


Abstract
Background Lumbar interbody fusion has become a well established method to diminish axial back pain as well as radiculopathy in patients with degenerative disc disease, stenosis, and instability. The concept of indirect decompression of the neural foramen and spinal canal while performing fusion became popular in the mid 1990’s with description of ALIF techniques. Morphometric analysis confirmed the extent of decompression of posterior elements with interbody height restoration. In an attempt to diminish potential complications associated with anterior or posterior approaches to the spine for interbody fusion, and with the hope of accomplishing fusion in a less invasive manner, lateral lumbar interbody fusion has become quite popular. This transpsoas approach to the disc space has been associated with a high incidence of neurologic complications. Even though this is the first technique to routinely recommend EMG monitoring to increase safety in the approach, neurologic injuries still occur. A newer oblique lateral lumbar interbody (OLLIF) approach has recently been described to lessen the incidence of neurologic injury. This technique also advocates use of EMG testing to lessen neurologic trauma. In spite of this precaution, neurologic insult has not been eliminated. In fact, even in patients whose electrical stimulation thresholds suggested a safe entry space into the disc, transient dysaesthesia continues to occur in 20-25 percent of cases.
Purpose This pilot study reflects data and observations of a subset of patients treated with endoscopic foraminotomy preceding oblique lateral lumbar interbody fusion (OLLIF) to assess specifically potential improvements in dysaesthesia rates.
Methods A select subset of patients undergoing OLLIF failed to meet electrodiagnostic criteria for safe disc access through Kambin’s triangle. These patients underwent an endoscopic foraminotomy and exiting nerve decompression prior to discectomy, endplate preparation and cage insertion.
Results Dysaesthesia did not occur in these patients whom otherwise would have likely been at risk for neurologic deficit.
Conclusions These findings suggest that patients at risk for neurologic insult during oblique lateral lumbar interbody fusion can be protected by foraminoplasty.
- Oblique Lateral Lumbar Interbody Fusion
- endoscopic foraminoplasty
- Dysaesthesia
- Dysaesthesia rates in OLLIF
- Lumbar interbody fusion
Introduction
Lumbar interbody fusion has become a widely accepted treatment for painful conditions of the lumbar spine from degenerative disc disease, instability, and stenosis.1 Axial back pain and radicular symptomatology can be dramatically improved from interbody fusion. When outcomes are evaluated, higher fusion rates and improved pain reduction can be anticipated than from posterolateral fusion alone.2
The benefits of interbody fusion indirectly decompressing the neural elements have been known since the 1990s. Morphometric assessment of neural canal and neural foraminal dimension after anterior lumbar interbody fusion supports the concept of indirect decompression.3
Interbody fusion does pose a risk for complications. In an attempt to lessen the risk of severe complications that may occur with anterior or posterior approaches to the spine and to offer less invasive surgical alternatives, lateral lumbar interbody fusion has become popularized. Although this technique recommends electromyography (EMG) monitoring to safely transverse the psoas muscle and lumbar plexus, nerve root injury remains a concern. In a large review of 919 lumbar lateral interbody fusion (LLIF) levels performed at the Hospital for Special Surgery in New York, Lykissas et. al. reported an incidence of sensory deficit in 38% of patients, motor deficits in 23.9% of patients, and anterior thigh and groin pain in 38.5% of patients.4 While many published series, such as that reported by Rodgers reviewing 600 cases of lateral lumbar interbody fusions, never discuss dysaesthesia at all,5 studies where this problem is considered routinely have reported dysaesthesia rates from 20-60%.6, 7 Residual sensory deficits at one year post-op are typically between 1-3% and motor weakness between 2-3%.6, 8
Oblique lateral lumbar interbody fusion is a newer technique employed to achieve interbody fusion. This is also a bone and muscle preserving minimally invasive technique. Although the incidence of neurologic injury is lower than in lateral interbody fusion cases, neural injury remains a concern. This approach utilizes Kambin’s triangle to gain access to the disc space for discectomy and endplate preparation. Of course, the superior margin of this space is the exiting nerve root. As such, due to nerve root retraction or tension, nerve root irritation is not uncommon. In a retrospective analysis of our first 55 consecutive cases, transient dysaesthesia occurred between 20-25% of cases. Since the technique also recommends utilizing EMG monitoring to gain access safely to the disc space, sensory neurologic injury lasting greater than 3 months has an incidence less than 1% and motor deficit is even less frequent. Our dysaesthesia occurrences involved the L5-S1 level almost exclusively, although one patient treated with an L2-3 and L3-4 OLLIF did experience transient dysaesthesia.
