


Abstract
Background The L2 nerve root is considered part of the lumbar plexus that innervates the iliopsoas (IP) and quadricep muscles (Qd). Total en bloc spondylectomy (TES) at the L2 vertebra requires bilateral nerve root transection to facilitate surgical dissection and vertebral body removal. Information regarding neurological function recovery of the IP and Qd in patients with muscle weakness before TES is lacking. We aimed to report the neurological recovery of IP and Qd after TES involving the L2 vertebra in preoperative lower extremity weakness in spinal tumor patients.
Methods We prospectively recorded all L2-involved spinal tumor patients undergoing TES between January 2018 and November 2020. As a primary outcome, we recorded the Manual Muscle Testing (MMT) grade of the IP and Qd preoperatively, immediately postoperatively, and at follow-up. Secondary outcomes included the Frankel neurological status, sensation impairment, and the Eastern Cooperative Oncology Group score.
Results From 8 TES-involving L2 patients, 6 (4 males) met the inclusion criteria. One patient had first-grade deterioration of the Qd MMT immediately postoperatively. All patients could ambulate independently 6 months after surgery. Five patients required follow-up for more than 1 year and could walk without any gait aids. All patients had persistent anterior groin and bilateral thigh numbness until the final follow-up.
Conclusion Neurological recovery of the IP and Qd muscles as measured by MMT can occur within 6 months of bilateral L2 nerve root transection. Bilateral L2 nerve root sacrifice can have acceptable neurological outcomes and recovery, even in patients with preoperative IP and Qd weakness.
Level of Evidence 4.
INTRODUCTION
Total en bloc spondylectomy (TES) is considered one of the surgical options for primary spinal tumors and some patients with spinal metastasis.1–6 As an aid to surgical dissection, bilateral nerve root ligation is performed at the thoracic spinal level. It is known that at the lumbar spinal level, L3 to L5 nerve root transection will result in residual deterioration of motor function of the quadriceps (Qd) and tibialis anterior, which will impair the ability to perform basic activities of daily living (ADL).7–9 What is lacking, however, is information on motor function after transection of the L1 and L2 nerve roots.
The L2 nerve root is included in the lumbar plexus and innervates the iliopsoas (IP) and Qd muscles.10,11 A study by Kato et al showed initial deterioration of IP and Qd muscle strength after bilateral transection of the L2 nerve roots, which gradually recovered.12 Kato et al, however, included only patients who had preoperative motor function of the Qd and IP of at least grade 4 (by Manual Muscle Testing [MMT]) and at least D3 (according to the Frankel neurological grade). The aim of the current study was to evaluate the neurological recovery of Qd and IP muscle function (Frankel grade A, B, and C) after performing bilateral L2 nerve root resection TES.
MATERIALS AND METHODS
