Article Text

Abstract
Purpose To determine if lumbar synovial cyst rupture in symptomatic patients results in improved clinical outcome when using direct tandem and/or coaxial percutaneous CT guided techniques.
Materials and methods 20 patients with unilateral lower extremity radiculopathy and/or low back pain underwent CT guided percutaneous treatment for their symptomatic lumbar synovial cysts. Cysts were identified with the use of a low osmolar non-ionic contrast agent via facet joint injection or through direct injection. Cyst rupture, using a direct tandem and/or coaxial technique, was attempted in all patients using an 18 gauge guide needle and a 22 gauge insert needle. Following attempted cyst aspiration, cyst rupture was performed using 1–3 mL of a mixture of methylprednisolone (2 mL, 80 mg) and bupivacaine (3 mL, 0.5%). All patients were followed-up in clinic for a minimum of 6 months after their procedures and up to a maximum of 24 months.
Results 11 patients were male and nine were female, with an average age of 65.6 years. 17 patients presented with severe unilateral lower extremity radiculopathy and three patients were experiencing low back pain. One of the patients had two synovial cysts, and therefore a total of 21 lumbar synovial cysts were treated in this group of patients. Direct cyst puncture was achieved using a tandem technique in nine patients, a coaxial interlaminar approach in seven patients, a coaxial transforaminal approach in two patients, and a coaxial trans-facet approach in three patients. Cyst rupture was documented in all cases, as evidenced by CT confirmation of cyst decompression and contrast agent extravasation into the epidural space. The mean surveillance period in these patients was 18 months. Six patients experienced their usual radicular pain within 2 months of their treatment. Four of these patients were re-treated for recurrent smaller cysts. These patients have not had a recurrence at 24 months of follow up. Two of these six patients elected to undergo open surgical decompression without symptomatic improvement. No treatment related complications were observed in this group of patients.
Conclusions Direct tandem and/or coaxial percutaneous CT guided techniques for rupture and treatment of symptomatic lumbar synovial cysts reduces recurrence rates and therefore helps avoid more invasive open surgical procedures in this group of patients.
- Spine
- Lumbosacral
- Intervention
Statistics from Altmetric.com
Introduction
Lumbar synovial cysts most often occur as a result of degenerative changes of the facet joint.1 ,2 With degenerative disruption of the facet joint, synovial fluid may build up within the joint. Small amounts of the fluid then escape from the joint capsule but remain within the synovium, creating a sac-like protrusion called a synovial cyst. Lumbar synovial cysts are usually found posterior and lateral to the dural sac where, depending on the exact location, they contribute to central spinal canal, lateral recess, or exit foramen stenosis. This leads to symptoms of lower back pain, radiculopathy, and neurogenic claudication.2 In descending order of frequency, lumbar synovial cysts are typically found at the L4–L5, L5–S1, L3–L4, and L2–L3 levels.
Lumbar synovial cysts are best diagnosed with MRI of the lumbar spine. They are located in close proximity to the facet joint, often anterior, but rarely posterior. Because of the proximity to the nerve roots, it is the anterior cysts that present with back pain and/or radicular symptoms, depending on the size and location of the cyst. Most cysts range in size from 3 mm to 12 mm in diameter. The cysts can project into the neural foramen and impinge upon the exiting nerve root, or they can project into the posterior and lateral aspect of the dural sac, resulting in variable spinal canal stenosis. Treatment options for symptomatic lumbar synovial cysts range from conservative to invasive measures.3 ,4 Conservative treatment, which is reserved for patients without neurological deficits, includes non-steroidal anti-inflammatory medications, physical therapy, and oral and/or epidural steroid medication. More aggressive surgical management is a treatment option for patients with neurological deficits, which includes laminectomy with or without fusion. Another treatment option is percutaneous image guided therapy, which includes aspiration, steroid injection, and rupture of the cyst. These percutaneous methods attempt to indirectly access the synovial cyst via the facet joint. Cysts that do not communicate with the joint cannot be successfully aspirated or ruptured with this technique. The recurrence rate for those cysts that do communicate and are initially ruptured or aspirated with this technique is high, and many of these patients subsequently require an open surgical decompression with or without spinal stabilization.
