

Abstract
Background This review outlines clinical data and characteristics of current Food and Drug Administration (FDA)–approved implants in cervical disc replacement/cervical disc arthroplasty (CDR/CDA) to provide a centralized resource for spine surgeons.
Methods Randomized controlled trials (RCTs) on CDR/CDA were identified using a search of the PubMed, Web of Science, and Google Scholar databases. The initial search identified 69 studies. Duplicates were removed, and the following inclusion criteria were applied when determining eligibility of RCTs for the current review: (1) discussing CDR/CDA prosthesis and (2) published within between 2010 and 2020. Studies without clinical data or that were not RCTs were excluded. All articles were reviewed independently by 2 authors, with the involvement of an arbitrator to facilitate consensus on any discrepancies.
Results A total of 34 studies were included in the final review. Findings were synthesized into a comprehensive table describing key features and clinical results for each FDA-approved CDR/CDA implant and are overall suggestive of expanding indications and increasing utilization.
Conclusions RCTs have provided substantial evidence to support CDR/CDA for treating single- and 2-level cervical degenerative disc disease in place of conventional anterior cervical discectomy and fusion.
Clinical Relevance This review provides a resource that consolidates relevant clinical data for current FDA-approved implants to help spine surgeons make an informed decision during preoperative planning.
Level of Evidence 5
- cervical, cervical disc arthroplasty
- cervical disc replacement
- anterior cervical discectomy and fusion
- degenerative disc disease
- myelopathy
Introduction
Until recently, anterior cervical discectomy and fusion (ACDF) had been the customary surgical treatment option for patients with symptomatic cervical degenerative disc disease (DDD).1,2 Although ACDF has been widely accepted as an efficacious treatment for radiculopathy or myelopathy secondary to cervical DDD, the incidence of adjacent segment disease (ASD) postoperatively remains a concern.3 This significant limitation has since driven the search for treatment alternatives that can provide clinical outcomes similar to ACDF while preserving motion at the operative levels.
Over the past 2 decades, cervical disc replacement/cervical disc arthroplasty (CDR/CDA) has gained considerable traction as an alternative treatment option to ACDF. CDR shares many indications with ACDF but offers superior preservation of native spinal kinematics.4 This characteristic feature is thought to be protective against the development of ASD because it minimizes aberrant distribution of mechanical forces unto structures adjacent to the operative levels.5 This theoretical advantage has driven substantial interest in the translation of these concepts into clinically relevant applications.
As such, many randomized controlled trials (RCTs) have been conducted to compare CDR to ACDF. Park et al assessed cervical spine kinematics following ACDF and CDR in a prospective RCT and found that CDR significantly improved the restoration of lordotic alignment and disc height while maintaining preoperative translational and angular motion at the operative level.6 McAfee et al performed a meta-analysis of 4 prospective multicenter RCTs involving 1226 patients. Their analysis demonstrated superior long-term clinical outcomes and survivorship associated with CDA relative to ACDF.7 Similarly, in a meta-analysis of 18 RCTs, Gao et al reported greater clinical efficacy with CDR over ACDF in treating single-level cervical DDD across a number of outcome measures including visual analog scale neck and arm pain scores, neurological function, postoperative range of motion, and need for additional surgery.8
As increasing evidence surfaces to corroborate the clinical success of CDR, indications continue to expand as well.1 CDR was initially used to treat single-level cervical DDD but has since extended its application to 2-level cervical pathologies in light of supporting literature.2,9–11 As CDR continues to establish itself as a viable treatment option for cervical pathology, the authors of this study felt it was important to perform a thorough review of this procedure. The aim of this review study was 3-fold: (1) to discuss the background of CDR and its potential benefits compared with anterior discectomy and fusion, (2) to discuss the history of currently and previously available CDR prostheses and depict all Food and Drug Administration (FDA)–approved devices in a table format, and (3) to highlight all RCTs conducted comparing ACDF to CDR in a readily accessible, synthesized table. The main purpose of this article is to serve as a resource for spine surgeons to quickly refer, in table format, FDA-approved CDR implant characteristics and the available clinical data for each CDR implant.