After securing ethics approval from our institution (registration HE611450), we prospectively recorded 38 patients who underwent TES between January 2018 and November 2020. The inclusion criteria were as follows: (a) spinal tumor involving L2 vertebra, (b) bilateral L2 ligation and transection, (c) minimum follow-up time of 6 months, and (d) preoperative Frankel neurological grade of A, B, or C. The exclusion criteria were (a) no follow-up for at least 6 months and (b) preoperative Frankel neurological grade of D or E.
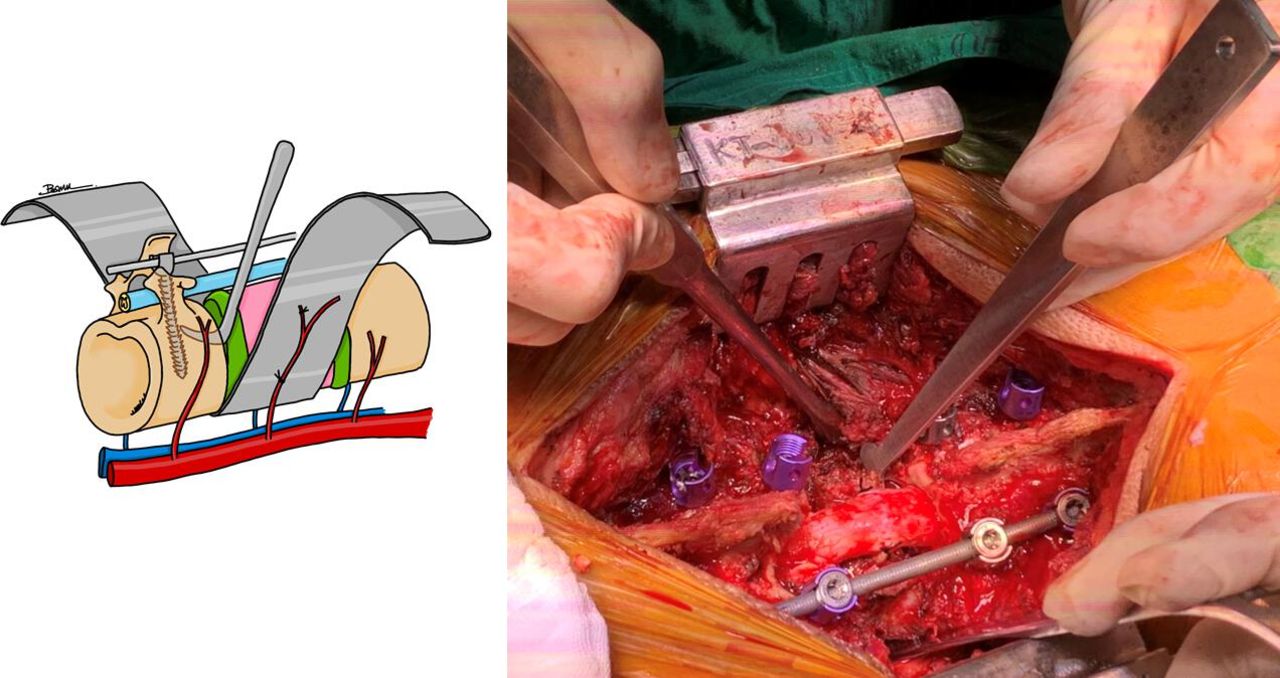
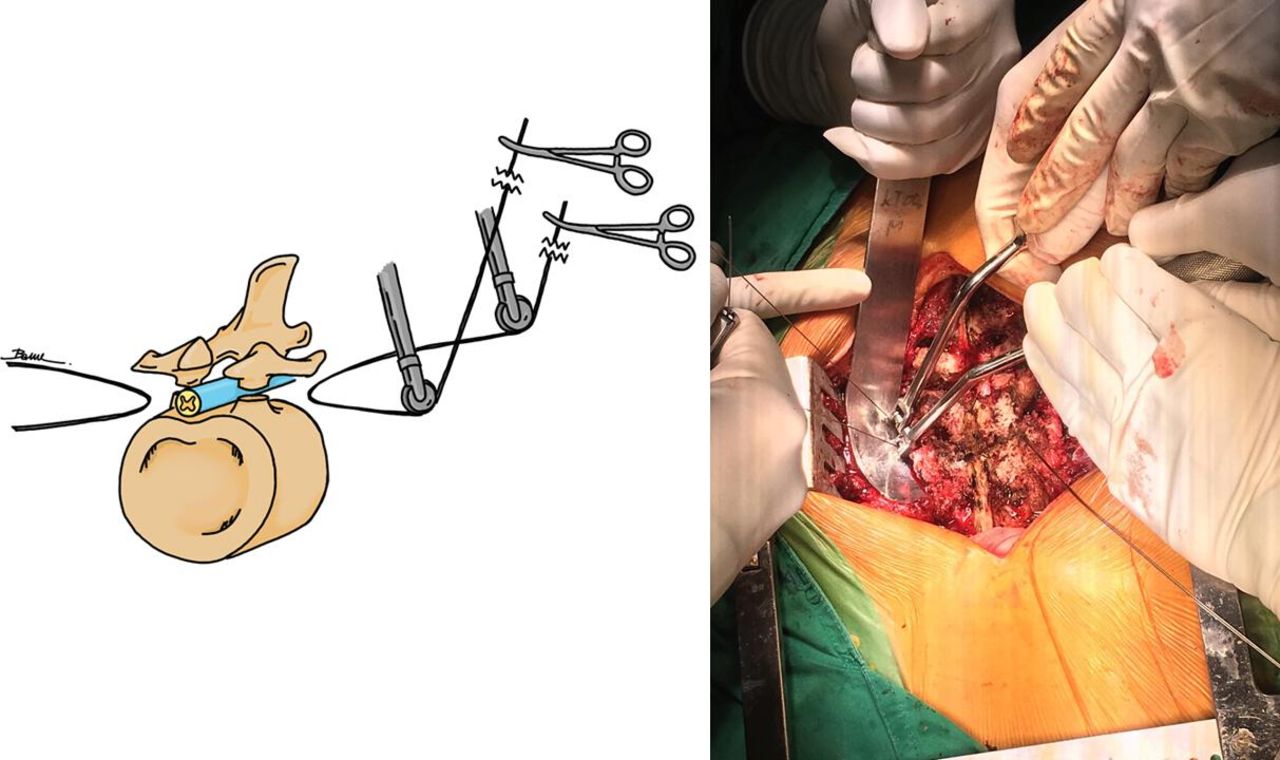
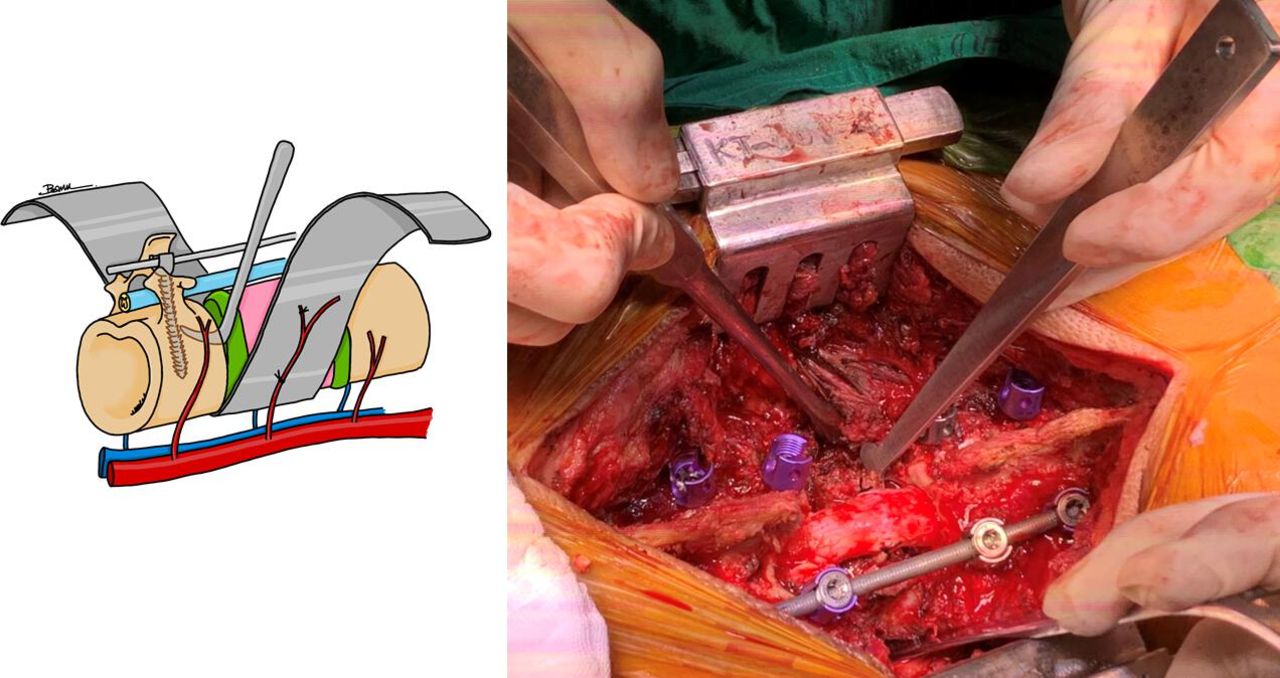
All TES cases were performed by the same operator (P.P.). All patients underwent an anterior-posterior approach. The anterior retroperitoneal approach on the left side was used to identify and cut the diaphragmatic crus, which were inserted at the L2 vertebral body (Figure 1). En bloc laminectomy was then performed with a posterior approach using T-saw pediculectomy (Figure 2). The bilateral L2 nerve roots were ligated and cut at the level proximal to the dorsal root ganglion. The en bloc vertebrectomy was done using a posterior approach by cutting the adjacent intervertebral disc with an L-shape osteotome (Figure 3) and then rotating the vertebral body outward carefully to avoid any thecal sac injury. A titanium mesh cage was used for anterior column reconstruction, and spinal shortening was performed to tighten the cage and increase spinal blood flow.
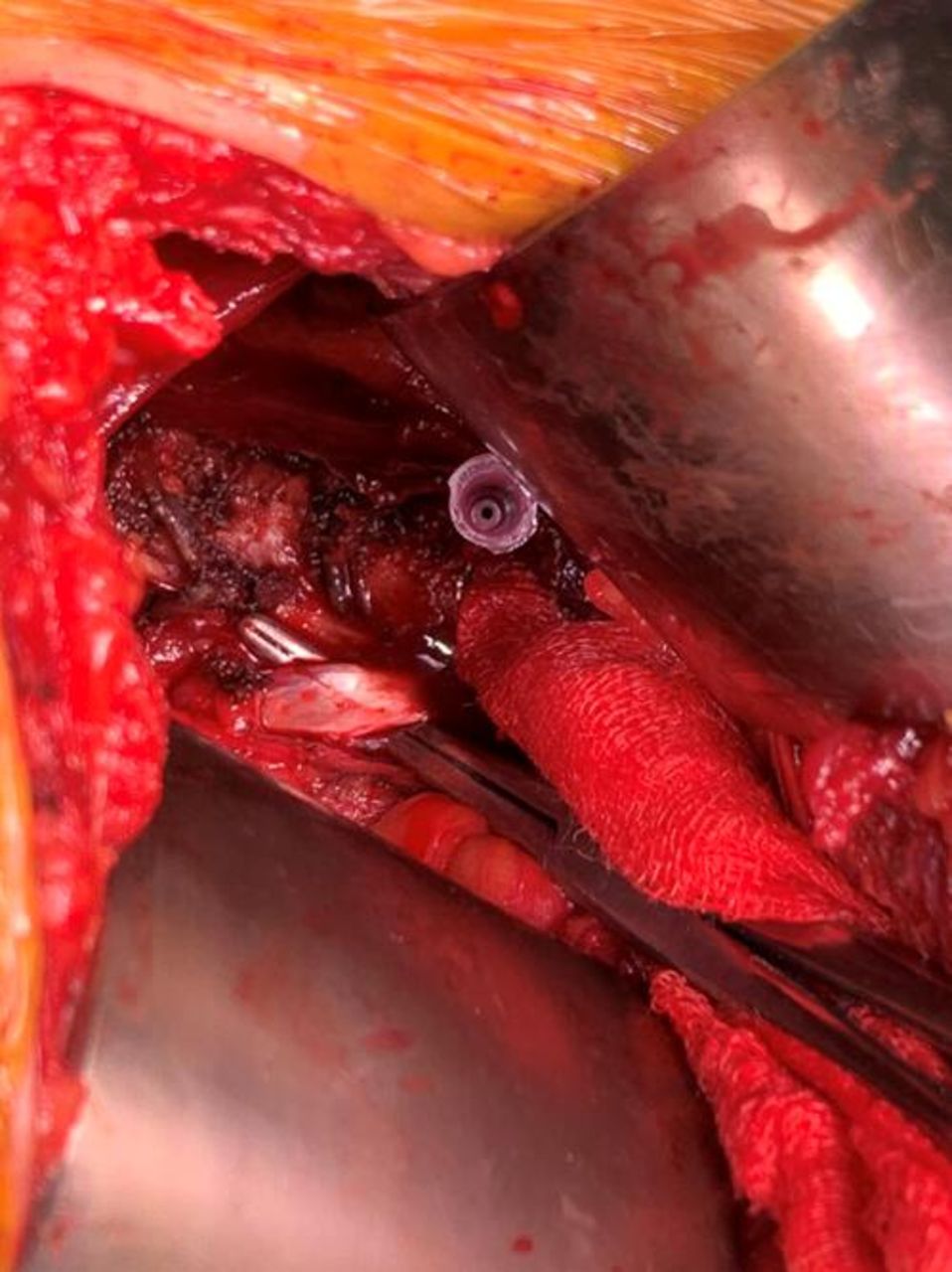
The diaphragmatic crus from left side anterior retroperitoneal approach.

