


ABSTRACT
Background Traumatic rotatory subluxation of the atlantoaxial joint is a rare but potentially life-threatening injury in adults. While acute cases have been shown to be managed successfully with closed reduction, chronic injuries in skeletally mature patients have rarely been reported.
Methods We present management of a 64-year-old female who presents 2.5 years after a traumatic cervical injury with neck pain and torticollis. Imaging revealed rotatory subluxation of C1–C2 without cord impingement. A focused appraisal of the reported literature was also performed.
Results Successful reduction was achieved with halo cervical traction, followed by definitive treatment with atlantoaxial arthrodesis.
Conclusions Cases of fixed, chronic C1–C2 rotatory subluxation after traumatic etiology may be amenable to closed reduction with skeletal traction and fusion.
Level of Evidence 4.
Clinical Relevance Chronic, post-traumatic atlantoaxial rotatory subluxation in the adult population is extremely rare, without a well-described treatment algorithm. The purpose of this case report is to highlight the reduction and fixation of someone with this injury.
INTRODUCTION
The atlantoaxial joint and its concomitant ligaments provide significant rotational and biomechanical stability to the cervical spine.1 Isolated traumatic rotatory subluxation of the atlantoaxial joint without fracture is a rare injury,1–3 with no consensus for management in the adult population.4 Missed or neglected treatment of these injuries may lead to a chronic rotated neck posture (mimicking torticollis), pain, and potential for neurologic compromise.4–6 While acute traumatic atlantoaxial instability may be treated with closed management,1 delayed presentation can limit reducibility, maintenance of reduction, or both.7–11
