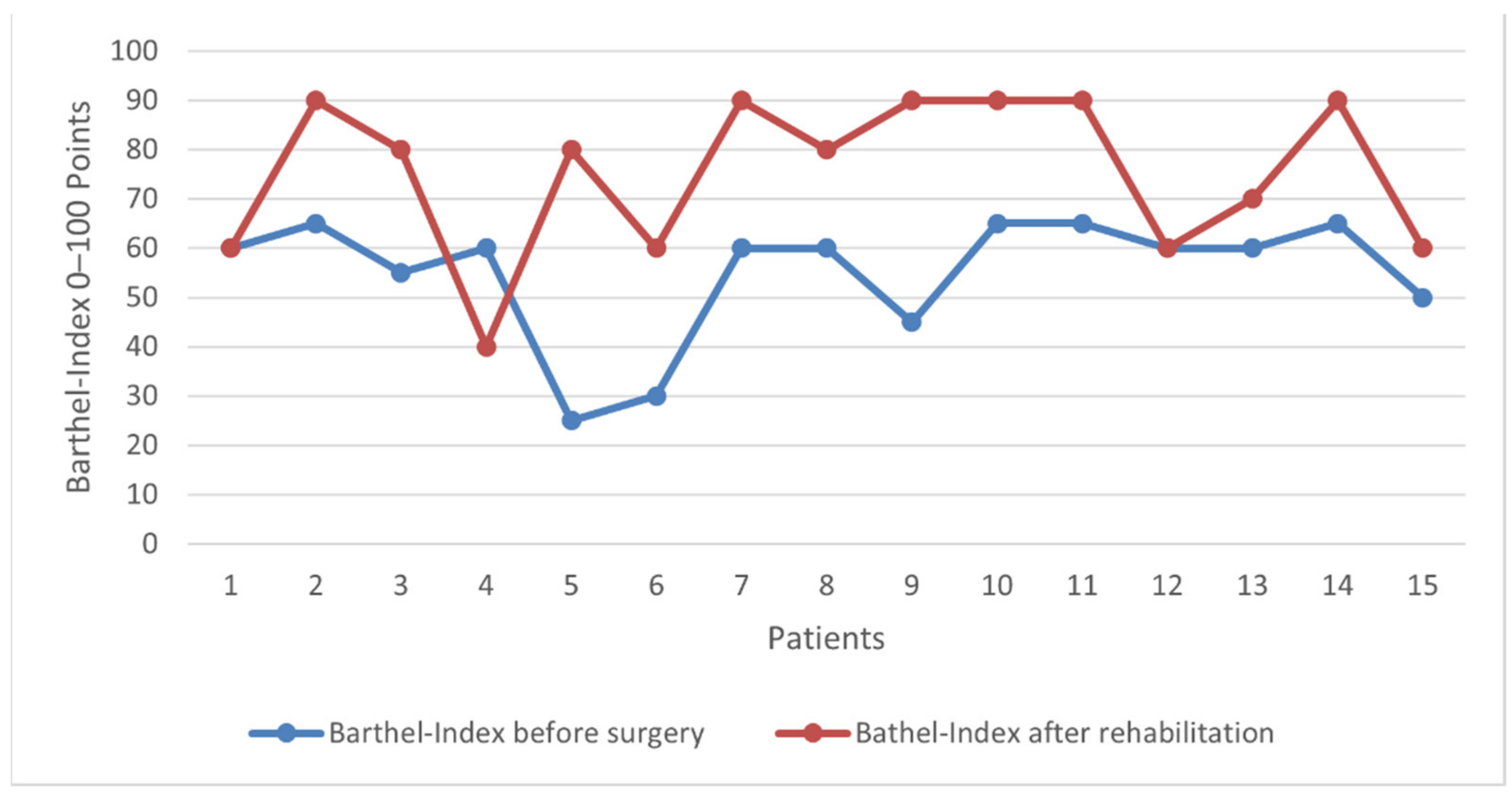
3.3. Clinical and Functional Characteristics
3.4. Radiographic Results
3.5. Complications and Perioperative Course
3.6. Comparison of Complication Rates with Patients under 90 Years of Age
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kobayashi, K.; Imagama, S.; Sato, K.; Kato, F.; Kanemura, T.; Yoshihara, H.; Sakai, Y.; Shinjo, R.; Hachiya, Y.; Osawa, Y.; et al. Postoperative Complications Associated with Spine Surgery in Patients Older Than 90 Years: A Multicenter Retrospective Study. Glob. Spine J. 2018, 8, 887–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berlau, D.J.; Corrada, M.M.; Kawas, C. The prevalence of disability in the oldest-old is high and continues to increase with age: Findings from the 90+ Study. Int. J. Geriatr. Psychiatry 2009, 24, 1217–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lotan, R.; Smorgick, Y.; Anekstein, Y.; Rudik, O.; Prosso, I.; Hershkovich, O. Kyphoplasty for Elderly Patients with Vertebral Compression Fractures-Do We Save Lives? Mortality Rates Analysis Comparison in a Long-Term Follow-Up Cohort. Glob. Spine J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jeanmonod, R.; Varacallo, M. Geriatric Cervical Spine Injury; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Malik, S.; Murphy, M.; Connolly, P.; O’Byrne, J. Evaluation of morbidity, mortality and outcome following cervical spine injuries in elderly patients. Eur. Spine J. 2008, 17, 585–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishak, B.; Dupont, G.; Lachkar, S.; Yilmaz, E.; Von Glinski, A.; Altafulla, J.; Kikuta, S.; Iwanaga, J.; Chapman, J.R.; Oskouian, R.; et al. Update on the Biomechanics of the Craniocervical Junction-Part I: Transverse Atlantal Ligament in the Elderly. Glob. Spine J. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishak, B.; Schneider, T.; Gimmy, V.; Unterberg, A.W.; Kiening, K.L. Early complications, morbidity, and mortality in octogenarians and nonagenarians undergoing posterior intra-operative spinal navigation-based C1/2 fusion for type II odontoid process fractures. J. Neurotrauma 2017, 34, 3326–3335. [Google Scholar] [CrossRef]
- Ryang, Y.-M.; Török, E.; Janssen, I.; Reinke, A.; Buchmann, N.; Gempt, J.; Ringel, F.; Meyer, B. Early morbidity and mortality in 50 very elderly patients after posterior atlantoaxial fusion for traumatic odontoid fractures. World Neurosurg. 2016, 87, 381–391. [Google Scholar] [CrossRef]
- Pommier, B.; Ollier, E.; Pelletier, J.B.; Castel, X.; Vassal, F.; Tetard, M.C. Conservative versus Surgical Treatment for Odontoid Fracture: Is the Surgical Treatment Harmful? Systematic Review and Meta-Analysis. World Neurosurg. 2020, 141, 490–499. [Google Scholar] [CrossRef]