The goal of this study was to demonstrate and examine the efficacy of two advanced methods of CT guided percutaneous lumbar synovial cyst treatment, the tandem and coaxial methods, both of which directly access the lumbar synovial cyst. In the tandem technique, the first needle is used to opacify the cyst via facet injection and a second insert needle is advanced through an interlaminar epidural trajectory in an attempt to directly rupture the cyst. Coaxial methods use a guide needle for the initial percutaneous access and to guide a coaxially placed insert needle either to the posterior aspect of the neural foramen (transforaminal approach) or to the inferior aspect facet joint in an attempt to directly opacify and then rupture the cyst.
Methods and materials
Twenty patients underwent CT guided percutaneous treatment for their symptomatic lumbar synovial cysts over an 11 year period. All patients presented with unilateral lower extremity radiculopathy with or without lower back pain. These patients did not respond to conservative management and elected to undergo attempted percutaneous management of their symptomatic lumbar synovial cysts.
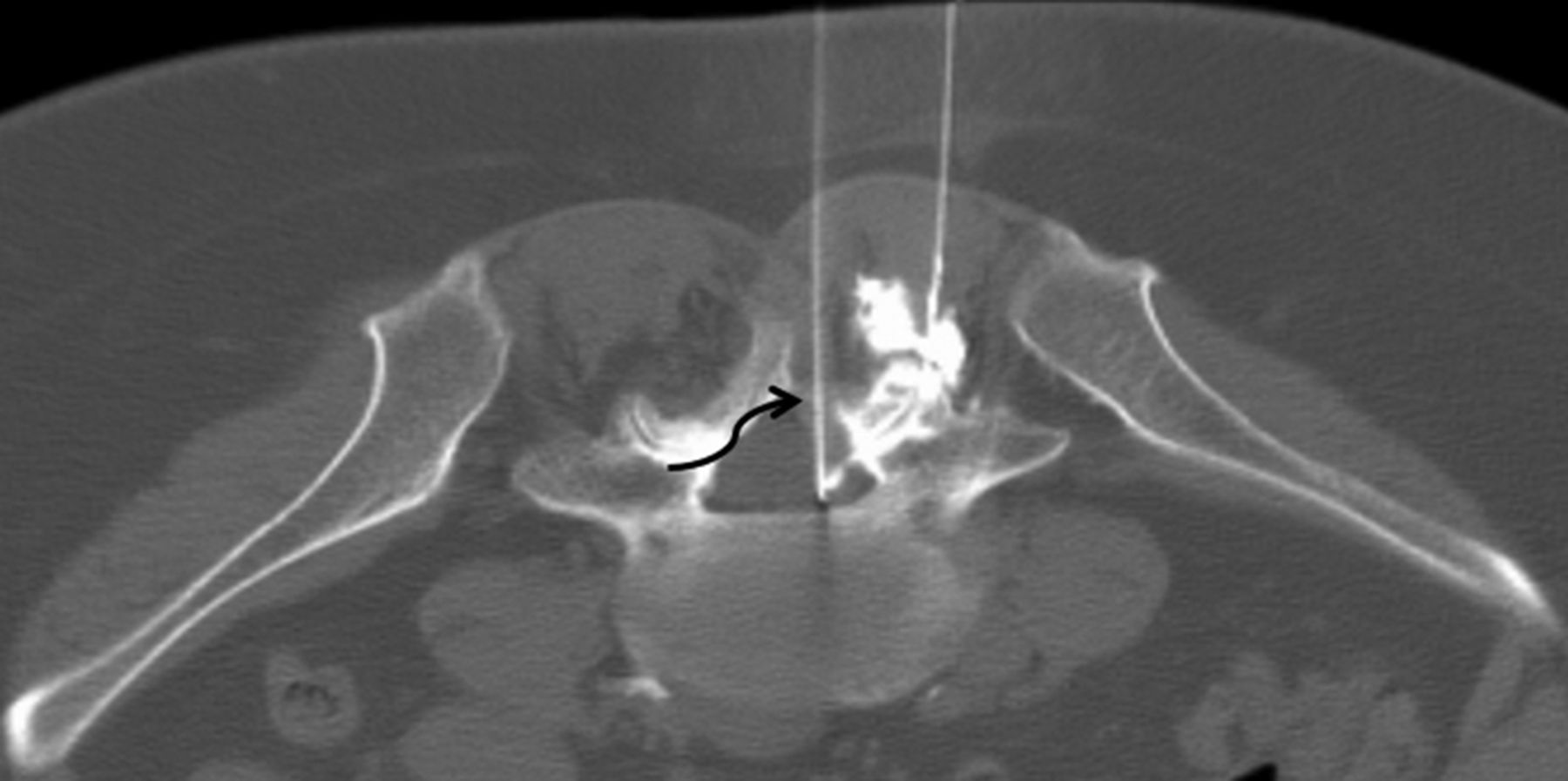
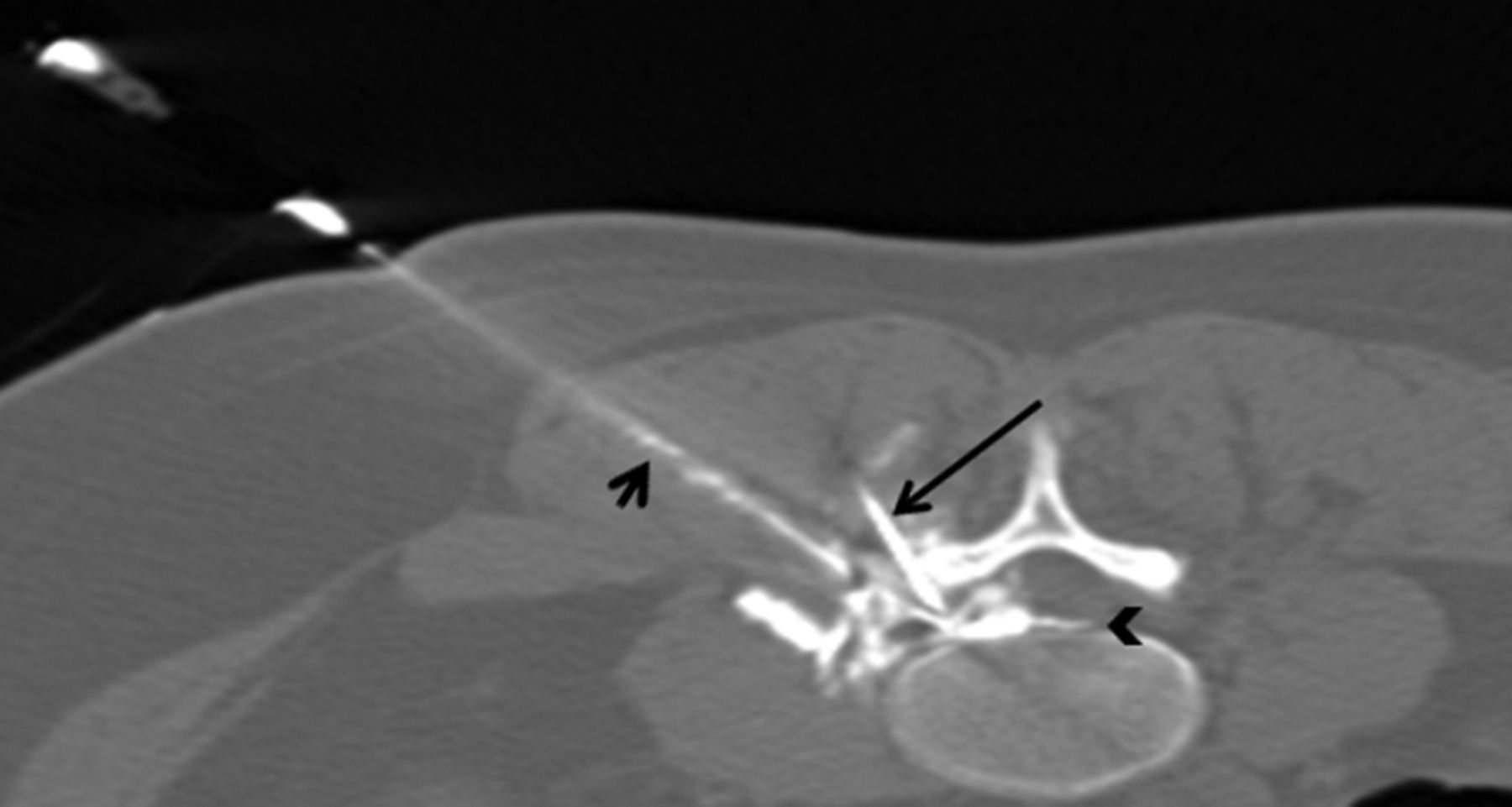