En bloc laminectomy performed with a posterior approach using T-saw pediculectomy.
L-shaped osteotome used to perform spondylectomy through posterior approach.
The primary outcome was neurologic recovery of the IP and Qd vis-à-vis motor function according to MMT grading. The secondary outcomes were Frankel neurological status, sensation impairment, the Eastern Cooperative Oncology Group (ECOG) score, and the Oswestry Disability Index (ODI)13,14 at the last follow-up. In terms of follow-up, a clinical evaluation was done, and a plain radiograph taken monthly until month 3. Then a clinical assessment was done, and a plain radiograph and computed tomographic (CT) image were taken of the spine every 3 months until 1 year. Finally, the clinical examination and x-ray imaging were done every 6 months until year 2. Magnetic resonance imaging (MRI) was indicated when local recurrence of the tumor was suspected by CT. In terms of neurological status and MMT testing evaluation, all patients were assessed by the operating author (P.P.).
RESULTS
Of the 38 TES cases at our institution, 8 underwent TES at the L2 level. After screening according to the inclusion and exclusion criteria, only 6 patients (4 men) remained in the study. The demographic data, presenting symptoms, and duration of symptoms for these patients are presented in Table 1.
Patients’ demographics and presenting symptoms.
Immediately postoperatively, 1 patient (case no. 3) had a temporary single grade bilateral reduction in the MMT of the Qd (Table 2). All patients had bilateral anterior thigh and groin paresthesia and 1 patient (case no. 4) had transient tingling in the anterior groin. All patients at the last follow-up showed recovery of the IP and Qd MMT to at least grade 4. The ECOG score was improved in all patients. Regarding ADL, all patients could perform self-care and dependent ambulation at home by the last follow-up (Table 2). Most of the patients could perform self-ambulation with gait aids, such as a walker frame, within 5 months postoperatively. Regarding ODI, the disability status was mild (score ranges from 10% to 28%) in 5 patients and moderate in 1 patient (score ranges from 30% to 48%) at the last follow-up period. All patients had persistent bilateral numbness of the anterior thigh, but this did not disturb their ADL. Five of the 6 patients were still attending follow-up more than 12 months postoperatively. One patient died (case no.1) from the disease (cholangiocarcinoma) at 7 months postoperatively. Before his death, he could perform ADL with minimal help and was satisfied with the result of his spinal surgery.
The Eastern Cooperative Oncology Group (ECOG), Frankel grading, Oswestry Disability Index (ODI) at the last follow-up, and Manual Muscle Testing (MMT) of the iliopsoas (IP) and quadriceps (Qd) at preoperative and postoperative follow-up until last follow-up.
Regarding complications, none of the patients suffered from surgery-related complications.