Materials and Methods
Search Strategy
In July 2020, a search using PubMed, Web of Science, and Google Scholar was conducted to identify RCTs on CDR/CDA. The following Boolean search terms were used to identify studies of interest: ([CDR OR CDA OR total disc replacement OR total disc arthroplasty] AND [RCT]). As such, studies published between 2010 and 2020 were eligible for inclusion. The same search terms were used for each database, and the syntax was adjusted accordingly. The reference lists of all included studies were also reviewed. Two authors (D.R. and S.S.) independently reviewed each article, and any discrepancies were discussed by an arbitrator (K.A.) until a consensus was reached. D.R. and S.S. performed data extraction once the list of included studies was finalized.
Selection Criteria and Data Collection
Overall, the initial search identified 69 studies. Duplicates were removed, after which the following search criteria were applied (1) studies discussing a CDR prosthesis, (2) published within the last 10 years, and (3) written in the English language. The full text was reviewed if any discrepancies arose while parsing through the studies. Studies were excluded if they were (1) case studies, (2) book chapters, (3) animal and/or nonhuman models, and (4) non-RCTs. RCTs that did not measure clinical outcomes were also excluded. For example, some studies only assessed radiographic outcomes and were therefore excluded. RCTs that were published from earlier results of the same initial trial were also excluded. A total of 34 studies met inclusion and exclusion criteria and were included in the review (Figure). Characteristics of CDR were prespecified and included the manufacturer, images and x-rays of the implant, articulating materials, center of rotation, internal fixation methodology, FDA approval characteristics, magnetic resonance imaging compatibility, and disc height availability. Finally, a comprehensive table highlighting the key features and results of each study was created.