All procedures were performed under a strict aseptic technique using intravenous anesthesia and analgesia as well as CT fluoroscopic guidance. Lumbar synovial cyst rupture, using a direct tandem and/or coaxial technique, was attempted in all patients using an 18 gauge guide needle and a 22 gauge insert needle. A facet arthrogram was attempted using a low osmolar non-ionic contrast agent (Omnipaque 180; GE Healthcare) in all patients. In those instances where the facet arthrogram demonstrated the presence of a communicating cyst, an attempt was made to rupture the cyst by injecting the facet joint under pressure. In those patients in whom cyst rupture was not possible with this ‘traditional’ percutaneous technique, a tandem technique was utilized. The tandem approach consisted of simultaneous cyst opacification via arthrography with one needle and cyst puncture, attempted aspiration, and rupture with a second needle (18 and/or 22 gauge) (figure 1). Isolated non-communicating cysts were accessed via an interlaminar or transforaminal approach using a coaxial technique with an 18 gauge spinal (guide) needle and a 22 gauge (insert) Chiba needle (figure 2). For those cysts that could not be accessed via an interlaminar or transforaminal approach, a coaxial approach through the inferior aspect of the facet joint was used (figure 3).
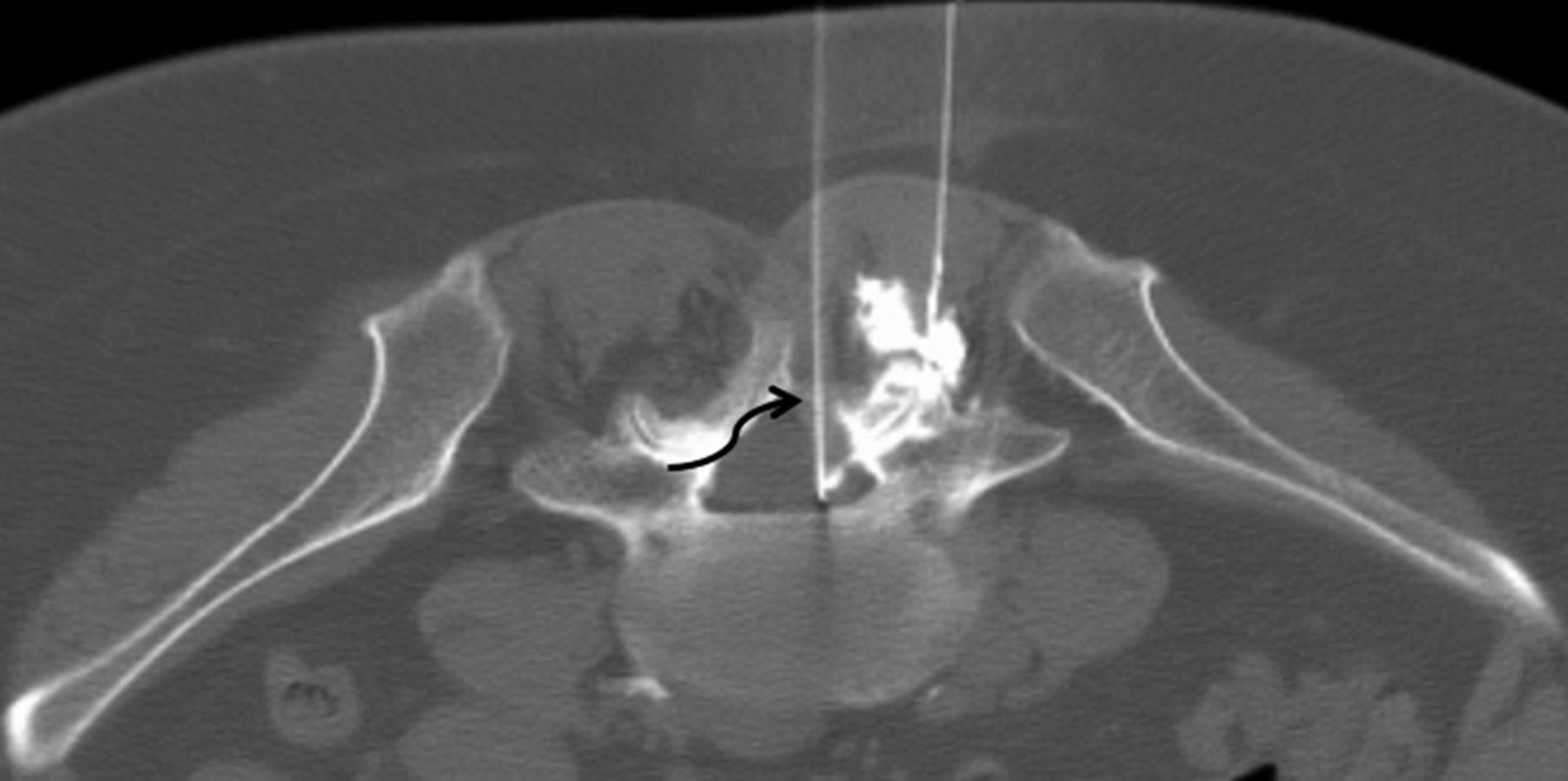
