


ABSTRACT
Background: The minimally invasive cortical trajectory screw (MidLF) technique has been described accompanied with posterolateral interbody fusion (PLIF). We present our 2-year results of a hybrid technique to show that using transforaminal interbody fusion (TLIF) rather than PLIF in conjunction with MidLF is a less invasive and safe technique.
Methods: We retrospectively identified 25 patients who underwent MidLF with TLIF from July 2015 through September 2017. The surgical technique was the same for each, with radiological, clinical, and patient-reported outcome data collected and analyzed at a 2-year follow-up.
Results: The cohort showed a mean age of 55 (35–85) years. The length of hospital stay was between 1 and 4 days, with an average of 2.7 days. Postoperatively, lordosis across the motion segment fused increased by a mean of 7.3° (0°–24°), mean pelvic incidence was 53°(31°–80°), and pelvic tilt reduced by an average of 3.5° (0°–11°). The Oswestry Disability Index improved from 34 preoperatively to 19 postoperatively. Visual analogue pain score–leg improved by 4.7 points, from 6 down to 1. One patient showed delayed wound healing. There were no incidences of neurological injury or durotomy.
Conclusions: Our data suggests that MidLF with TLIF is both less invasive than traditional techniques and safe. It restores lordosis, requires less exposure and retraction of neural elements than the more widely used PLIF, and shows early discharge and satisfactory medium-term patient-reported outcomes.
Level of Evidence: 3.
Clinical Relevance: The MidLF technique with PLIF is less invasive than traditional techniques, restores alignment and shows satisfactory medium term results.
INTRODUCTION
The indications for lumbar fusion are broadening through increasing understanding of pathology and instrumentation, and surgeons are treating patients with comorbidities that were previously contraindications to surgery. Although pedicle screws are the most commonly used anchors, they are not free from complications and they require a wide approach to ensure safe insertion and a thorough decompression.1–4 A recent development has been minimally invasive cortical trajectory screws (MidLF) first described by Santoni et al5 in 2009. MidLF relies on the infero-medial to supero-lateral trajectory of screws through a less invasive midline incision to achieve purchase into the posterior elements of the vertebra. Several studies have since shown that this technique is effective in reducing screw pullout and achieving fusion whilst requiring much less dissection than the standard technique and reducing length of stay and intraoperative blood loss.2,3,6–8 In addition, several studies have shown that it is beneficial to include interbody fusion alongside posterolateral fusion over posterolateral fusion alone in degenerative disease.9–12 In order to achieve this, surgeons using a posterior approach have the option of either posterolateral interbody fusion (PLIF) or transforaminal interbody fusion (TLIF) with evidence suggesting that the safety, biomechanics, and cost are superior with TLIF.13–19 This retrospective study investigates the 2-year results of using the TLIF technique in conjunction with MidLF in order to determine whether the technique is less invasive, safe, and associated with good patient outcomes.
MATERIALS AND METHODS
A retrospective case series method was used. From July 1, 2015 to September 30, 2017, all patients treated by the senior author with a primary interbody fusion underwent MidLF accompanied with TLIF. Each patient with a minimum of 2 years of follow-up was retrospectively identified and included in the analysis. Data were collected regarding demographics, diagnosis, operated levels, wound length, depth of retractor blade used, length of inpatient stay, and dimensions of the interbody fusion device. The senior author assessed the pre- and postoperative lumbar lordosis, pelvic incidence, pre- and postoperative pelvic tilt on pre- and postoperative 36-inch spinal radiographs. Complications were recorded and the Oswestry Disability Index and visual analogue scale (VAS) were assessed both pre- and postoperatively for each case.
Statistical Methods
Analysis was carried out using STATA v14.0 (StataCorp, College Station, Texas). Demographic characteristics were described using assessment of central tendency and spread. Changes in radiological parameters were analyzed through a paired Student t test with Shapiro-Wilk W test used to prove normality for continuous data. Postoperative complications were recorded categorically.
The procedures were all carried out by the senior author. A Gen 2.0 retractor system (Medtronic, Memphis, Tennessee) of the appropriate size was placed in the wound and the light source attachment used. A midline decompression and bilateral facet excision was carried out under direct vision. Cortical trajectory screws (Solera 4.75, Medtronic) were then placed into the neural arches of the target levels. These were then used to distract to facilitate insertion of a TLIF device (Crescent Titanium TLIF cage, Medtronic), which was packed with a mixture of autologous and demineralized bone matrix (Grafton DBM, Medtronic) prior to insertion. Compression was then applied across the segment to achieve the final lordosis. Cobalt chrome rods were used to maintain the final position. Additional autologous and Grafton DBM with petalization was used in the contralateral interlaminar gap to encourage fusion.
RESULTS
Between July 1, 2015, and September 30, 2017, 34 levels of MidLF with TLIF in 25 patients were performed. Seventeen patients had spondylolisthesis and the remainder had degenerative stenosis. Incomplete perioperative data was available for 4 patients, and 16 patients declined to provide a complete set of patient-reported outcome data. The mean age of patients was 55 years (range: 35–85 years). The length of hospital stay was between 1 and 4 days, with an average of 2.7 days.
The mean length of the incision was 45 mm per level (95% confidence interval [CI]: 42–48 mm) and the mean depth of retractor blades used was 790 mm (range: 600–1100 mm). The mean cage height and length used was 10.45 mm (range: 8–15 mm) and 28.6 mm (range: 25–30 mm), respectively. Lordosis across the fused segment increased by a mean of 7.5° (95% CI: 5.0°–9.9°, P < .001) from a mean of 14° (95% CI: 12°–17°) preoperatively.
