
Abstract
Introduction and hypothesis
Androgen insensitivity syndrome (AIS) constitutes a natural model to study effects of androgens and estrogens on growth and bone density. We evaluated height and bone density in patients with AIS with mutations in the androgen receptor (AR) gene.
Methods
A retrospective analysis was conducted of eight subjects with complete AIS (CAIS) and four with partial AIS (PAIS) submitted to gonadectomy followed by estrogen replacement, and three with PAIS who did not undergo gonadectomy. Standing height and bone mineral apparent density (BMAD) by DXA were measured and compared with male (z m) and female (z f) reference populations. The z-scores were compared with a value of zero using the one-sample t-test.
Results
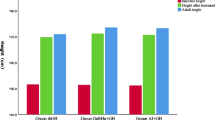
Final heights of patients with CAIS and PAIS were intermediate between those predicted for females and males. BMAD of the lumbar spine in CAIS and PAIS after gonadectomy and estrogen replacement (z f = − 1.56 ± 1.04, P = 0.006, and z m = − 0.75 ± 0.89, P = 0.04) indicated vertebral bone deficit, whereas BMAD at the femoral neck was normal. No patient reported fractures.
Conclusion
Subjects with AIS had mean final height intermediate between mean normal male and female, and decreased bone mineral density in the lumbar spine. These data suggest an important role for androgens in normal male growth and bone density not replaced by estrogens.
Similar content being viewed by others


References
Quigley CA, De Bellis A, Marschke KB et al (1995) Androgen receptor defects: historical, clinical, and molecular perspectives. Endocr Rev 16:271–321
Boehmer AL, Brinkmann O, Bruggenwirth H et al (2001) Genotype versus phenotype in families with androgen insensitivity syndrome. J Clin Endocrinol Metab 86:4151–4160
Melo KF, Mendonca BB, Billerbeck AE et al (2003) Clinical, hormonal, behavioral, and genetic characteristics of androgen insensitivity syndrome in a Brazilian cohort: five novel mutations in the androgen receptor gene. J Clin Endocrinol Metab 88:3241–3250
Vanderschueren D, Vandenput L, Boonen S et al (2004) Androgens and bone. Endocr Rev 25:389–425
Griffin J, Wilson JD (1989) The androgen resistance syndromes: 5a-reductase deficiency, testicular feminization, and related disorders. In: Scriver CR, Beaudet AL, Sly WS et al (eds) (1989) The metabolic basis of inherited disease. McGraw-Hill, New York, pp 1919–1944
MacDonald PC, Madden JD, Brenner PF et al (1979) Origin of estrogen in normal men and in women with testicular feminization. J Clin Endocrinol Metab 49:905–916
Zachmann M, Prader A, Sobel EH et al (1986) Pubertal growth in patients with androgen insensitivity: indirect evidence for the importance of estrogens in pubertal growth of girls. J Pediatr 108:694–697
Frank GR (2003) Role of estrogen and androgen in pubertal skeletal physiology. Med Pediatr Oncol 41:217–221
Grumbach MM (2000) Estrogen, bone, growth and sex: a sea change in conventional wisdom. J Pediatr Endocrinol Metab 13:1439–1455
Carrascosa A, Audi L, Ferrandez MA et al (1990) Biological effects of androgens and identification of specific dihydrotestosterone-binding sites in cultured human fetal epiphyseal chondrocytes. J Clin Endocrinol Metab 70:134–140
Abu EO, Horner A, Kusec V et al (1997) The localization of androgen receptors in human bone. J Clin Endocrinol Metab 82:3493–3497
Ben-Hur H, Thole HH, Mashiah A et al (1997) Estrogen, progesterone and testosterone receptors in human fetal cartilaginous tissue: immunohistochemical studies. Calcif Tissue Int 60:520–526
Noble B, Routledge J, Stevens H et al (1999) Androgen receptors in bone-forming tissue. Horm Res 51:31–36
van der Eerden BC, van Til NP, Brinkmann AO et al (2002) Gender differences in expression of androgen receptor in tibial growth plate and metaphyseal bone of the rat. Bone 30:891–896
Munoz-Torres M, Jodar E, Quesada M et al (1995) Bone mass in androgen-insensitivity syndrome: response to hormonal replacement therapy. Calcif Tissue Int 57:94–96