A septuagenarian with low back pain and right lower extremity radiculopathy. Right L4–5 facet arthrogram performed with CT fluoroscopic guidance and a 22 gauge spinal needle shows a 3 mm synovial cyst that encroaches upon the right L5 nerve root. The cyst could not be ruptured by facet injection and contrast extravasated posterior to the facet joint. Using a tandem interlaminar approach with a 22 gauge spinal needle, the synovial cyst was simultaneously opacified by facet injection and ruptured with the interlaminar spinal needle (curved arrow). The patient's symptoms immediately resolved with no recurrence at the 2 year follow-up.

A sexagenarian with recurrent right lower extremity radiculopathy; the patient had been treated with a transforaminal approach 3 months earlier for a right L4–5 synovial cyst that was located in the right L4–5 neural foramen. (A) T2 weighted axial MRI shows a recurrent L4–5 level 5 mm synovial cyst (arrow). The facet joint could not be accessed due to severe arthropathy. (B) The cyst was ruptured by injecting through the insert needle (large arrow); a small amount of epidural contrast agent confirms rupture of the cyst (small arrow). The patient's symptoms resolved, and the patient remained symptom free at the 2 year follow-up.

{kind=link}
{kind=link}
{kind=link}
A pentagenarian with left lower extremity radiculopathy. Facet arthrogram showed a 10 mm synovial cyst which could not be ruptured through facet joint injection. The cyst could not be safely accessed with a coaxial (small arrow) transforaminal approach. An 18 gauge spinal needle was exchanged over a 20 gauge spinal needle (not shown) and advanced into the inferior aspect of the facet joint (large arrow) with subsequent decompression and rupture of the cyst (arrowhead). This patient remained asymptomatic at the 6 month follow-up.
Additional intravenous analgesics were administered just prior to attempted cyst rupture in order to facilitate patient comfort and cooperation during the procedure. Following attempted cyst aspiration, cyst rupture was performed using 1–3 mL of a mixture of methylprednisolone (2 mL, 80 mg) and bupivacaine (3 mL, 0.5%). All patients have been or were followed-up in clinic at 3 weeks, 3 months, 12 months, and 24 months after their procedure or when they presented with possible recurrent symptoms. Institutional review board approval was obtained for this study.
Results
Eleven patients were male and nine were female, with an average age of 65.6 years. Seventeen patients presented with severe (9–10/10) unilateral lower extremity radiculopathy, two patients presented with severe 10/10 low back pain, and one patient presented with both 9/10 low back pain with radiculopathy. When radiculopathy was present, the symptomatic side correlated with the side of the synovial cyst. Eleven cysts were located at L4–5, five cysts were found at L3–4, four cysts were identified at L3–4, and one cyst was located at L2–3. The average cyst size, using the maximum cyst diameter, was 7.3 mm (range 3–14 mm).