- Gembruch, O.; Lemonas, E.; Ahmadipour, Y.; Sure, U.; El Hindy, N.; Dodel, R.; Muller, O. Treatment of Odontoid Type II Fractures in Octogenarians: Balancing Two Different Treatment Strategies. Neurospine 2019, 16, 360–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tashjian, R.Z.; Majercik, S.; Biffl, W.L.; Palumbo, M.A.; Cioffi, W.G. Halo-vest immobilization increases early morbidity and mortality in elderly odontoid fractures. J. Trauma Acute Care Surg. 2006, 60, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Majercik, S.; Tashjian, R.Z.; Biffl, W.L.; Harrington, D.T.; Cioffi, W.G. Halo vest immobilization in the elderly: A death sentence? J. Trauma Acute Care Surg. 2005, 59, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.; Smith, J.S.; Kopjar, B.; Vaccaro, A.R.; Arnold, P.; Shaffrey, C.I.; Fehlings, M.G. The AOSpine North America Geriatric Odontoid Fracture Mortality Study: A retrospective review of mortality outcomes for operative versus nonoperative treatment of 322 patients with long-term follow-up. Spine 2013, 38, 1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fehlings, M.G.; Arun, R.; Vaccaro, A.R.; Arnold, P.M.; Chapman, J.R.; Kopjar, B. Predictors of treatment outcomes in geriatric patients with odontoid fractures: AOSpine North America multi-centre prospective GOF study. Spine 2013, 38, 881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarode, D.P.; Demetriades, A.K. Surgical versus nonsurgical management for type II odontoid fractures in the elderly population: A systematic review. Spine J. 2018, 18, 1921–1933. [Google Scholar] [CrossRef] [PubMed]
- Ishak, B.; Schneider, T.; Gimmy, V.; Unterberg, A.W.; Kiening, K.L. A Modified Posterior C1/C2 Fusion Technique for the Management of Traumatic Odontoid Type II Fractures by Using Intraoperative Spinal Navigation: Midterm Results. J. Orthop. Trauma 2018, 32, e366–e371. [Google Scholar] [CrossRef]
- Ishak, B.; Schneider, T.; Tubbs, R.S.; Gimmy, V.; Younsi, A.; Unterberg, A.W.; Kiening, K.L. Modified Posterior C1 Lateral Mass Screw Insertion for Type II Odontoid Process Fractures Using Intraoperative Computed Tomography–Based Spinal Navigation to Minimize Postoperative Occipital Neuralgia. World Neurosurg. 2017, 107, 194–201. [Google Scholar] [CrossRef]
- Moisi, M.; Fisahn, C.; Tkachenko, L.; Jeyamohan, S.; Reintjes, S.; Grunert, P.; Norvell, D.C.; Tubbs, R.S.; Page, J.; Newell, D.W.; et al. Posterior arch C-1 screw technique: A cadaveric comparison study. J. Neurosurg. Spine 2017, 26, 679–683. [Google Scholar] [CrossRef]
- Harms, J.; Melcher, R.P. Posterior C1–C2 fusion with polyaxial screw and rod fixation. Spine 2001, 26, 2467–2471. [Google Scholar] [CrossRef] [PubMed]
- Ishak, B.; Younsi, A.; Wieckhusen, C.; Slonczewski, P.; Unterberg, A.W.; Kiening, K.L. Accuracy and revision rate of intraoperative computed tomography point-to-point navigation for lateral mass and pedicle screw placement: 11-year single-center experience in 1054 patients. Neurosurg. Rev. 2019, 42, 895–905. [Google Scholar] [CrossRef]