The results of this study suggest that foraminotomy lessens the incidence of dysaesthesia in patients who failed to meet EMG safety thresholds. This technique can also be utilized for patients with facet hypertrophy and foraminal stenosis.
Method
Between 2012 and 2013, 55 OLLIFs were done; each augmented with posterior pedicle screw fixation. Each patient had failed conservative treatment. Treatments included medications, spinal injections, and physical therapy over a minimum of 6 months. All suffered from low back pain, 36 patients had back pain with radiculopathy. Spondylolisthesis (grade 1-2) was noted in 5 patients. Stenosis was present in 28 cases. None of the patients were operated on for DDD without stenosis or instability. In 5 additional patients this procedure was not offered due to anatomic considerations including high pelvis with narrow ilium (3 patients) or marked facet overgrowth with foraminal stenosis (2 patients). These 5 cases were managed with transforaminal lumbar interbody fusion (4 cases) or Axialif (1 case). These set of patients were not included in this study.
The subject patients of this study were a very limited cohort. These cases were considered appropriate for OLLIF by radiographic criteria. However, at the initiation of the case, a safe neurologic EMG threshold could not be obtained to access the disc through Kambin’s triangle. The protocol for this approach mandates that no neurologic response should be obtained from a 3 milliamp stimulus from the ball tipped EMG probe. If a stimulus response is absent above 3 milliamps, a safe zone of at least 1.5 mm exists past the exiting nerve root. Five patients failed to meet this safety threshold. In all five cases, an endoscopic foraminotomy and nerve root decompression was done as the initial step.
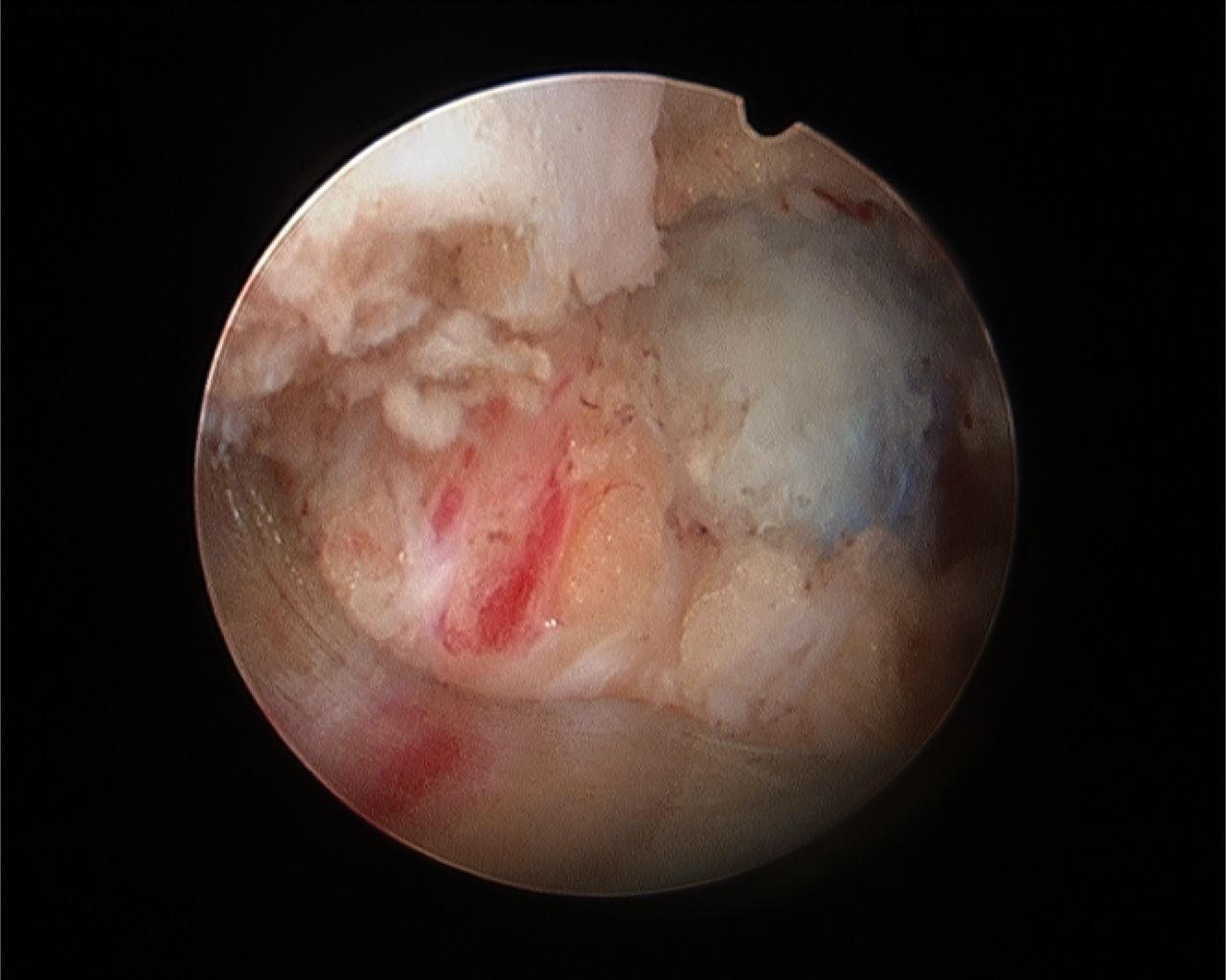
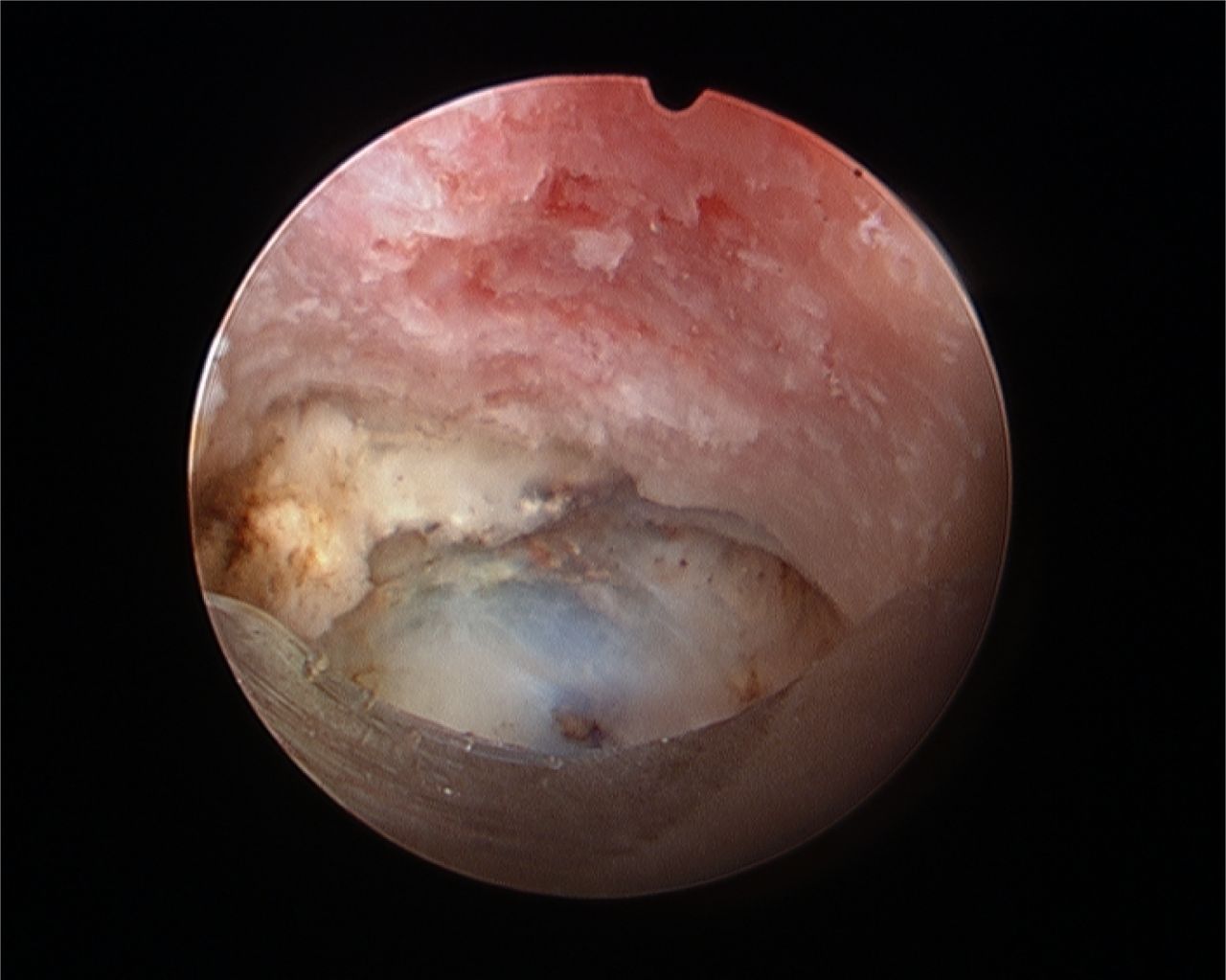
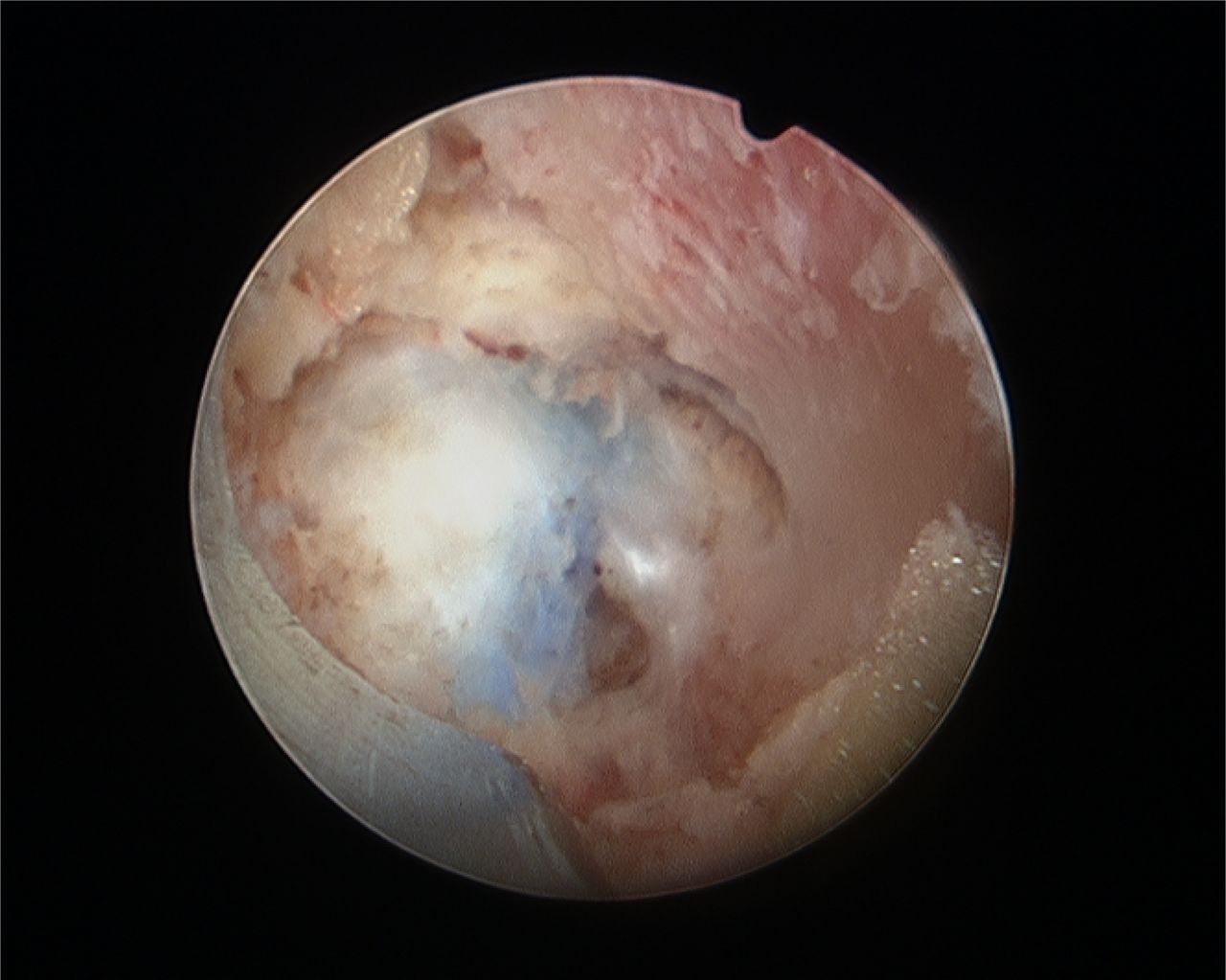
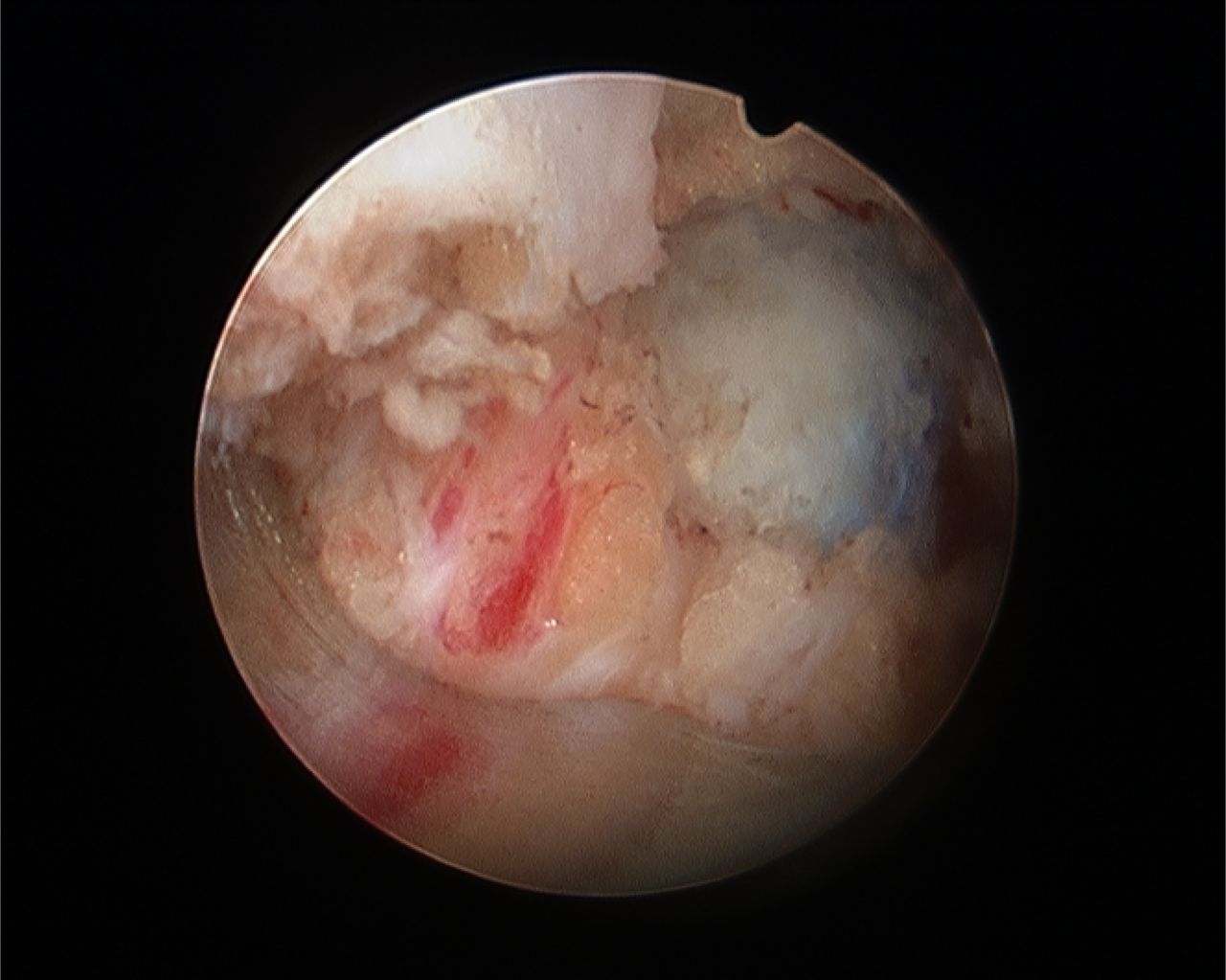
The authors’ technique for foraminal decompression is as follows: a targeting needle is placed under fluoroscopic guidance to the junction of the pedicle and the base of the superior articular process. A guide