


Abstract
We provide a historical and technical perspective on the evolution of Kambin’s triangle as a safe working corridor for percutaneous access to the intervertebral disc to an anatomically expanded space to accommodate and facilitate open lumbar total joint replacement. The nearly 6-decade progression from intradiscal access in the intact lumbar spine to an enlarged working space following facetectomy to accommodate a transforaminal lumbar interbody fusion, and eventual further expansion via pedicle vertebral body osteotomy to support motion preservation with total joint replacement, represents a unique evolutionary pathway in surgical technique development. For each of these steps in evolution, we detail and provide the historical context of the corresponding surgical modifications required to expand the original anatomical boundaries of Kambin’s triangle. It is postulated that the introduction of machine learning technologies coupled with innovations in robotics, materials science, and advanced imaging will further accelerate and refine the adaptation of more complex, precise, and efficacious surgical procedures to treat spinal degeneration via this working corridor.
Introduction
One of the most salient structural and functional features of the vertebral column is to serve as a motion-protective encasement of the spinal cord and exiting nerves.1 Considering that the protection of these neural structures is paramount, the surrounding bony skeleton offers minimal access to the neural elements to avert penetration from extrinsic objects that could potentially harm the cord. Surgical access to the intervertebral disc space from a posterior approach is similarly obstructed.2
This article provides a historical and technical perspective on the evolution of Kambin’s triangle as a safe working corridor for percutaneous access to the intervertebral disc to an anatomically expanded space to accommodate and facilitate open lumbar total joint replacement (TJR).
Kambin’s Triangle: Identifying Posterior Intradiscal Access
In the early 1970s, Dr. Parviz Kambin was the first person credited in identifying a posterolateral access corridor in the lumbar spine that was large enough to accommodate instrumentation to allow for the percutaneous decompression of a bulging disc through a cannula.3 However, it took more than a decade for Kambin to publish a description of the boundaries of this eponymous anatomical configuration.4–6
With an entry point for the initial incision approximately 8 to 9 cm lateral of the midline, Kambin’s triangle is a distinct anatomical feature whose morphological boundaries include the exiting nerve root superiorly under the pedicle moving anteriorly laterally, the traversing nerve root and dural sac medially, and the superior endplate of the lower vertebral body inferiorly (Figure 1).5,7 Surgical approaches via this corridor are considered safe because it avoids important neurovascular structures.7 This corridor provided the ideal working channel for the initial development, refinement,8–10 and eventual widespread clinical adoption of percutaneous discectomy procedures to manage disc herniation.11 With this minimally invasive procedure and its endoscopic variants, the utilization of Kambin’s triangle allows the disc to be approached posterolaterally without the need for bone or facet resection, thus preserving spinal stability.12 Consequently, there is less damage to muscular and ligamentous structures, allowing for more rapid recovery and symptom amelioration, reduced hospital stay, and earlier return to activities of daily living.13

Anatomical rendering of Kambin’s triangle.