- De Groot, V.; Beckerman, H.; Lankhorst, G.J.; Bouter, L.M. How to measure comorbidity: A critical review of available methods. J. Clin. Epidemiol. 2003, 56, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index: A simple index of independence useful in scoring improvement in the rehabilitation of the chronically ill. Md. State Med J. 1965, 14, 61–65. [Google Scholar]
- Robinson, A.-L.; Olerud, C.; Robinson, Y. Epidemiology of C2 fractures in the 21st century: A national registry cohort study of 6370 patients from 1997 to 2014. Adv. Orthop. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. Department of Economic and Social Affairs, Population Division World Population Ageing 2013; United Nations: New York, NY, USA, 2013. [Google Scholar]
- Greene, K.A.; Dickman, C.A.; Marciano, F.F.; Drabier, J.B.; Hadley, M.N.; Sonntag, V.K. Acute axis fractures: Analysis of management and outcome in 340 consecutive cases. Spine 1997, 22, 1843–1852. [Google Scholar] [CrossRef]
- Ryan, M.; Henderson, J. The epidemiology of fractures and fracture-dislocations of the cervical spine. Injury 1992, 23, 38–40. [Google Scholar] [CrossRef]
- Molinari, R.W.; Dahl, J.; Gruhn, W.L.; Molinari, W.J. Functional outcomes, morbidity, mortality, and fracture healing in 26 consecutive geriatric odontoid fracture patients treated with posterior fusion. Clin. Spine Surg. 2013, 26, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Horn, E.M.; Theodore, N.; Feiz-Erfan, I.; Lekovic, G.P.; Dickman, C.A.; Sonntag, V.K. Complications of halo fixation in the elderly. J. Neurosurg. Spine 2006, 5, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Isidro, S.; Molinari, R.; Ikpeze, T.; Hernandez, C.; Mahmoudi, M.S.; Mesfin, A. Outcomes of Halo Immobilization for Cervical Spine Fractures. Glob. Spine J. 2019, 9, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Bono, C.M. The halo fixator. JAAOS-J. Am. Acad. Orthop. Surg. 2007, 15, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, J.P.; Magnotti, L.J.; Weinberg, J.A.; Schroeppel, T.J.; Fabian, T.C.; Croce, M.A. The old man and the C-spine fracture: Impact of halo vest stabilization in patients with blunt cervical spine fractures. J. Trauma Acute Care Surg. 2016, 80, 76–80. [Google Scholar] [CrossRef] [PubMed]
- DePasse, J.M.; Palumbo, M.A.; Ahmed, A.-K.; Adams, C.A.; Daniels, A.H. Halo-Vest Immobilization in Elderly Odontoid Fracture Patients. Clin. Spine Surg. 2017, 30, E1206–E1210. [Google Scholar] [CrossRef] [PubMed]
- Julien, T.D.; Frankel, B.; Traynelis, V.C.; Ryken, T.C. Evidence-based analysis of odontoid fracture management. Neurosurg. Focus 2000, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Polin, R.S.; Szabo, T.; Bogaev, C.A.; Replogle, R.E.; Jane, J.A. Nonoperative management of types II and III odontoid fractures: The Philadelphia collar versus the halo vest. Neurosurgery 1996, 38, 450–457. [Google Scholar] [PubMed]