wire is placed through the needle. Next, blunt muscle dilation is done over the guide wire so an endoscopic cannula can be passed and anchored on the SAP. The cannula is then turned so the tang protects the exiting nerve root. Endoscopic burrs, reamers, and kerrison ronguers increase foraminal surface area by removing the lateral and anterior portion of the SAP from a caudal to cephalad direction. The facet joint capsule and lateral portion of the ligamentum flavum are removed. Finally, the decompression is continued in a cephalad direction to include the deep portion of the inferior articular process to free the exiting nerve root (Figure 1, Figure 2, Figure 3). This effectively increases the dimensions of Kambin’s triangle allowing safe access for annulotomy and placement of a 9mm access cannula for completion of OLLIF procedure.

Exposed disc for OLLIF insertion
Exiting nerve root cephalad to disc
Widened neuroforamen & hole in disc from EMG probe
Results
The five patients treated with combined foraminoplasty nerve root decompression followed by OLLIF have been followed at 1 week, 3 weeks, 6 weeks and 3 months post operatively by interview and examination. None of these patients experienced any neurologic complaint of paraesthesia, dysaesthesia, or weakness after surgery. All had a normal neurologic examination.
Discussion
Neurologic injury remains a common occurrence after lumbar fusion surgery whether by TLIF,9 PLIF,10 or LLIF.11
OLLIF, while preserving the minimally invasive benefits of LLIF and decreasing the incidence of neurologic injury, has not eliminated transient dysaesthesia and hypaesthesia.
In this unique subset of patients, whose numbers are small due to the unique circumstances required to be treated in this manner, neurologic injury was avoided. This is of particular interest in light of the low stimulation threshold elicited before decompression that would have likely predicted potentially severe neurologic injury had the initial intended procedure been completed.
We recognize the limitations of this study. The criteria for patient inclusion was so strict that the number of enrollees in this cohort are too small for any statistical analysis. Furthermore, no randomization was done, as it is not possible to preoperatively predict who will fail EMG screening for this procedure.
This work is submitted for several reasons. One is to introduce an alternative minimally invasive “bail out” option for patients intended for OLLIF who do not meet EMG thresholds for safety. The hope is to not have to revert to a more painful bone sacrificing TLIF procedure. Another is to stimulate interest in a pilot study to prompt physicians to evaluate OLLIF combined with foraminal decompression to study the effects on neurologic injury. Lastly, we can now show a method to increase the indications for OLLIF surgery now having an ability to help patients with foraminal stenosis and facet overgrowth who previously would have not been able to benefit from this technology.
Disclosures
Dr. Katzell has consulting and royalty agreements and owns stock and stock options in Amendia, Inc.
- Copyright © 2014 ISASS - International Society for the Advancement of Spine Surgery
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.