The identification of Kambin’s triangle also served as an ideal working channel for the delivery of epidural corticosteroids.14,15 It is considered the safest approach for this procedure.16 Needle-based pain management indications that utilize this access corridor have expanded and proliferated to include intradiscal restorative therapies, discography, and basivertebral nerve ablation, among other mainstream and developing procedures.17–19
Development of the Transforaminal Corridor
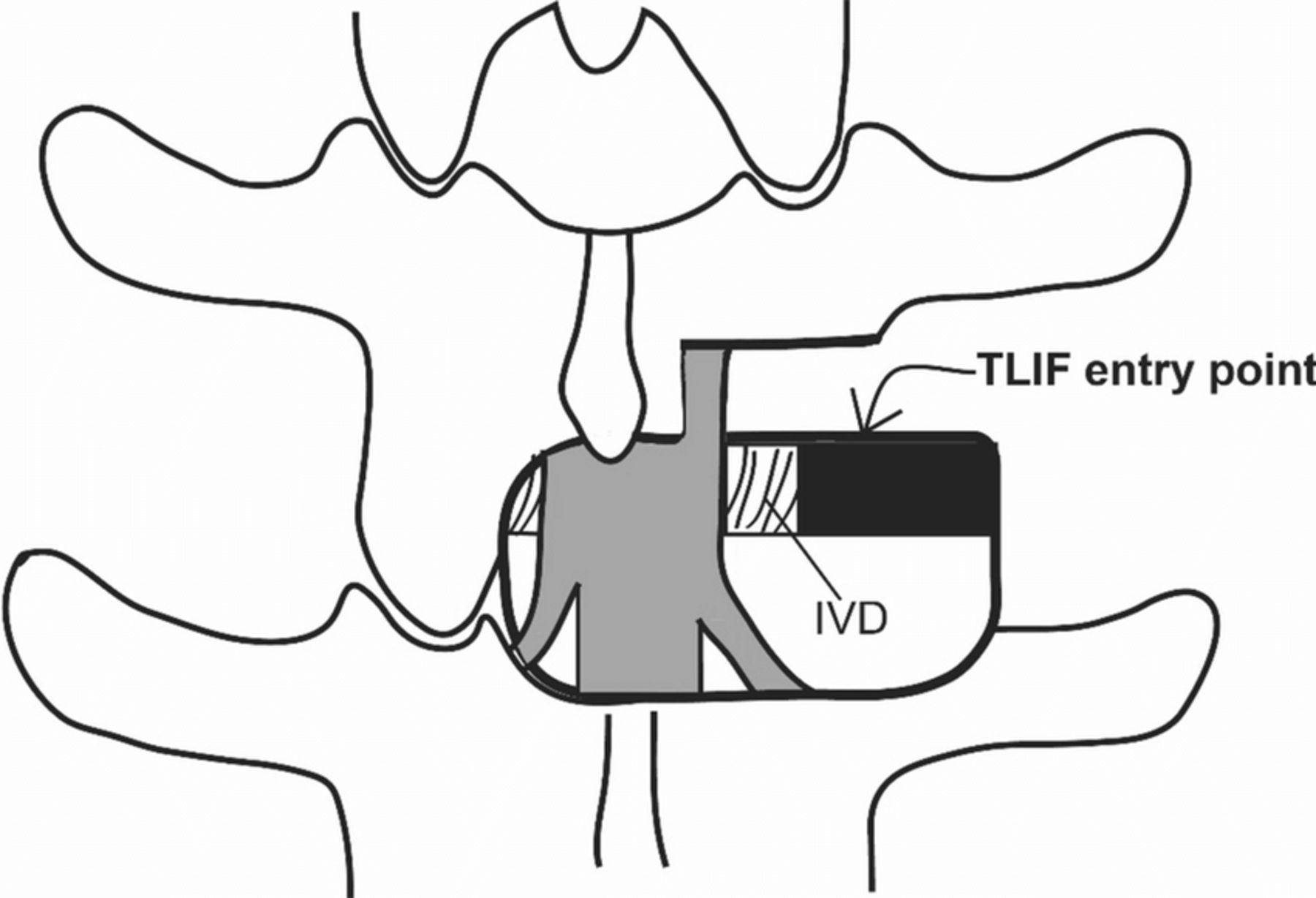
The rapid technical advancements in spine surgery were the direct result of the burgeoning development of new instrumentation as the clinical indications for spine fusion grew to include degenerative disease in addition to spinal deformity.20,21 Kambin’s triangle played a pivotal role in the evolution of fusion surgery as it provided a logical corridor to access the disc space for the placement of interbody cage devices and grafting material.2,3,7 However, the corridor was too small with an inherently limited field of view to safely and effectively deploy an adequately sized interbody device.2 Many of the initial generation devices had sharp edges and were less refined compared with contemporary devices. Recognizing these limitations, Dr. Jürgen Harms expanded the working space by including a facetectomy to safely undertake a complete discectomy and accommodate larger devices.22 With the removal of the facets, pars interarticularis, and lamina, a 3-dimensional tunnel was formed to facilitate an arthrodesis procedure now referred to as transforaminal lumbar interbody fusion (TLIF; Figure 2).23

Transforaminal lumbar interbody fusion (TLIF). Abbreviation: IVD, intervertebral disc.