Bertelloni S, Baroncelli GI, Federico G et al (1998) Altered bone mineral density in patients with complete androgen insensitivity syndrome. Horm Res 50:309–314
Marcus R, Leary D, Schneider DL et al (2000) The contribution of testosterone to skeletal development and maintenance: lessons from the androgen insensitivity syndrome. J Clin Endocrinol Metab 85:1032–1037
Tanner JM, Whitehouse RH (1976) Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child 51:170–179
Katzman DK, Bachrach LK, Carter DR et al (1991) Clinical and anthropometric correlates of bone mineral acquisition in healthy adolescent girls. J Clin Endocrinol Metab 73:1332–1339
Bhudhikanok GS, Wang MC, Eckert K et al (1996) Differences in bone mineral in young Asian and Caucasian Americans may reflect differences in bone size. J Bone Miner Res 11:1545–1556
Bachrach LK, Hastie T, Wang MC et al (1999) Bone mineral acquisition in healthy Asian, Hispanic, black, and Caucasian youth: a longitudinal study. J Clin Endocrinol Metab 84:4702–4712
Carter DR, Bouxsein ML, Marcus R (1992) New approaches for interpreting projected bone densitometry data. J Bone Miner Res 7:137–145
Smith DW, Marokus R, Graham JM Jr (1985) Tentative evidence of Y-linked statural gene(s). Growth in the testicular feminization syndrome. Clin Pediatr (Phila) 24:189–192
Sobel V, Schwartz B, Zhu YS et al (2006) Bone mineral density in the complete androgen insensitivity and 5(-reductase-2 deficiency syndromes. J Clin Endocrinol Metab 91:3017–3023
Colvard DS, Eriksen EF, Keeting PE et al (1989) Identification of androgen receptors in normal human osteoblast-like cells. Proc Natl Acad Sci USA 86:854–857
Weinstein RS, Jilka RL, Parfitt AM et al (1997) The effects of androgen deficiency on murine bone remodeling and bone mineral density are mediated via cells of the osteoblastic lineage. Endocrinology 138:4013–4021
Kousteni S, Bellido T, Plotkin LI et al (2001) Nongenotropic, sex-nonspecific signaling through the estrogen or androgen receptors: dissociation from transcriptional activity. Cell 104:719–730
Francis RM (1999) The effects of testosterone on osteoporosis in men. Clin Endocrinol (Oxf) 50:411–414
Kiratli BJ, Srinivas S, Perkash I et al (2001) Progressive decrease in bone density over 10 years of androgen deprivation therapy in patients with prostate cancer. Urology 57:127–132
Frost HM (1987) The mechanostat: a proposed pathogenic mechanism of osteoporoses and the bone mass effects of mechanical and nonmechanical agents. Bone Miner 2:73–85
Rauch F, Bailey DA, Baxter-Jones A et al (2004) The ‘muscle-bone unit’ during the pubertal growth spurt. Bone 34:771–775
Saggese G, Baroncelli GI, Bertelloni S (2002) Puberty and bone development. Best Pract Res Clin Endocrinol Metab 16:53–64
Schiessl H, Frost HM, Jee WS (1998) Estrogen and bone-muscle strength and mass relationships. Bone 22:1–6
Frost HM, Schonau E (2000) The “muscle-bone unit” in children and adolescents: a 2000 overview. J Pediatr Endocrinol Metab 13:571–590
Schoenau E, Neu CM, Mokov E et al (2000) Influence of puberty on muscle area and cortical bone area of the forearm in boys and girls. J Clin Endocrinol Metab 85:1095–1098
Vered I, Kaiserman I, Sela BA et al (1997) Cross genotype sex hormone treatment in two cases of hypogonadal osteoporosis. J Clin Endocrinol Metab 82:576–578
Mizunuma H, Soda M, Okano H et al (1998) Changes in bone mineral density after orchidectomy and hormone replacement therapy in individuals with androgen insensitivity syndrome. Hum Reprod 13:2816–2818
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Danilovic, D.L.S., Correa, P.H.S., Costa, E.M.F. et al. Height and bone mineral density in androgen insensitivity syndrome with mutations in the androgen receptor gene. Osteoporos Int 18, 369–374 (2007). https://doi.org/10.1007/s00198-006-0243-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0243-6