Twelve cysts did communicate with the adjacent facet joint whereas nine did not. Nine cysts were treated with a tandem needle technique. A coaxial technique was used to treat the other 14 cysts, seven with an interlaminar approach, two with a transforaminal approach, and three with a trans-facet approach. Cyst aspiration was successfully performed in seven of the 21 cysts, yielding straw colored viscous fluid. Cyst rupture was documented in all cases by the eradication of the cyst, as seen with post-procedure imaging and the presence of small amounts of contrast agent within the epidural space.
The mean surveillance period in these patients was 18 months (range 4–24 months). Four patients were re-treated for recurrent, though smaller, cysts, which occurred within 2 months of the initial treatment. These patients have not had a recurrence at a minimum of 15 months of follow-up. Two patients with a cyst recurrence elected to undergo open surgery at 5 months after their initial percutaneous treatment. One of these patients had axial low back pain with L3–4 spinal canal stenosis due to a 12 mm cyst and the other had right lower extremity radiculopathy due to an L3–4, 7 mm synovial cyst. Neither of these two patients showed significant symptomatic improvement and have required chronic pain management. To date, none of the remaining patients (18) have had a recurrence. No treatment related complications were observed in this group of 20 patients.
Discussion
Lumbar synovial cysts are cystic lesions that arise from the synovium of degenerated facet joints. Some of these cysts do not necessarily demonstrate communication with the adjacent facet joint and are sometimes referred to as ganglion cysts. These latter cysts are not lined by synovial cells.1 The term juxta-articular cyst has also been used interchangeably with lumbar synovial cyst. Lumbar synovial cysts are most commonly encountered within the lumbar spine, most frequently at the L4–5 level, but also at other lumbar levels. They occur more frequently in adult women than in adult men. Their incidence is approximately 0.6%.2 When these cysts are in contact with the spinal canal or exit foramen, and when they reach sufficient size, they may become symptomatic, resulting in axial low back pain with or without a radicular component, depending on their location. The radicular pain often corresponds to the compressed nerve root that is seen on the patient's imaging examination.
Because these lesions can cause significant symptoms, they are often identified on MRI studies near the time of the patient's clinical presentation. The cyst is usually associated with a facet joint that demonstrates advanced facet arthropathy. Synovial cysts are round well circumscribed masses that are hypo- to iso-intense on T1 weighted MRI and hyperintense on T2 weighted sequences. In some cases it might be possible to demonstrate signal intensity continuity between the cyst and the adjacent facet joint. This is not common, however, and the definitive way to establish a communication between the cyst and the facet joint is by performing an arthrogram, either via fluoroscopic or CT guidance. The presence of cyst–facet joint communication is important because it is the only way that a cyst can potentially be aspirated or ruptured when using a facet joint injection technique that indirectly accesses the cyst. The cyst wall is moderately thick and shows variable enhancement following intravenous contrast administration. Chronic cysts may contain calcification within their walls, a finding which is better visualized on CT.1 As the cyst expands in size it will impinge on the adjacent neural elements. This results in either focal axial low back pain and/or radiculopathy.
Symptomatic lumbar synovial cysts can be managed with a few different treatment options. An initial attempt at a conservative management is usually initiated by the treating clinician. This often consists of a combination of bed rest, oral analgesics, non-steroidal anti-inflammatory agents, and/or a short course of steroid therapy. Temporary relief, at best, is achieved with conservative management. Surgery is another possible treatment option for symptomatic lumbar synovial cysts. The surgical option is believed to be curative, especially when the offending cyst is resected. The extent of the surgery is variable and may include laminectomy, facetectomy, or possible posterior spinal fusion with bone graft or instrumentation.2 ,3 These open surgical procedures are not without risks. The risks of open lumbar spine surgery include bleeding, infection, dural tear, and CSF leak. More long term complications include spinal de-stabilization in patients who have not been fused, as well as the possible creation of new pain generators within the treated lumbar spine. Some patients may not be good surgical candidates due to their medical comorbidities. The efficacy of surgery for effectively treating symptomatic lumbar synovial cysts and eradicating pain is not 100%. In the largest surgical series that addressed the issue of surgical efficacy, 90% pain relief was observed.4
Fluoroscopy guided percutaneous facet joint injection was developed as a treatment option that is more invasive than conservative management but less aggressive than open surgery. The objective of this procedure is to access the affected facet joint space using a percutaneously placed spinal needle that is advanced under fluoroscopic guidance. In those cases where it is possible to access the facet joint and where the joint communicates with the cyst, it is usually possible to opacify the joint space and the cyst with a radiopaque contrast agent. Attempts can then be made to aspirate the cyst contents by aspirating the joint as well as rupturing the cyst by pressurizing the joint with an injection of contrast, liquid steroid agent, and/or anesthetic agent. The injection is considered to be successful if the cyst is ruptured, as evidenced by disappearance of the cyst and/or the epidural spread of the previously contained contrast agent. Successful cyst rupture is almost always associated with marked improvement in the patients’ clinical symptoms.1 This technique, with minor variations, has been used for the past several decades as the secondline therapy for symptomatic synovial cysts prior to considering surgical interventions.