The expanded, 3-dimensional working space required to perform a TLIF procedure involves consideration of a fourth anatomical boundary, the superior articular process, located posteriorly, that defines a true transforaminal corridor.2,7 This enlarged channel allows a different, more medial trajectory to the disc space compared with an endoscopic decompression procedure.3 Cutting down the angle of approach allows for an aggressive discectomy because visualization of the surrounding neural elements is improved during the removal of all cartilaginous material from the endplates and the placement of an interbody cage and bone graft as necessary in a TLIF.24
Initially, TLIFs were performed as an open procedure through a midline incision. Following the trend in the 1990s that emphasized tissue-sparing minimally invasive techniques, Foley and Lefkowitz introduced the minimally invasive TLIF technique in 2002.25 The procedure gained popularity as an effective surgical option and demonstrated comparable patient-reported outcomes to an open TLIF, with an improved safety profile that includes less trauma to the surrounding tissues, reduced postoperative pain, and faster recovery times.23 Improvements in retractor systems would allow minimal access while maintaining visualization. Concurrently, posterior lumbar interbody fusion (PLIF) offered an alternative approach by removing the medial facet and then retracting the dura and neural elements medially. However, compared with traditional posterior decompression with instrumentation and PLIF, TLIF allowed access to the disc space with less retraction on the neural elements, which reduced potential neurological injury and decreased intraoperative bleeding.26 Over time, the TLIF procedure was adopted primarily.
Pedicle and Vertebral Body Osteotomy
Based on the technique described by Harms and others, the concept of merging the procedural aspects of the TLIF procedure with the requirement to preserve anatomic motion in the form of a lumbar TJR was conceived.27,28
The TJR procedure is a lumbar motion segment reconstruction that involves device implantation using a bilateral transforaminal lumbar interbody approach to access the disc space. To expand the Kambin’s triangle working space further, laminectomy, bilateral facet removal, and complete discectomy are used to achieve a wide central and bilateral decompression of the neural elements. Additionally, sagittal balance can be restored by performing a superior pedicular osteotomy so that extension and flexion are optimized.
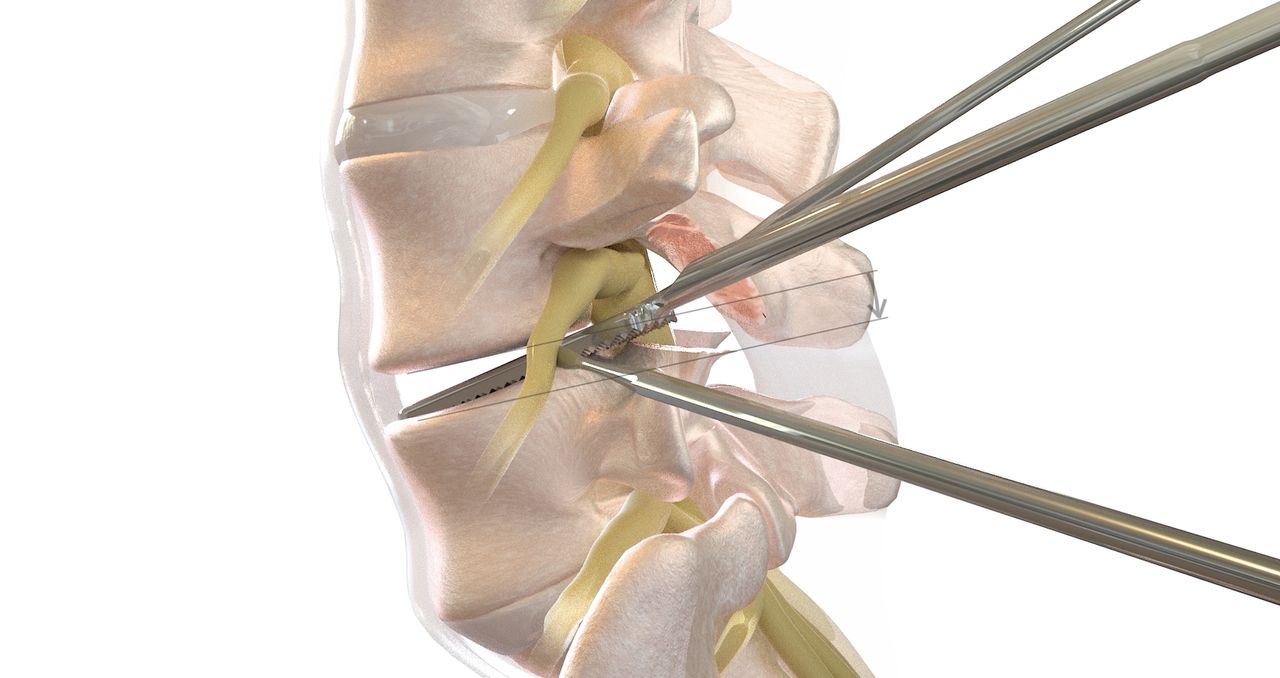