- Koivikko, M.; Kiuru, M.J.; Koskinen, S.K.; Myllynen, P.; Santavirta, S.; Kivisaari, L. Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J. Bone Jt. Surg. 2004, 86, 1146–1151. [Google Scholar] [CrossRef]
- Seybold, E.A.; Bayley, J.C. Functional outcome of surgically and conservatively managed dens fractures. Spine 1998, 23, 1837–1845. [Google Scholar] [CrossRef] [PubMed]
- Raudenbush, B.; Molinari, R. Longer-term outcomes of geriatric odontoid fracture nonunion. Geriatr. Orthop. Surg. Rehabil. 2015, 6, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Smith, H.E.; Kerr, S.M.; Maltenfort, M.; Chaudhry, S.; Norton, R.; Albert, T.J.; Harrop, J.; Hilibrand, A.S.; Anderson, D.G.; Kopjar, B. Early complications of surgical versus conservative treatment of isolated type II odontoid fractures in octogenarians: A retrospective cohort study. Clin. Spine Surg. 2008, 21, 535–539. [Google Scholar] [CrossRef]
- Fagin, A.M.; Cipolle, M.D.; Barraco, R.D.; Eid, S.; Reed III, J.F.; Li, P.M.; Pasquale, M.D. Odontoid fractures in the elderly: Should we operate? J. Trauma Acute Care Surg. 2010, 68, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, G.D.; Kepler, C.K.; Kurd, M.F.; Paul, J.T.; Rubenstein, R.N.; Harrop, J.S.; Brodke, D.S.; Chapman, J.R.; Vaccaro, A.R. A systematic review of the treatment of geriatric type II odontoid fractures. Neurosurgery 2015, 77 (Suppl. S1), S6–S14. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Kepler, C.K.; Kopjar, B.; Chapman, J.; Shaffrey, C.; Arnold, P.; Gokaslan, Z.; Brodke, D.; France, J.; Dekutoski, M. Functional and quality-of-life outcomes in geriatric patients with type-II dens fracture. JBJS 2013, 95, 729–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, H.E.; Kerr, S.M.; Fehlings, M.G.; Chapman, J.; Maltenfort, M.; Zavlasky, J.; Harris, E.; Albert, T.J.; Harrop, J.; Hilibrand, A.S. Trends in epidemiology and management of type II odontoid fractures: 20-year experience at a model system spine injury tertiary referral center. Clin. Spine Surg. 2010, 23, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, M.; Kono, M.; Nishiguchi, K.; Kakimaru, H.; Uchio, Y. Mortality in patients with hip fracture aged over 90 years: A report from a progressively aging island. Arch. Gerontol. Geriatr. 2012, 54, e113–e117. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age ≥ 90 years | Congenital instability |
| Acute unstable type II odontoid fracture | Rheumatoid arthritis |
| Traumatic etiology | Instability caused by tumor |
| - | Spinal infection |
| - | Previous cervical surgery |
| Patient Number | SEX M = Male F = Female | Age (Years) | BMI ** (kg/m2) | ASA | AACCI *** |