CASE PRESENTATION
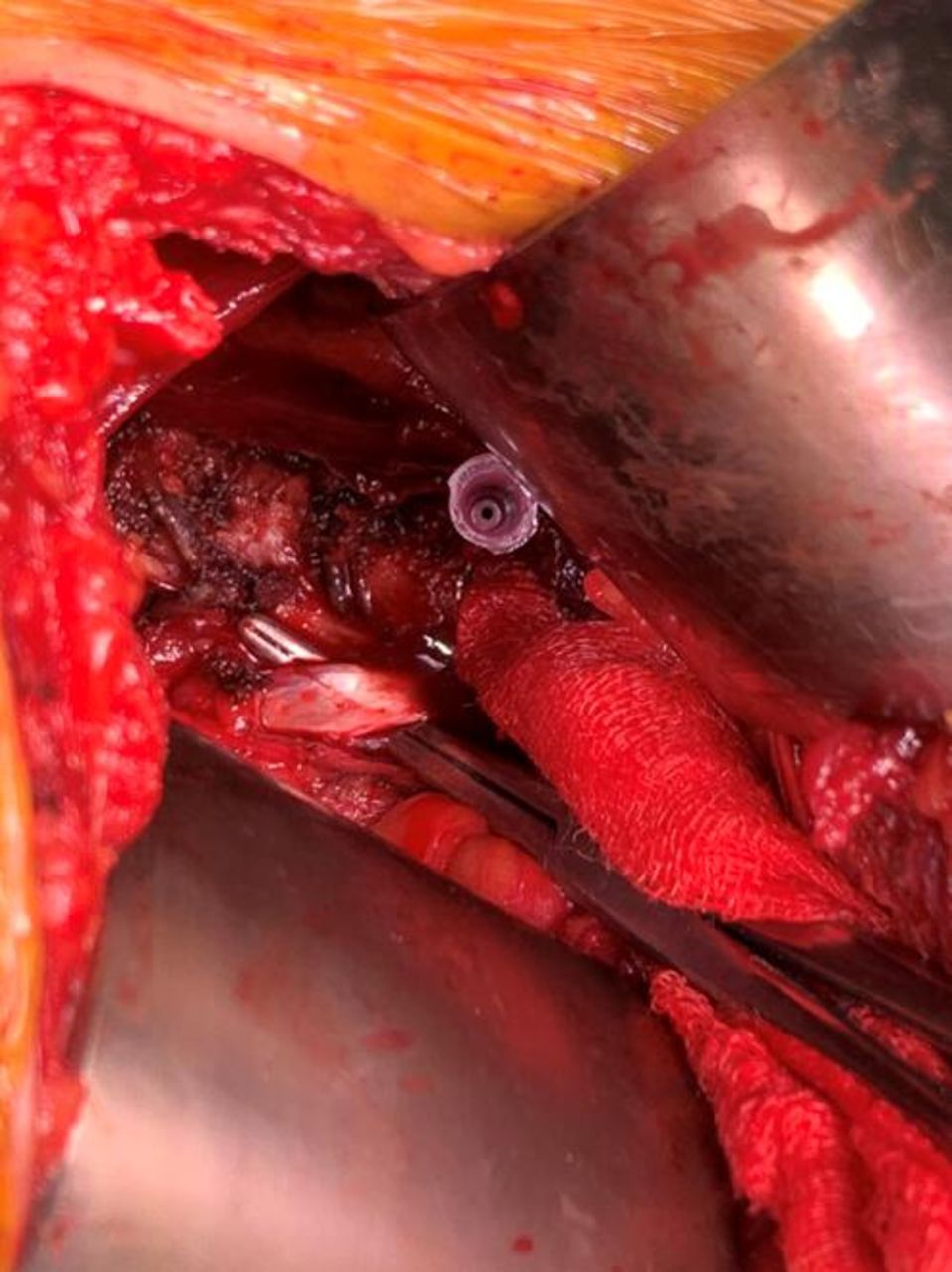
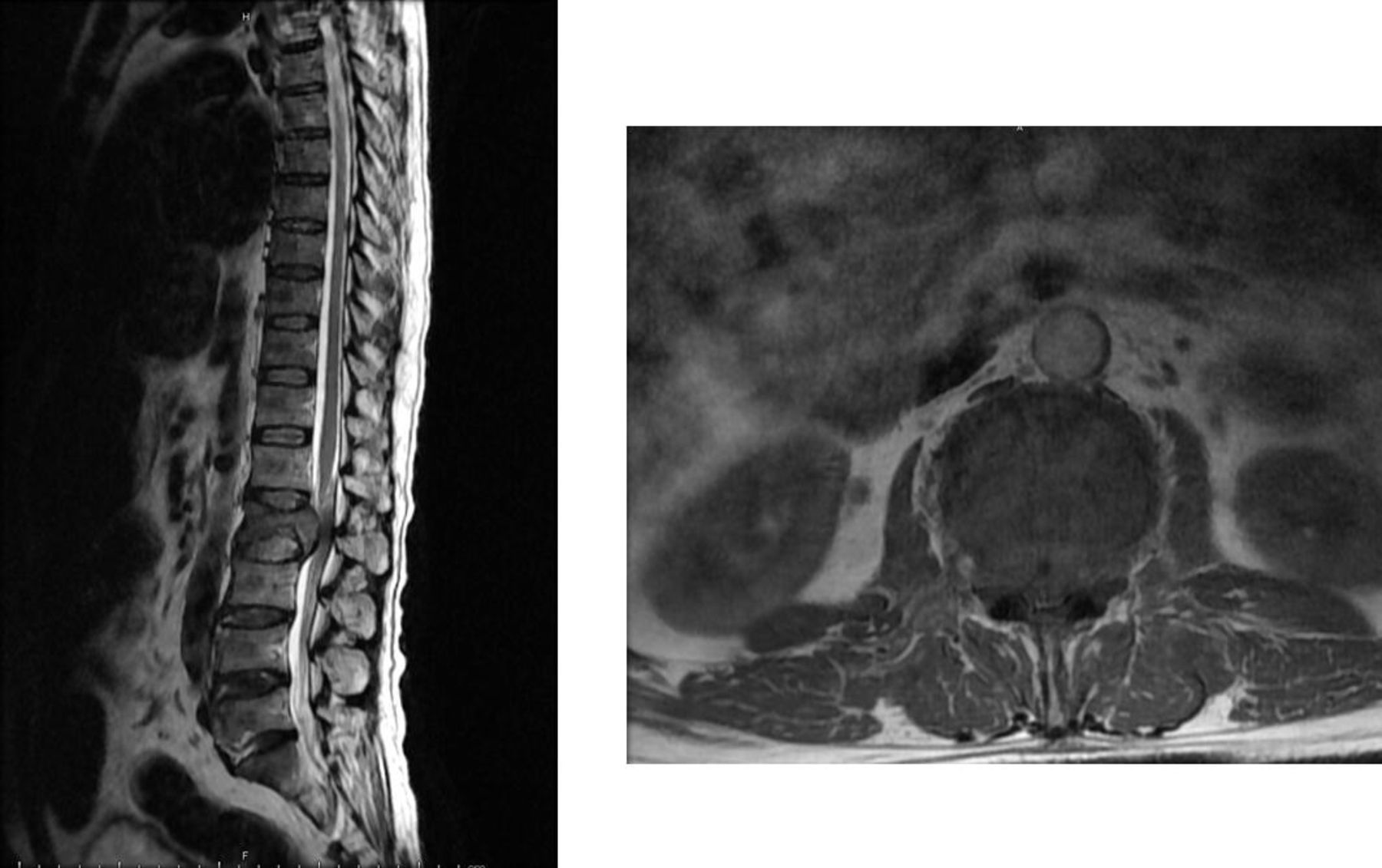
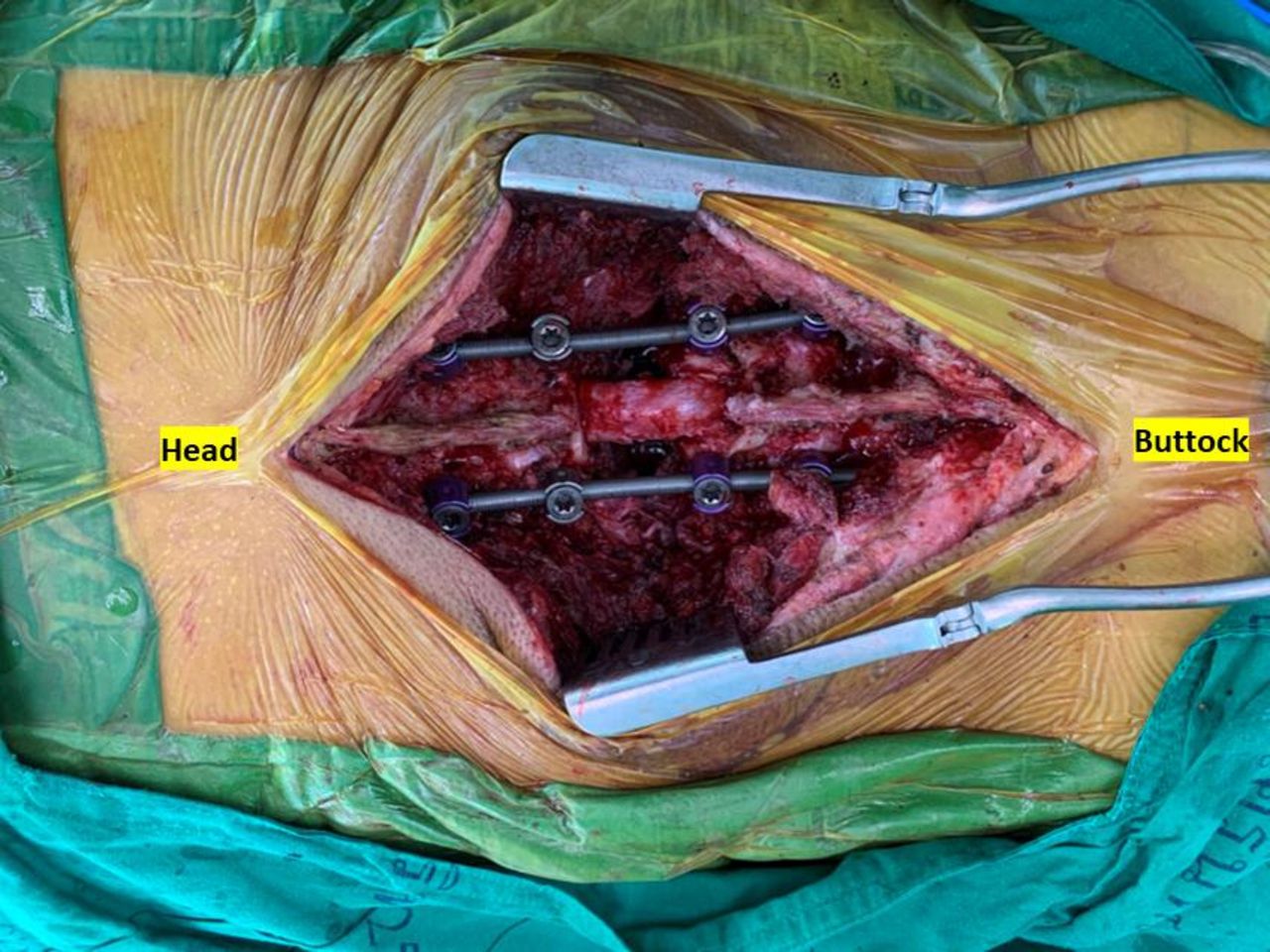
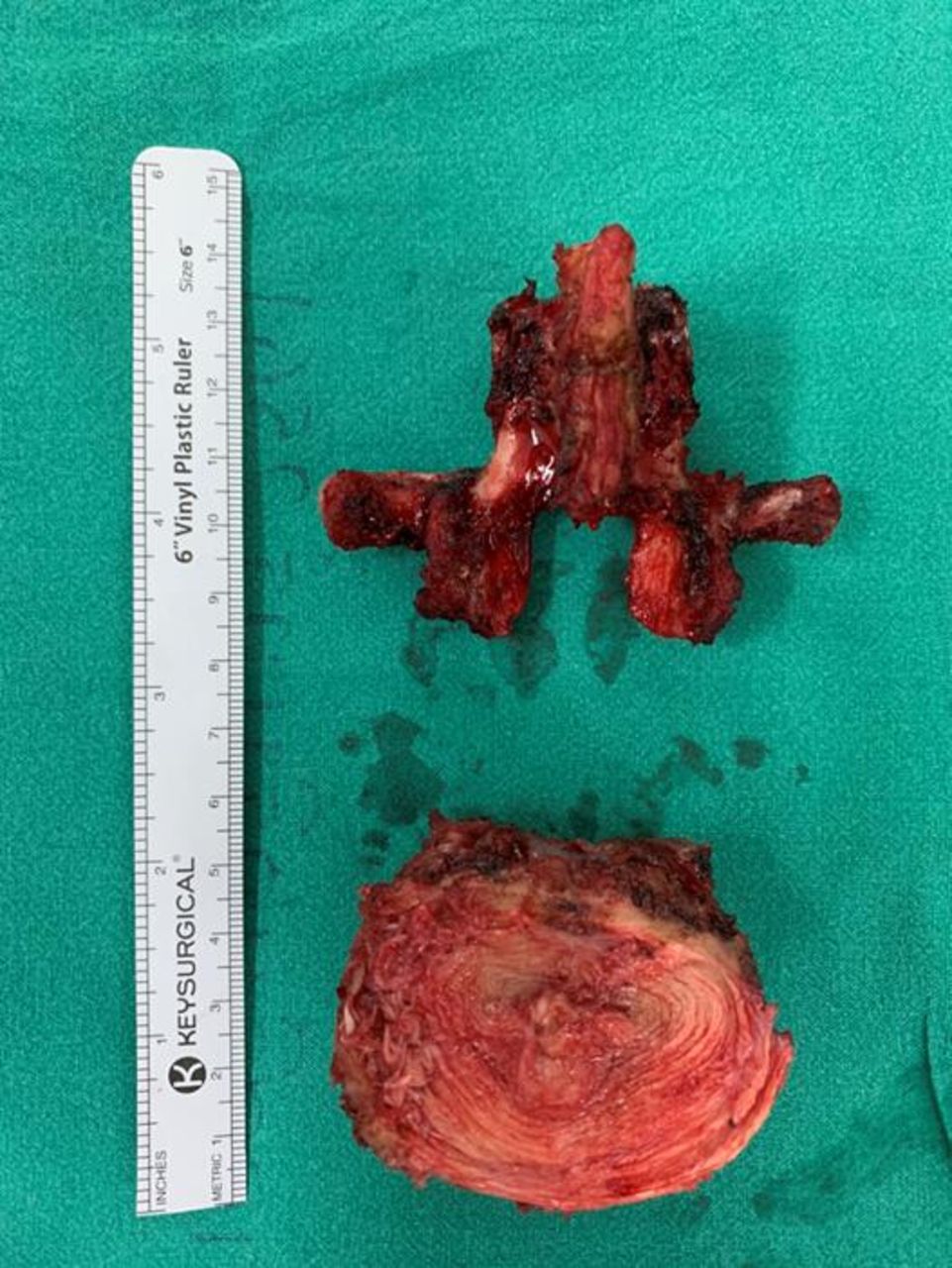
A 56-year-old man presented with L2 metastasis from adenocarcinoma of the lung. The MRI showed L2 destruction with soft tissue extension compressing the spinal canal, leading to bilateral weakness of the lower extremities’ muscle MMT (Figure 4). TES of L2 was performed using a combined anterior-posterior approach with L2 nerve root transection (Figure 5). The TES specimen is shown in Figure 6. At the last follow-up, the patient could walk independently and showed neurological recovery to Frankel E and an ECOG score of 1.