To prepare for TJR following complete discectomy, specialized oscillating rasps are used to manually prepare the vertebral endplates (Figure 3). These rasps are used to create an opening wedge osteotomy of the posterior vertebral body and superior pedicle. Modifying Harms’ TLIF approach, the pedicle is rasped down posteriorly to allow correction of sagittal alignment, neutral insertion of the TJR implant, and safer access by not disturbing the nerve superiorly or the device architecture, the dural sac, and nerve root medially. Additionally, during preoperative planning, the amount of sagittal correction needed can be planned and corrected by removing more or less of the superior pedicle to normalize the patient’s sagittal balance.

Specialized surgical rasp used for endplate preparation for total joint replacement. The shorter rasp is for the inferior endplate of the superior vertebrae. The longer rasp is for the superior endplate of the inferior vertebrae.
The apex of the wedge is in the anterior disc space to create lordosis so that the rectangular implant can be placed in a neutral position in the disc space (Figure 4). Additionally, in the coronal plane, this superior “pedicle vertebral body osteotomy” can be thought of as leveling the upper endplate of the caudal vertebral body to allow the implant to be inserted horizontally as the lateral vertebral body often sweeps up on the lateral edge of the superior vertebrae (Figure 5).

Lateral view illustrating the creation of a wedge osteotomy of the superior pedicle and contiguously into the posterior disc space.

Lateral view illustrating the pedicle vertebral body osteotomy, which entails leveling the upper endplate of the caudal level to allow the implant to be inserted horizontally.
The device’s longitudinal axis roughly parallels the pedicle into the interbody space stopping just short of the annulus to allow for motion with no impingement. Convergence occurs naturally and assists in the resistance of shear at the implant/bone interface and can be adjusted as the surgeon sees fit. The muscular compressive forces, ligamentotaxis of the surrounding soft tissue, and mechanical stresses across the motion segment combine with neutral device positioning to restore sagittal balance and normal stability (Figure 6). Rasps are used to complete a parallel surface modification for the subsequent keel cuts, allowing the device to be seated in a balanced “parallelized” position.

Distractor is in place; on the contralateral side, an oscillating rasp is being used to resect the superior S1 pedicle and posterior vertebral body to create a wedge-shaped osteotomy with the apex in the anterior disc space.
Oscillating keel cutters are used to manually create aligned superior and inferior keel cuts in the vertebral bodies that will allow for an initial coordinated press-fit of the superior and inferior keel components of the device (Figure 7).

Specialized surgical cutters are used to create keel cuts to anchor, in “press-fit” fashion, the implant. The shorter keel cutter is for the inferior endplate of the superior vertebra (no pedicle). The inferior keel cutter is for the superior endplate of the inferior vertebrae (including pedicle).