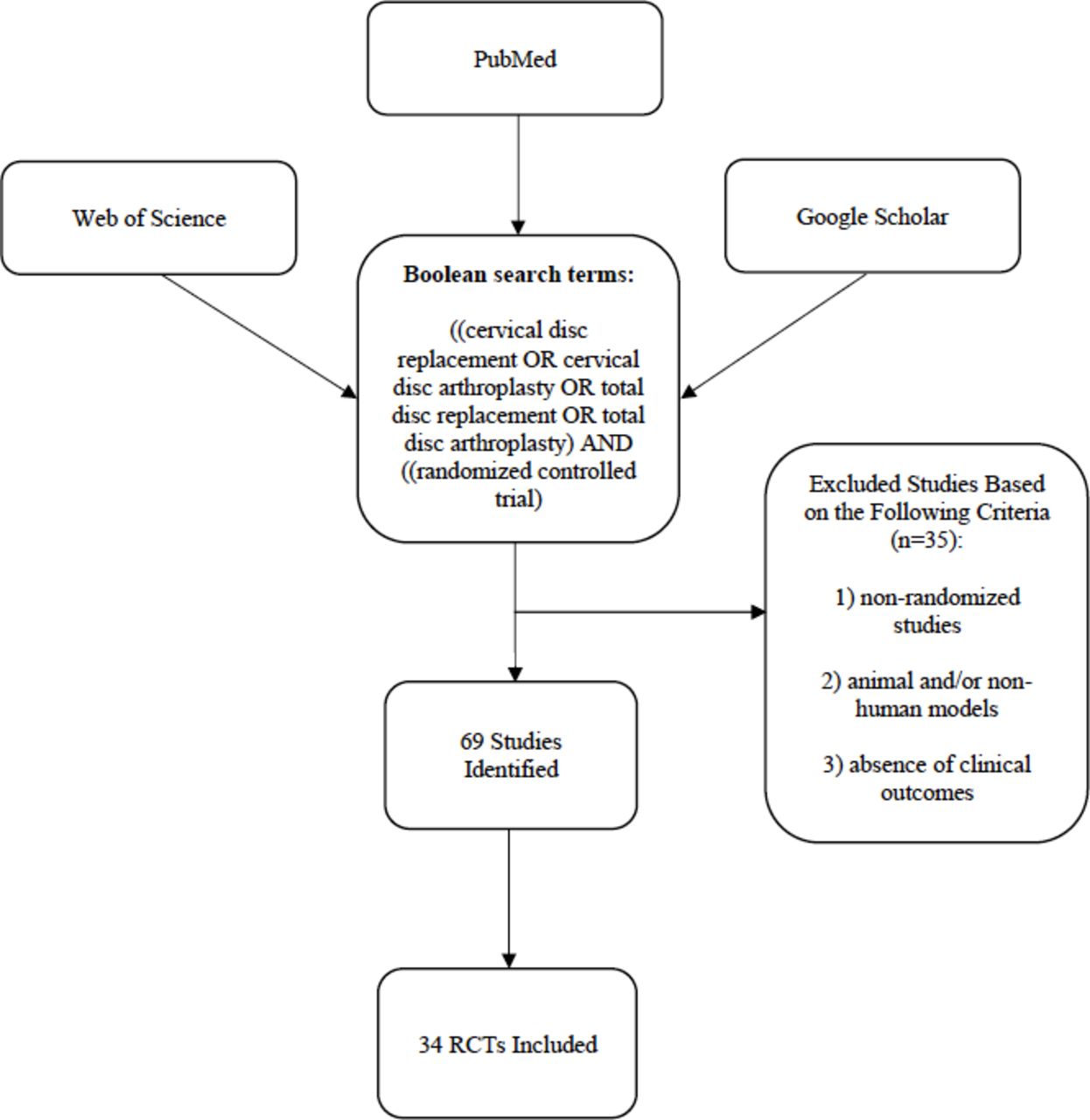
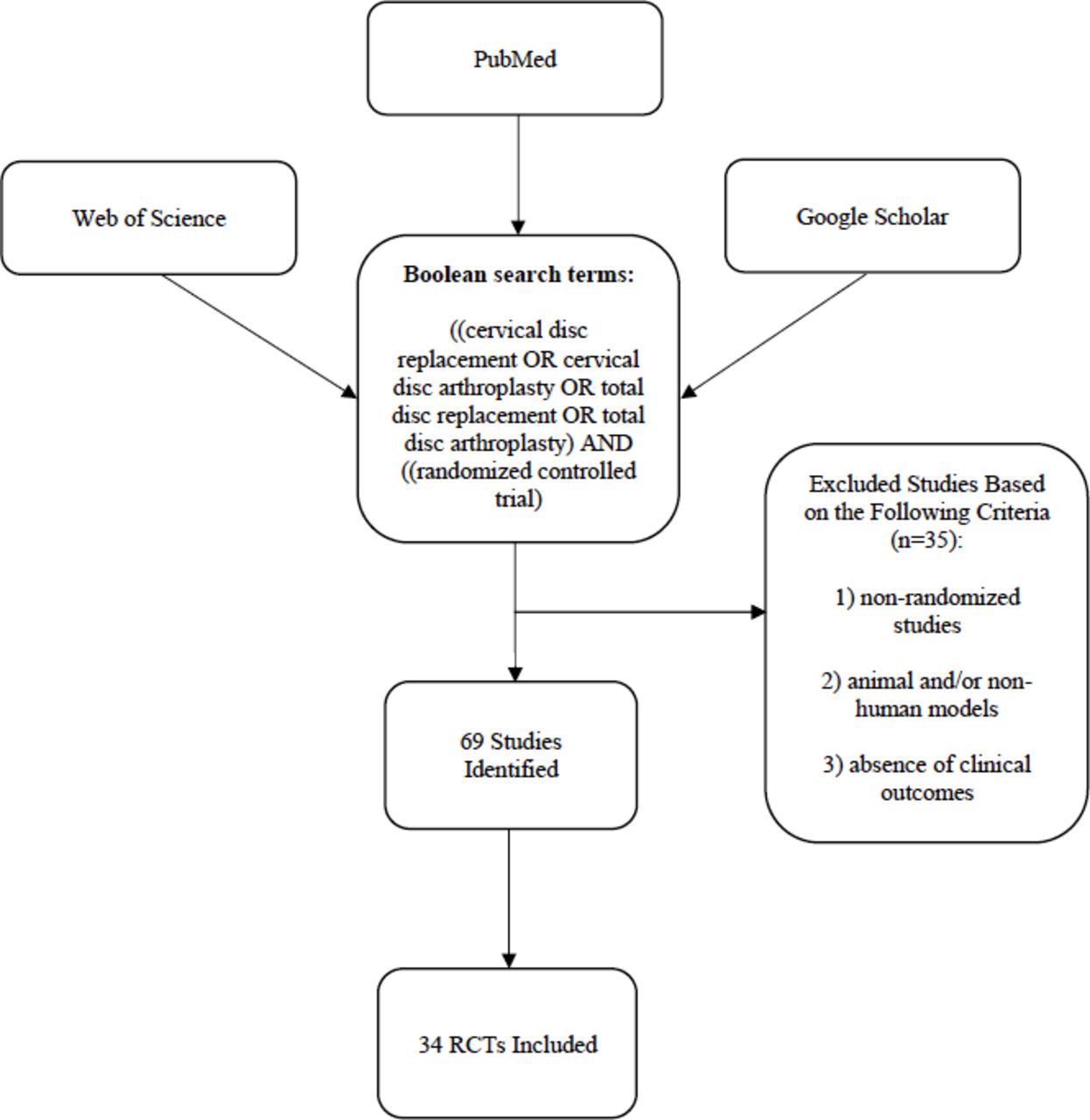{kind=link}
Flowchart of recorded articles related to randomized controlled trials comparing cervical disc arthroplasty to anterior discectomy and fusion.
Results
CDR History
Although CDR has only gained substantial support in recent years, its history dates back to the 1960s. Disc replacement was first introduced in 1966 by Swedish surgeon, Ulf Fernstrom. His spherical stainless steel prosthesis aimed to preserve mobility and restore disc articulation and height.12 This precursory model, however, was associated with hypermobility of adjacent segments, implant migration, subsidence, and vertebral body erosion.12 In 1989, B.H. Cummins introduced a second generation of disc replacements through a stainless steel ball-and-socket design. This prosthesis, however, yielded substandard preliminary results in a study of 18 patients, in which 100% of patients experienced lasting dysphagia, 22% fixation failure, and 6% instability.12,13 Although presumed unsuccessful, this implant prompted the inception of the first successful cervical disc prosthesis. The Frenchay cervical disc, an iteration of Cummins’s precedent model, demonstrated favorable results in a 2002 study and was subsequently developed into the Prestige ST Cervical Disc, one of the several cervical disc implants gaining FDA approval in the 2000s.14 A current list of all FDA-approved CDR prostheses with accompanying clinical and radiographic images is listed in Table 1.
Summary of current FDA-approved cervical disc arthroplasty devices with clinical and radiographic image examples.