Chronic atlantoaxial rotatory subluxation (AARS) has been reported in the pediatric population, with several authors recommending attempted treatment with external halo bracing if reducible.12,13 However, the etiology in children is most often secondary to infection rather than direct trauma. Due to the rarity of this traumatic event, subluxations can often be missed on standard radiographs in the acute setting.14 The associated spasm and contracture of the sternocleidomastoid that occurs with a late presentation4 may require open reduction and arthrodesis of the atlantoaxial joint.
To the authors' knowledge, delayed presentation (>2 years) of purely traumatic atlantoaxial subluxation in the skeletally mature individual has not been reported. The purpose of the present report was to present a rare case of chronic AARS after a trauma in an adult patient treated successfully with closed reduction and arthrodesis.
Case Report
An otherwise healthy 64-year-old female presented to the clinic after sustaining a ground level fall, hitting the right side of her neck on a lower cabinet 2.5 years before. She reported complaints of neck pain, difficulty with neck range of motion, along with an inability to comfortably face her head directly forward. The patient denied any numbness, weakness, or changes in balance and coordination. Over the course of 2 years, the patient attempted conservative treatment with physical therapy, acupuncture, muscle relaxants, and multiple Botox injections.
Physical Exam and Imaging
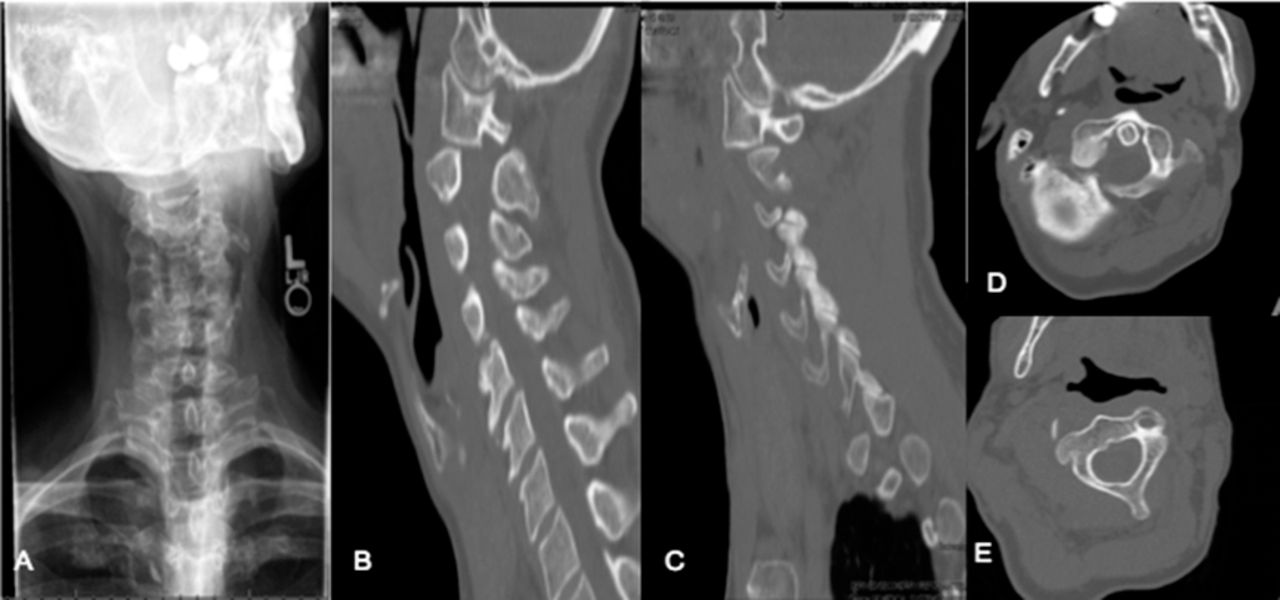
On physical exam, the patient was neurologically intact. The patient's head was fixed in a position rotated to the left, with limited ability to rotate (∼20%) to the right side. In addition, the patient was unable to fully flex or extend the neck. Standard cervical spine x-rays including flexion/extension radiographs were obtained, demonstrating no evidence of fracture or frank dislocation. Computed tomography (CT) obtained demonstrated rotary displacement of the atlas without anterior displacement (Fielding type 1, Figure 1) in relation to the odontoid. Magnetic resonance imaging was also performed with no evidence of cord compression.