A review of the literature for percutaneous fluoroscopy guided trans-facet therapy shows moderate to favorable benefits with this treatment. Many of the initial studies consist of small patient series with limited clinical follow-up and short follow-up periods. One study of 12 patients that included imaging follow-up noted that symptomatic relief, seen in 75% of patients, correlated well with either complete or partial reduction of cyst volume, which was also seen in 75% of patients.1 In another series of 32 patients, pain relief was achieved in 72% of patients.5 The cyst recurrence rate in this group of patients was 37.5% (12 patients), with five of these patients undergoing a repeat successful cyst rupture and six of these patients ultimately requiring surgical resection of the cyst. Patients who had a repeat attempt at cyst rupture had a 50% chance of a therapeutic benefit.5 By far the largest study to investigate this treatment option included 101 patients.4 In this study, the authors found that the average duration of pain relief following facet injection was 8.4 months. The treatment benefit was attributed to both mechanical decompression of the cyst and to the anti-inflammatory effect of the epidural steroid extravasation. They also noted that 50% of these patients eventually required an open surgical procedure and that there was no statistically significant difference between patients who received injections only versus patients who underwent surgery with respect to pain scores or Oswestry Disability Index scores.4 The clinical follow-up in this retrospective series was somewhat limited as there was only a 79% response rate. Additionally, the post-procedure evaluation in this study consisted only of a telephone interview, with no direct clinical evaluation of the patients.
The percutaneous image guided trans-facet joint, or indirect cyst rupture technique, has inherent limitations. First, the operator must be able to access the joint space which is not always possible in the setting of severe facet arthrosis. In those cases where it is possible to perform an arthrogram, the joint space may not communicate with the cyst. Thus facet joint access and lack of cyst communication are two potential barriers to this treatment option. In some cases, when it is possible to access the joint and opacify the cyst, it may not be possible to rupture the cyst. This is not an infrequent occurrence and has been noted in prior large studies, with the incidence of fluoroscopy confirmed ‘successful’ cyst rupture ranging from 75% to 81%.1 ,4 There are two major reasons for not achieving cyst rupture: (1) it may not be feasible to adequately pressurize the joint as the contrast agent leaks around the needle entry site and (2) the cyst wall may be thick or calcified and resistant to the pressurization maneuver.