CDR Advantages
CDR offers several advantages over ACDF when treating single- and 2-level cervical DDD. The placement of artificial disc implants in lieu of rigid fusion constructs preserves motion at operative levels and facilitates normative load-sharing at index levels and their adjacent segments. Taken in conjunction, these features likely account for the notably lower incidence of ASD following CDR as compared with ACDF. In a meta-analysis of 11 RCTs comparing CDR and ACDF outcomes in treating single- and 2-level cervical DDD, Xu et al found significantly reduced ASD incidence and reoperation requirement with CDR use.15 With respect to long-term outcomes, Ghobrial et al similarly found significantly decreased development of symptomatic ASD requiring surgery in the cervical total disc replacement cohort compared with ACDF (6.9% vs 11.7% respectively) at 7 years.16
Biomechanical advantages seen with CDA also translate into improved clinical outcomes. Findlay et al affirmed this notion through a meta-analysis of 14 studies showing superior clinical outcomes—from 2 to 7 years—with respect to Neck Disability Index (NDI) and 36-Short-Form Health Survey (SF-36) physical component scores, as well as overall patient satisfaction.6 Another meta-analysis conducted by Zhu et al further attributed superior NDI scores in addition to a safer risk profile. ACDF, however, was associated with shorter operative times and noninferiority across blood loss, hospital length of stay (LOS), and requirement for additional procedures.17 Tables 2 and 3 provide a concise overview of design features and published outcomes from RCTs associated with various cervical disc implants.9,10,18–47
Overview of randomized controlled trials on cervical disc arthroplasty.