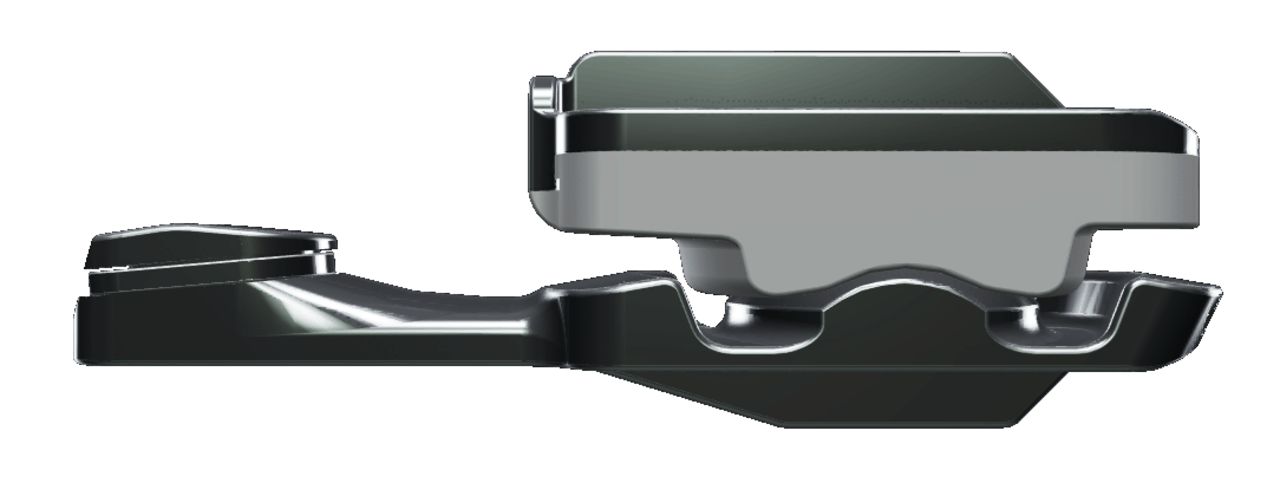
The TJR implant (MOTUS, 3Spine, Chattanooga, TN, USA) replaces the function of the disc and facet joints through a posterior approach. The dual bearings resist shear much like the 2 native facet joints while carrying compressive axial loads such as the disc (Figure 8).29 The technology utilizes highly cross-linked antioxidant vitamin E polyethylene, compression molded into a cobalt chrome and titanium plasma-sprayed substrate.30

The MOTUS device.
The treated segment receives 2 implants, inserted bilaterally along the trajectory of the pedicles, such that the midpoint of the ball of the implant is approximately 40% ventral to the posterior vertebral body, which is consistent with the physiological center of rotation (Figure 9).

Final implant placement showing the rectangular implant resting on posterior superior L5 with the L4 to L5 segment in lordosis. The wedge-shaped pedicle vertebral body osteotomy of L5 allows the rectangular implant to rest in the disc space while maintaining segmental lordosis.
Initial fixation is achieved by press-fit via a titanium plasma spray ingrowth surface at the keel/bone interface, as well as the placement of a retention screw into the caudal portion of the implant, which passes obliquely through the pedicle and into the vertebral body of the caudal level (Figure 9).
Discussion
The identification and subsequent surgical modifications of Kambin’s triangle have supported an increasing array of more complex procedures.19 The progression from posterolateral intradiscal access in the intact lumbar spine to an enlarged working space following facetectomy, to accommodate a TLIF as developed by Harms to further expansion via PVBO, to support motion preservation with TJR represents a unique evolutionary pathway in surgical technique development. The initial approaches were introduced in the 1960s and 1970s. At that time, anatomic landmarks, rudimentary radiographs, and fluoroscopy were utilized to identify a safe corridor for injections, trocars, and endoscopic instruments. As technology improved and interbody fusions became a more common solution for a wider array of surgical pathologies, more direct visualization was necessary because of the size of the implants and the safety of adjacent neural structures.