(A) Demonstrates radiographic rotation of the head in the anterior-posterior view. Computed tomography scan showed (B) posterior and (C) anterior subluxation of the C1 lateral mass in relation to the C2 facet. Axial view demonstrated (D) the C1 arch rotated about odontoid, significantly subluxed compared to (E) the C2 vertebrae.
Treatment Management
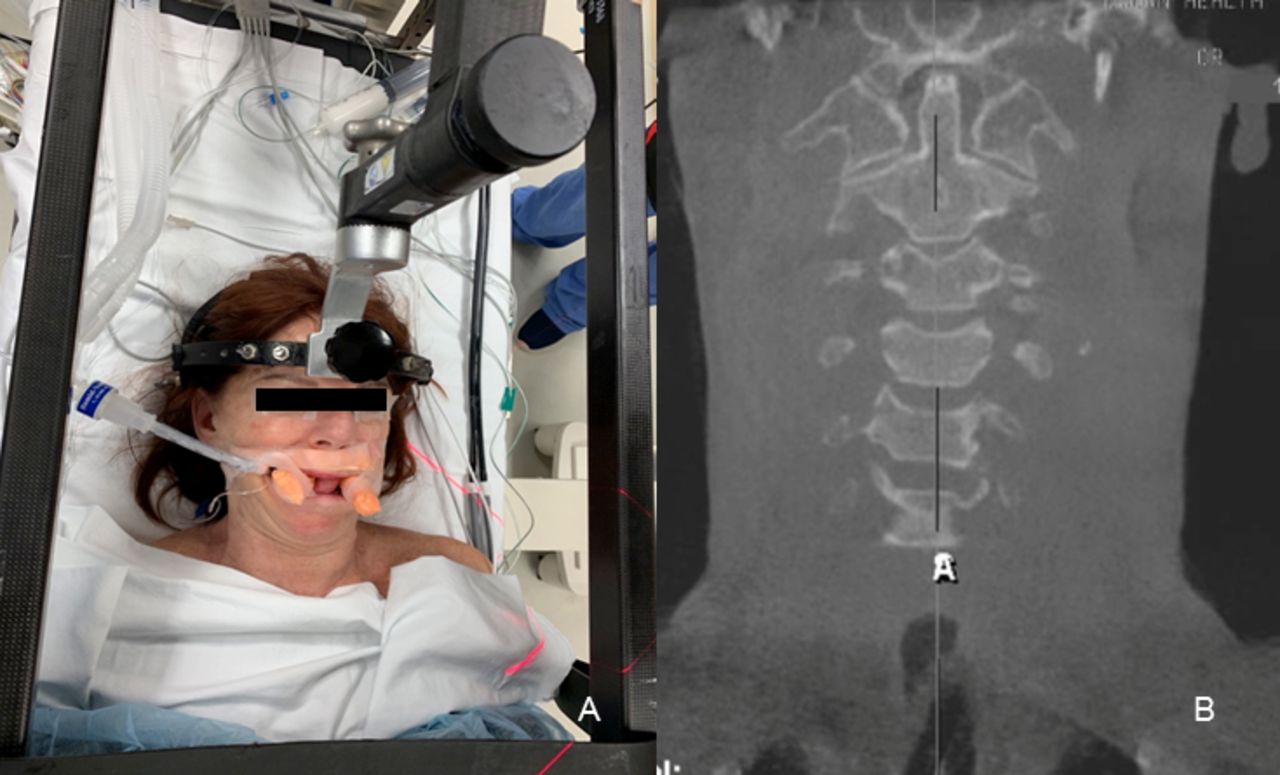
The decision was made to admit the patient to the hospital, with an initial attempt at closed reduction. A halo crown was secured, and 10 lb of in-line traction was initially placed (Figure 2A). Over the course of 24 hours, an additional 10 lb were added. Repeat radiographs after approximately 30 hours in traction demonstrated adequate reduction of the subluxation (Figure 2C). Given the chronicity of the injury, it was felt that the chance of recurrent subluxation would be high, so the patient was taken to the operating room for C1–C2 posterior spinal fusion. After a total of 48 hours of halo traction, the patient was brought to the operating room with the halo attached to a Mayfield head positioner on a rotating Jackson table. Intraoperative three-dimensional (3D) fluoroscopy was then used to confirm that reduction was still maintained before hardware placement (Figure 3). Using C1 lateral mass and C2 pedicle screws via the technique described by Harms et al,15 the atlantoaxial joint was fixed in anatomic alignment, with demineralized bone matrix putty used to augment the arthrodesis (Figure 4). The patient tolerated the procedure well without complication. She was discharged on postoperative day 2 in a hard collar with good maintenance of reduction.

(A) Closed reduction using in line halo traction was applied. (B) Pretraction open-mouth odontoid view demonstrated bilateral asymmetry of the C1–C2 facet joints. (C) Significantly improved reduction of the atlantoaxial subluxation was seen following in line traction.
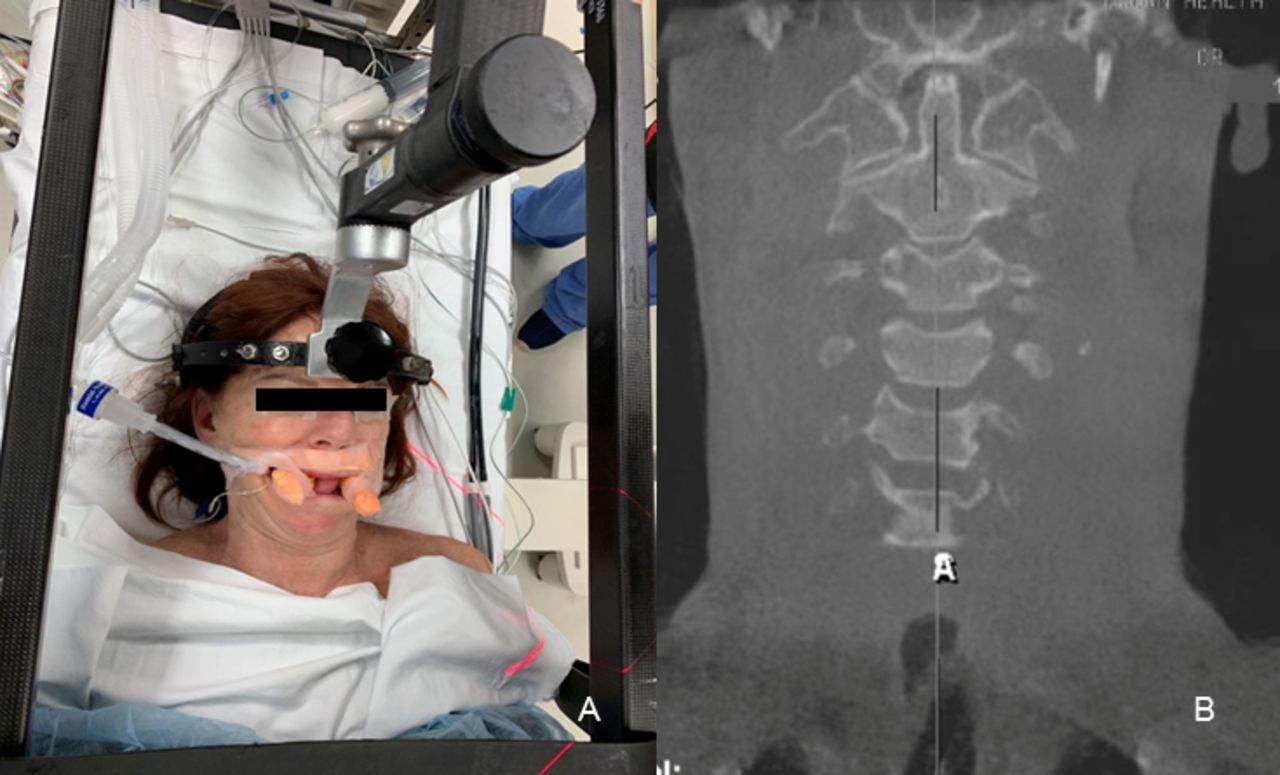
(A) Intraoperative positioning in Mayfield positioner with bilateral bite blocks to allow for open-mouth odontoid view during surgery. (B) A three-dimensional C-arm scan demonstrated maintained reduction before instrumentation.