Summary of cervical disc arthroplasty randomized controlled trials.
Longitudinal evidence further indicates CDR as a more cost-effective treatment relative to conventional ACDF. Radcliff et al performed a 7-year health economics analysis demonstrating superior cost efficiency with CDR for the treatment of single-level cervical DDD, whereby CDR was associated with a mean cost savings of $12,789 per patient compared with ACDF.49 These findings lend support to a surgical decision model proposed by Qureshi et al, which established 14 years as the minimal time period in which CDR function needs to be preserved to maintain greater cost-effectiveness over ACDF.31
CDR and Heterotrophic Ossification
Heterotrophic ossification (HO) frequently occurs after CDR and is thought to be a sequelae of either extensive vertebrae endplate preparation or colli muscle debridement. Arthrodesis resulting from HO induces aberrant loading across the index and adjacent segments, leading to decreased range of motion and increased prosthesis failure. Despite these alternations to spinal kinematics, the overall prevalence of ASD after CDR remains relatively low compared with ACDF.50 Similarly, in line with other arthroplasty procedures, HO progresses slowly in CDR, displaying an incremental increase in prevalence over time. In a meta-analysis of 8 articles examining the prevalence of HO at 1 and 2 years after CDR, Chen et al reported the pooled prevalence of HO to be 44.6% and 58.2% at 1 and 2 years, respectively.48 Over a more extensive follow-up period, Sheng reported pooled prevalences of 50%, 60%, and 70% at 1 or 2, 5 or 6, and 10 years postoperatively.50
The association between CDR and the development of HO has yet to be fully elucidated, but evidence suggests that the incidence of HO may be contingent on the biomechanic properties of individual prostheses. In a retrospective analysis, Yi et al compared the HO incidence of ProDisc-C, Mobi-C, and Bryan prosthesis in 170 patients with a minimum of 12-month follow-up, revealing that Bryan had the lowest occurrence of HO, while ProDisc-C had the highest.51 A prior study by Zeng et al that compared HO incidence between the same 3 prostheses in patients 4 years postoperatively also found HO to occur most with the ProDisc-C and least with the Bryan prosthesis.52 The Bryan and Mobi-C allow more degrees of freedom of motion compared with the ProDisc-C, which is a fixed-core prosthesis. This distinction may contribute to increased stress at the prosthesis-endplate interface, potentially contributing to the development of HO in more constrained implant designs.
Discussion
When appropriately indicated, CDR may provide a beneficial alternative to conventional ACDF for the treatment of degenerative cervical spine pathology on account of its motion-preserving features. This notion has been widely and consistently reported across prior studies and bypasses the major limitations imposed by ACDF.7,53 While indications remain relatively confined for CDR, increasing adoption of this technique will lend to expanding indications for its use in multilevel pathologies.
Future Directions—Expanding Indications
Investigational device exemptions (IDEs) with strict inclusion and exclusion criteria are required for FDA approval. These criteria are utilized by the FDA to establish appropriate indications and contraindications in the clinical setting.54 Common indications and contraindications for current CDA implants are listed in Table 4.55–57 Despite strict criteria set by device companies and the FDA, surgeons have been expanding their indications for CDA in recent years.
Most common indications and contraindications for cervical disc arthroplasty.