PLIF procedures were being developed and utilized prior to the introduction of the TLIF approach. These procedures utilized the more standard midline approach of the day but required more retraction on the dural elements, potentially causing injury. Bleeding was also more excessive than TLIF as retraction of epidural bleeding was harder to control.26 The transforaminal approach involved removing the facet from a lateral position or extraforaminally. This process initially required a more oblique angle for cage placement as more of the lateral facet was removed. Larger cages could be placed with improved direct line of sight. Additionally, the surgeon could identify the exiting nerve root and decide how much retraction of the dura was safe. With improved image guidance, interbody cage designs were modified to make them safer and more sophisticated, leading to the utilization of a variety of lordotic and expandable cages.
Over the past 5 decades, there has been enormous progress in developing joint replacement implants for the large synovial joints of the appendicular skeleton that replicate physiological motion. These kinematic improvements have been accompanied by materials with enhanced wear characteristics. Surgical techniques for placement that are safer and require smaller incisions minimize pain and discomfort after surgery and accelerate the return to normal activities and work. After Sir John Charnley performed the first modern low friction hip arthroplasty in November of 1962,31 it successfully became the gold standard because it replicated normal motion of the hip joint.32 Since that time, there has been continued exploration into new material and implant designs to return the joint to near-normal motion.33 As arthroplasty devices evolved and improved, there has been a corresponding expansion of the indications for surgery as the long-term safety and efficacy of the procedure have been established.34,35 For example, hip replacements were initially recommended only for patients older than 65 years because it was thought that the decreased activities of older patients would prolong the life of the prosthesis. With improvement in technique and materials, more than 50% of patients undergoing hip replacements are now younger than 65.36 Based on the recognized success and durability of this motion restoration procedure, hip arthroplasty has been referred to as the “operation of the century.”37
In the lumbar spine, the initial attempts at motion preservation were focused on replacing only the degenerated intervertebral disc, which is a cartilaginous amphiarthrotic joint.38,39 However, each vertebral motion segment consists of a 3-joint complex, which includes the 2 posterior synovial facet joints in addition to the intervertebral disc. Recently, motion preservation technology has been extended further to include lumbar facet arthroplasty given the appreciation that degeneration affects the entire 3-joint complex.40–42 TJR couples the advantages of disc and facet arthroplasty by replacing the entire 3-joint complex with a single implant system.27
The development of TJR has benefited from advances in materials science such as vitamin E–stabilized, highly crosslinked polyethylene, which provides a thinner and more reliable polymer to extend the wear of the motion surface.30 Similar improvements in bioactive titanium surfaces also provide more consistent ingrowth into the implant/bone interface.
It is interesting to note that the evolution of Kambin’s triangle as a working corridor for spinal procedures has spanned nearly 6 decades, mirroring trends in surgery and instrumentation development. With the inevitable adaptation of machine learning methods in spine surgery,43 personalized image-guided, artificial intelligence–enhanced, robotically assisted TJR is poised to reshape spine care, enhancing precision, personalizing treatment pathways, ensuring safety, and accelerating adoption. TJR is well-positioned to benefit from these advancements, ultimately improving patient outcomes, quality of life, and worldwide accessibility. It will be important to gauge and harness the acceleration of the progress in spine care particularly with respect to the convergence of advanced real-time intraoperative imaging, robotics, and artificial intelligence in the clinical acceptance of TJR of the lumbar spine.19
Footnotes
Funding J.E.B. received funding to assist in the preparation of this manuscript from 3Spine (Chattanooga, TN, USA). This research received no additional external funding.
Disclosures S.C.H., J.E.B., and S.D.H. have stock in 3Spine. Additionally, S.D.H. is an employee of 3Spine. The authors declare that they have no other known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Disclosures S.C.H., J.E.B., and S.D.H. have stock in 3Spine. Additionally, S.D.H. is an employee of 3Spine. The authors declare that they have no other known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}