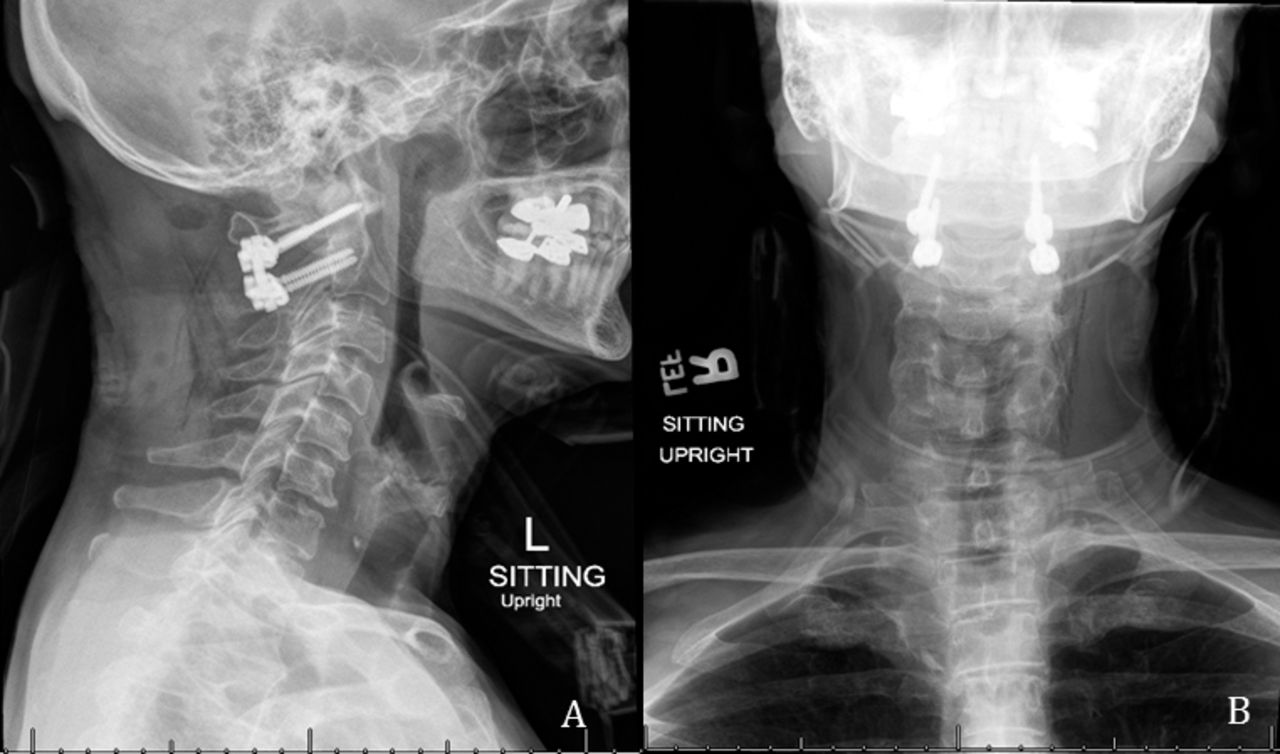
(A) Postoperative C1–C2 instrumented posterior spinal fusion with (B) correction of preoperative clinical torticollis seen on the anterior-posterior view.
DISCUSSION
Chronic subluxation of the atlantoaxial joint is a rare traumatic event in adults, with no current consensus for management. We present a case describing a patient who presented 2.5 years from injury with torticollis that was reducible using halo traction followed by posterior C1–C2 fusion.