Promising outcomes seen consistently across studies have contributed to increasing off-label uses of CDR.58 Routine utilization of CDR for extensive multilevel cervical disc pathology may potentially be on the horizon with forthcoming data to assess its clinical efficacy in these settings. In a recent study published in 2020, Gornet et al reported on 7-year outcomes for 3- (contiguous and noncontiguous) and 4-level (contiguous) CDA. The authors reported favorable results across all patient-reported outcome measures in tandem with low reoperation rates (3.6%) in a cohort of 139 patients.59 It is important to note, however, that this study did not include an ACDF cohort for comparison and was therefore not listed among the RCTs tabulated within the present study. Chang et al conducted a comparative analysis of patients undergoing either 3-level CDR or ACDF, where both groups achieved similar outcomes and complication rates; CDR nonetheless preserved a greater postoperative range of motion relative to the ACDF group.60 In a bibliometric analysis of 957 articles concerning CDA, Tu et al noted an exponential rise in publications pertaining to multilevel CDA (>2 levels) over the past decade, although the majority of these were composed of 2-level procedures.61 Nonetheless, studies on 3-level applications have seen a recent and sustained increase from 2017 to the present. This trend is believed to signify the growing acceptance of CDA as a viable surgical alternative for multilevel disease among spine surgeons, particularly in geographic regions with less stringent indications for CDA. Interestingly, research and application of multilevel CDA beyond currently established indications continues to expand in Asia and Europe, yielding precursory evidence to support its use as a safe and effective alternative in select patients. Although preliminary data on multilevel CDR appears promising, additional high-quality RCTs with longer follow-up intervals are required for a comprehensive, longitudinal assessment of its clinical efficacy.
Hybrid surgery is an emerging concept that combines features of ACDF and CDR. Existing literature on this novel strategy has been in part limited by the exclusion of patients with preexisting fusions in prior RCTs.8,11,31 Support surrounding this technique is driven by the idea that patients with multilevel cervical pathologies have varying degrees of degeneration at each level.62 As such, a hybridized approach incorporating both fusion and arthroplasty elements may be applied independently across affected levels to provide tailored treatments suited to patients’ unique pathologies.58 A recent retrospective database analysis comparing CDA, ACDF, and hybrid surgeries found no significant differences in 30-day postoperative complications or unplanned readmissions, although patients who underwent hybrid surgeries had shorter LOS on average. Conclusions from this study, however, should take into consideration that patients in the hybrid surgery cohort were younger and had fewer comorbidities.63 Wang et al compared 3-level variations across 64 patients with cervical DDD in the context of hybrid procedures using 2 cohorts: single-level ACDF with adjacent CDR or single-level CDR with contiguous 2-level ACDF of caudal segments. Both hybrid techniques produced outcomes to adequately support their safety and efficacy in clinical practice but also revealed distinctive features relative to one another. Single-level CDR with contiguous 2-level fusion achieved greater accuracy with correction of cervical lordosis but was associated with higher incidence of heterotopic ossification, while single-level fusion with 2-level CDR maintained superior range of motion.53 With only preliminary evidence to corroborate the use of cervical hybrid constructs, further longitudinal studies such as ZimVie’s Mobi-C Hybrid Surgery Trial—following recent FDA approval of its IDE status in September 2023—are warranted to assess the long-term impact of hybrid techniques in the clinical setting.64 ,60
Conclusions
CDA was developed to provide a motion-preserving alternative to ACDF. Numerous RCTs have demonstrated the procedure to be as safe and effective as ACDF for the treatment of radiculopathy and myelopathy refractory to conservative management of cervical DDD. As further evidence arises to corroborate its utility in various clinical settings, CDA indications and utilization will increase correspondingly. Establishing a centralized resource that consolidates relevant details and clinical data of current FDA-approved implants would help spine surgeons make better-informed decisions during preoperative planning.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests No funding was received for this study. Djani Robertson, Andy Ton, Michael Brown, Shane Shahrestani, and Emily S. Mills have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccentrial Robotics for lectures and presentations.
Ethics Approval Informed consent was waived and institutional review board (IRB) approval was not required because no patients were involved in this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.