Given the challenges associated with percutaneous image guided trans-facet therapy, we sought to develop alternative and more direct treatment strategies for symptomatic lumbar synovial cysts. The advent of CT fluoroscopy enabled us to consider different access routes and approaches for symptomatic lumbar synovial cysts, regardless of whether or not they communicate with the facet joint. Cross sectional imaging improves the visualization of all key structures and facilitates cyst identification as well as the effects of intervention. Needle guidance, with co-axial techniques, is also improved with CT fluoroscopy. This enables a percutaneous image guided technique with a somewhat more direct approach to accessing and rupturing the cyst. In our series, different approaches, interlaminar, trans-facet, or transforaminal, were used to access each cyst. The location of the cyst and its relation to the dural sac and exiting nerve root were primary determinants in establishing the safest needle trajectories. Cysts that are within the spinal canal might be accessed via the dorsolateral epidural space through an interlaminar approach. Cysts that are located within the neural foramen may require a coaxial technique either with a transforaminal or inferior facet joint approach. With these approaches and with direct visualization with CT, cyst rupture is now more readily achievable than with the previous techniques and technology. The traditional percutaneous image guided facet injection technique did not and would not be effective in those nine facet injections in our series in which the cyst did not communicate with the facet joint. This may account for the variable success rate with indirect cyst rupture via facet injection that has been previously reported in the literature.2 In our study, cyst rupture was objectively demonstrated with CT confirmation in each case. This was associated with at least temporary symptomatic improvement in all patients. In the six patients with cyst recurrence, symptoms developed within 6 months of the initial percutaneous treatment. Cyst communication with the facet joint was observed in four of these six patients with cyst recurrence. No other specific trends in this small group of six patients with respect to cyst size, morphology, or location were identified. The percutaneous procedure was repeated in four of these patients with a successful outcome in terms of cyst rupture and durable symptom relief. Two of the six patients underwent open surgical treatments, including cyst resection and laminectomy in both patients, and posterior fusion in one of the two patients. Despite adequate decompression, their symptoms have persisted. Certainly, while open surgery has been shown to have a high success rate in the treatment of symptomatic lumbar synovial cysts, a systematic review of the literature shows that the overall success rate, in terms of symptomatic relief, is approximately 92%.6 With respect to lumbar synovial cyst eradication or recurrence, decompression surgery alone is associated with a cyst recurrence rate of 1.8%. The lumbar synovial cyst recurrence rate of 0% is seen only after open surgical decompression and lumbar fusion, a more extensive surgical procedure. The latter surgical approach may benefit those patients with lumbar synovial cysts and associated spondylolisthesis.2 ,7 As with any other surgical procedure, complications may and do occur, and include CSF leak, postoperative instability, infection, and bleeding. In a large series of 194 patients that were treated with lumbar spine surgery, the observed complication rate was 6%.3 Thus the management of symptomatic lumbar synovial cysts is challenging, regardless of the treatment option.
Our favorable experience (an overall success rate (90%) that was higher compared with studies that have used the facet injection techniques) with these additional percutaneous techniques and with CT fluoroscopy suggests that these techniques and tools may be of benefit in the treatment of symptomatic synovial cysts. With CT, the immediate demonstration of cyst location and communication or non-communication with the facet joint facilitates the subsequent treatment decisions with respect to procedure and approach. Those cysts that do not communicate or do not rupture with the traditional ‘pressurization’ technique may indeed require a tandem or coaxial approach. Recurrent cysts that have been previously treated with the traditional indirect facet joint injection technique might also be considered for a possible tandem or coaxial approach.
The necessity for clinical follow-up of these patients is reinforced by the potential for cyst and symptom recurrence, particularly during the first year after percutaneous treatment. Our 2 year duration for following up these patients is consistent with the observation periods that have been described in the literature for this specific condition.2 With this follow-up time frame we were able to show a much longer duration of treatment benefit for the direct percutaneous tandem or coaxial techniques compared with the indirect, or facet, injection technique. Overall, 18 out of the 20 patients in our case series (90%) have remained symptom free over the study interval. Moreover, the requirement for subsequent open surgical intervention in this case series (two out of 20 patients) was much less than the 54% rate that has been previously reported with the fluoroscopy guided percutaneous facet injection technique.4
Our study limitations include a relatively small sample size at a single institution, performed by one operator. This is a case series and patients were not randomized into facet only injections versus direct cyst injection techniques. These percutaneous tandem and coaxial procedures do require an element of operator experience and comfort level with spine injection techniques. The potential risks of these procedures include dural puncture, subarachnoid space injection, and vascular or neural injury. The key with respect to procedure safety, however, is to always identify the cyst prior to attempting direct rupture. Nevertheless, the favorable results that have been observed in our series, combined with the increased durability of the treatment effect, suggest that a direct approach may be considered in those patients who have not responded to other non-surgical therapies.
Footnotes
-
Contributors AOO made a substantial contribution to the study concept, developed the techniques and performed the procedures, performed patient follow-up examinations, re-wrote and edited the main manuscript, and selected the final figure parts. LT did the institutional review board submission, wrote the preliminary manuscript, was responsible for patient database creation and management, and performed the initial analysis of the data.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review board of Winthrop-University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.