|---|---|---|---|---|---|
| 1 | M | 91 | 22 | 3 | 8 |
| 2 | F | 90 | 19 | 3 | 8 |
| 3 | F | 96 | 22.6 | 3 | 6 |
| 4 | F | 95 | 24.1 | 3 | 7 |
| 5 | F | 92 | 26 | 3 | 10 |
| 6 | F | 90 | 23.7 | 2 | 7 |
| 7 | F | 91 | 19 | 3 | 7 |
| 8 | M | 91 | 27.3 | 3 | 16 |
| 9 | F | 90 | 18.4 | 3 | 6 |
| 10 | F | 90 | 22.1 | 3 | 16 |
| 11 | F | 91 | 26.3 | 3 | 9 |
| 12 | F | 90 | 24.2 | 2 | 6 |
| 13 | F | 94 | 26.9 | 3 | 10 |
| 14 | F | 90 | 19.1 | 2 | 6 |
| 15 | F | 90 | 26 | 3 | 6 |
| Mean (SD *) | 91.4 (1.9) | 23.1(3.0) | 2.9 (0.3) | 9.1 (3.4) |
| Comorbidity | Frequency (%) |
|---|---|
| Heart failure | 6 (40%) |
| Diabetes mellitus | 4 (27%) |
| Peripheral vascular disease | 4 (27%) |
| Myocardial infarction | 3 (20%) |
| Severe renal disease | 3 (20%) |
| Tumor | 2 (13%) |
| Cerebrovascular disease | 2 (13%) |
| Chronic obstructive pulmonary disease | 1 (7%) |
| Major Complications | Frequency (%) | n = 1 (7%) |
|---|---|---|
| Pneumonic Sepsis | 1 (7%) | |
| Minor complications | Frequency (%) | n = 4 (27%) |
| Urinary tract infection | 2 (13%) | |
| Delirium | 1 (7%) | |
| Epistaxis | 1 (7%) |
| Group A: Patients ≥ 90 (n = 15) | Group B: Patients 65–89 (n = 72) | Significance (p ≤ 0.05) | |
|---|---|---|---|
| ASA * (1–4); Mean (SD) | 2.9 (±0.3) | 2.9 (±0.6) | NS |
| Postoperative ICU ** Stay (SD ***) | 3.8 (±6.6) | 1.9 (±2.1) | NS |
| 90-Day-Mortality (%) | 0 (0%) | 2 (2.8%) | NS |
| Postoperative neurological deficit (%) | 1 (6.7%) | 2 (2.7%) | NS |
| Minor complications | 4 (27%) | 5 (6.9%) | NS |
| Major complications | 1 (7%) | 9 (12.5%) | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issa, M.; Kiening, K.L.; Unterberg, A.W.; Scherer, M.; Younsi, A.; Fedorko, S.; Oskouian, R.J.; Chapman, J.R.; Ishak, B. Morbidity and Mortality in Patients over 90 Years of Age Following Posterior Stabilization for Acute Traumatic Odontoid Type II Fractures: A Retrospective Study with a Mean Follow-Up of Three Years. J. Clin. Med. 2021, 10, 3780. https://doi.org/10.3390/jcm10173780
Issa M, Kiening KL, Unterberg AW, Scherer M, Younsi A, Fedorko S, Oskouian RJ, Chapman JR, Ishak B. Morbidity and Mortality in Patients over 90 Years of Age Following Posterior Stabilization for Acute Traumatic Odontoid Type II Fractures: A Retrospective Study with a Mean Follow-Up of Three Years. Journal of Clinical Medicine. 2021; 10(17):3780. https://doi.org/10.3390/jcm10173780
Chicago/Turabian StyleIssa, Mohammed, Karl L. Kiening, Andreas W. Unterberg, Moritz Scherer, Alexander Younsi, Stepan Fedorko, Rod J. Oskouian, Jens R. Chapman, and Basem Ishak. 2021. "Morbidity and Mortality in Patients over 90 Years of Age Following Posterior Stabilization for Acute Traumatic Odontoid Type II Fractures: A Retrospective Study with a Mean Follow-Up of Three Years" Journal of Clinical Medicine 10, no. 17: 3780. https://doi.org/10.3390/jcm10173780