Mean pelvic incidence was 53° (95% CI: 48°–58°). Pelvic tilt reduced by a mean of 2.8° (95% CI: 1.4°–4.2°, P < .001). For the 9 patients for whom data were available, the VAS-leg score improved by an average of 4.7 points (P < .01). In the 9 patients for whom data were available, the Oswestry Disability Index improved from a mean of 33 preoperatively to 19 postoperatively (P =.01).
Over the 2 years of follow-up, 2 patients went on to have additional procedures for adjacent-level disease; one for known preexisting stenosis, the second for a distal pars fracture following interspinous fusion without interbody cage below the index level. One patient showed delayed wound healing. There were no incidences of neurological injury or durotomy.
DISCUSSION
MidLF is a technique that is less invasive than traditional open decompression and posterolateral fusion, and is associated with less morbidity, blood loss, and length of stay.2,6 Due to retraction of the neural elements, using a PLIF device carries an appreciable risk of neurological injury.13,15,20 TLIF is an alternative to PLIF which is at least equivalent in terms of fusion rates and outcomes, and in several studies has been shown to have a lower risk of durotomy and neurological injury and an improved correction of lordosis.17–19 Furthermore, Li et al showed that open TLIF is at least equivalent to minimally invasive TLIF, with the exception of blood loss due to a larger incision.21 As such, the evidence suggests that the optimal outcome would be associated with the use of TLIF with MidLF (Figure 1).
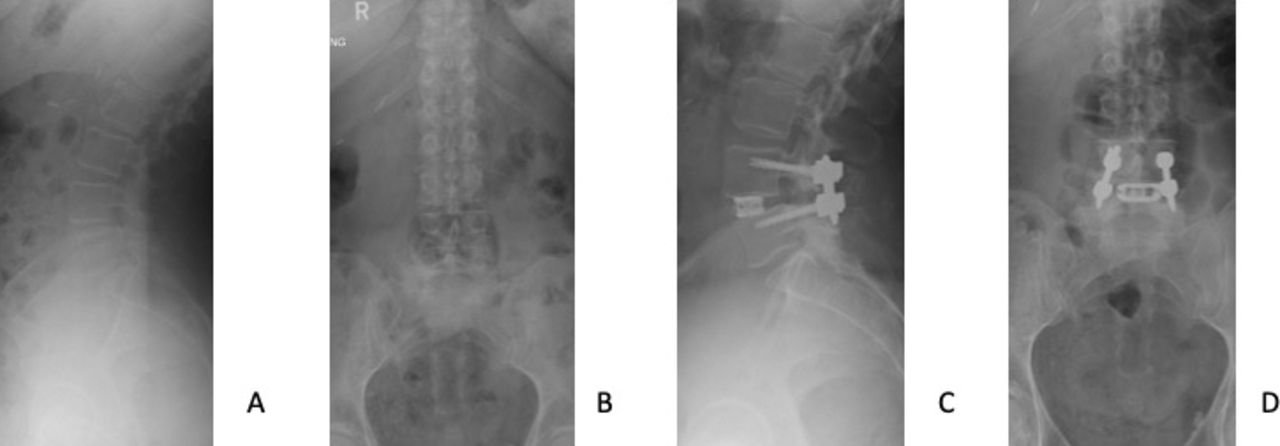
(A) The lateral and (B) anteroposterior radiographs of a patient requiring treatment for degenerative spodyloisis. (C) The lateral and (D) anteroposterior view of the final construct showing the minimally invasive cortical trajectory screw and transforaminal interbody fusion with restoration of lordosis and decompression of the foramen.
There are no randomized controlled trials assessing the effectiveness of TLIF and MidLF used in combination, although a study protocol has been recently published.22 Kasukawa et al published a case series in 2015 showing that, in their series of 10 patients who underwent TLIF following MidLF, blood loss and operative time were reduced when compared to TLIF in combination with minimally invasive or open pedicle screw placement.23 Our data take this one step further in showing that not only is this the case, but that the technique is safe and achieves the necessary lordosis to achieve spinal harmony.
Evidence suggests that pelvic incidence–lumbar lordosis (PI-LL) mismatch is a risk factor for failure of fusion in the degenerate spine.24 This study aimed to analyze the correction of segmental lordosis and describe what can be achieved with this technique rather than assess the influence of the PI-LL mismatch on the outcome, particularly in light of PI-LL mismatch being a simple measure of deformity correction subject to many other variables that influence its magnitude.
Our data show that this surgical strategy is less invasive than traditional techniques, restores lordosis, is not associated with postoperative complications or increased length of inpatient stay and that there are benefits in both pain and function. With experience of interbody fusion techniques, this modification to the MidLF procedure is straightforward to employ and brings with it the biomechanical, safety and therapeutic benefits of TLIF.
This study has several limitations including its retrospective methodology and relatively short follow-up period. Alongside this, the absence of a control group prevents direct comparison of the effectiveness of MidLF with TLIF with other techniques; this could be addressed with an interventional trial in the future.
CONCLUSION
MidLF is a recent technique that benefits from reduced surgical morbidity and biomechanical advantages. In this study, we have shown that MidLF with TLIF is less invasive than standard techniques, is safe, has a low rate of complications, and can give equivalent or better segmental lordosis when compared to a traditional open procedure.
Footnotes
Disclosures and COI: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The second author, Ian Harding, receives consultation fees from Medtronic Inc.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}