The atlantoaxial joint is formed by 2 saddle-shaped, biconvex surfaces that contribute to roughly 50% of axial neck rotation.3,16 In addition, the transverse and alar ligaments are important static stabilizers, preventing anterior translation of C1 on the C2 vertebrae.1 Authors of previous cadaveric studies simulating rotatory subluxation or dislocation have suggested that facet joint disruption followed by the alar ligaments may be the mechanism by which these injuries occur.17,18 AARS without associated fracture is rare in adults, with most cases in the literature describing either unilateral or bilateral facet dislocation.19–21 The cause of this dislocation has been generally due to higher energy trauma, such as a fall from height, motor vehicle accidents, or sports-related injuries.17,22
Despite the rarity of this injury, the Fielding classification was developed to describe 4 types of rotatory instability.23 Type 1, as seen in this case, is rotatory subluxation without disruption of the atlantodens interval. With disruption of the transverse ligament, progressive changes in the atlantodens interval (type 2) can occur, with potential impingement on the spinal cord in types 3 or 4 after facet dislocation. While this classification helps with communication of the injury, it does not provide guidance for treatment or recurrence. Singh et al24 reported a case of a 25-year-old female with traumatic bilateral facet rotatory subluxation mimicking torticollis after a motor vehicle collision. Although initially missed on radiographs, the patient was treated acutely with a halo brace for 4 weeks, with resolution of symptoms and maintenance of reduction at 1 year.24 Venkatesan et al1 reported 2 similar cases of traumatic AARS in skeletally mature patients after motor vehicle accidents. Both patients underwent acute reduction with halo traction, followed by 8 weeks in a hard collar.1 The patients maintained anatomic reduction at over 2-year follow up, without requiring arthrodesis.1 While these reports showed success without surgical intervention in cases of acute AARS, treatment of chronic cases of subluxation in adults have not established.
Chronic AARS has previously been defined as subluxation of greater than 3 months.3,22 Ishii et al4 recently reported a case series of 12 consecutive pediatric patients with chronic atlantoaxial instability. The authors recommended a “remodeling therapy” involving initial closed reduction in the operating room followed by halo bracing for up to 3 months to allow for the C2 facet to remodel.4,25 Although only 3 patients in their cohort were secondary to trauma, no patient had recurrence of symptoms nor subluxation at a mean follow up of 42 months.4 The authors recommended fusion for patients that are either irreducible or have bony union between C1 and C2. Pang et al12 examined risk factors for recurrence after closed reduction and found that Fielding type 1 and chronic subluxations yielded the highest risk of recurrence (75% and 80%, respectively). Given the chronicity of injury in the patient presented, we felt management in a neck orthosis alone would result in a high risk of recurrence. Interestingly, we found the patient's subluxation was still amenable to closed reduction in halo traction, limiting the need for significant open reduction maneuvers prior to fusion.
Several fixation options have been proposed for atlanatoaxial arthrodesis.26 Wire fusion was originally proposed; however, pseudoarthrosis and construct failure have been reported.27–29 Transarticular screw fixation has also been used but is technically demanding and may not be suitable in cases of aberrant vertebral artery anatomy.30 For this reason, obtaining a CT angiogram is essential in preoperative planning. The current authors used a Harms technique with polyaxial screws in the C1 lateral masses and C2 pedicles. This technique has shown several advantages over transarticular, such as a more superior and medial screw trajectory to reduce risk to the vertebral artery.30,31 In addition, it has been shown to be biomechanically stronger than transarticular fixation. With regard to intraoperative imaging, 3D fluoroscopy can be helpful to confirm reduction and screw placement. If this is unavailable, the authors recommend the use of tall bite blocks placed along the edges of the mouth bilaterally to allow for intraoperative open-mouth odontoid views.
Posttraumatic atlantoaxial rotatory stability is a rare injury but can be missed on standard radiographs. Adults who present with torticollis after a trauma should obtain a CT scan to examine for C1–C2 subluxation or dislocation. Closed reduction should be attempted; however, the chronicity of the injury may place it at high risk of recurrence if arthrodesis is not performed.
Footnotes
Disclosures and COI: Isaac Moss is a consultant and receives personal fees for Stryker (Kalamazoo, MI), Nuvasive (San Diego, CA), Spineart USA (Irvine, CA), and Pfizer Inc. (New York, NY).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.