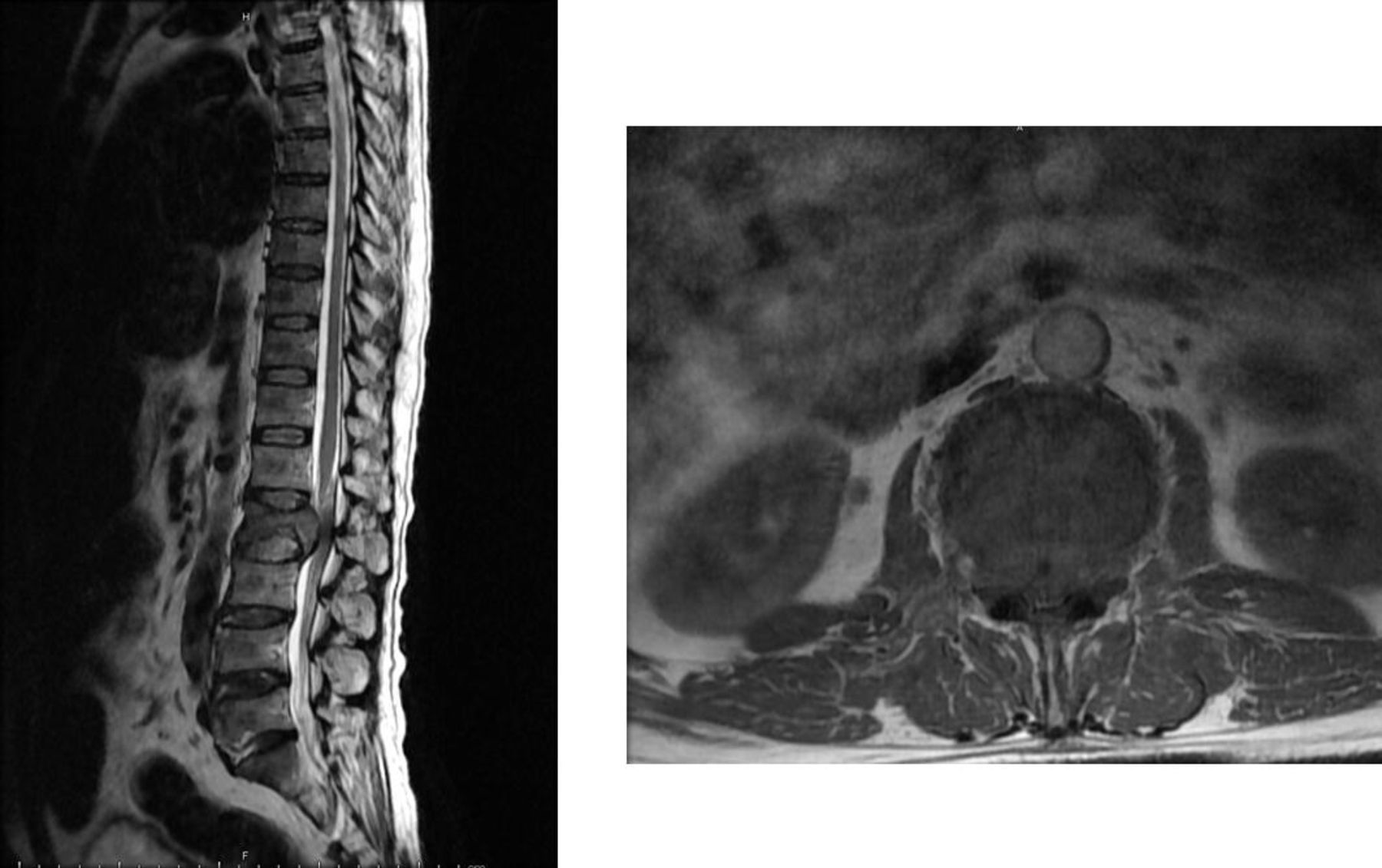
MRI demonstrated single L2 level spinal metastasis with severe spinal canal compression.

L2 Total en bloc spondylectomy (TES) was performed with bilateral L2 nerve root sacrificed.

L2 TES specimen (TES, total en bloc spondylectomy).
DISCUSSION
TES is a surgical procedure that achieves total removal of a spinal column-containing tumor.10,11,15–17 To facilitate complete removal of the tumor and the vertebral column, bilateral nerve root transection at the affected vertebra is recommended. At the thoracic level, bilateral nerve root ligation causes dermatomal numbness and weakness of the paravertebral muscle, which does not much alter ADL.4,6,18,19 However, at the lumbar level, especially at L3 to L5, the nerve root sacrificed can cause significant deterioration in ambulation and dependence on other people for normal ADL.1,7,8,20 The L2 nerve root forms part of the lumbar plexus, which contributes to innervation of the IP and Qd muscles.10,11Sacrificing the bilateral L2 nerve root in spinal surgery raises the possibility of post-operative neurological deterioration of the IP and Qd muscles.
Kato et al12 reported a period of temporary MMT deterioration of the IP and Qd postoperatively after sacrificing the bilateral L2 nerve root during TES (ie, MMT grading at least 4, and Frankel D2 to E). All 13 patients in the study by Kato et al returned to preoperative MMT of the IP and Qd with no impairment in ADL at their last followup. In our study, an improvement in MMT grading of the IP and Qd was demonstrated over time when the preoperative IP and Qd MMT grading was less than grade 3. All the patients in our study showed almost completely independent ambulation (ECOG of 1 and 2) and no impairment in ADL at their last follow-up (Frankel D3C to E) (Table 2). Our results confirm that the L2 nerve root plays some part in the innervation of Qd and IP along with L3 and L4. Even with sacrifice of the bilateral L2 nerve root, the MMT of the IP and Qd recovered after surgery, albeit over time. All patients in our study experienced persistent bilateral numbness at the anterior thigh, but this did not significantly disturb ADL. Evidence suggests L2 nerve root transection during L2-involving TES can have satisfactory outcomes.
The limitations of our study were (a) the small number of patients and (b) the relatively short period of postoperative follow-up. Our study had several strengths: (a) only L1 and L2 transection cases were included, and (b) despite the short period of follow-up, the study demonstrated recovery of MMT of the IP and Qd.
CONCLUSION
The findings of this study suggest that L2-sacrificing TES can be safely performed, and acceptable neurological results can be expected in terms of MMT recovery of the IP and Qd vis-à-vis preoperative Frankel A to C. Considering the small number of patients, further study with a larger number of patients and longer follow-up is needed to confirm these findings.
Acknowledgments
We thank the patients, the Department of Orthopedics and the Faculty of Medicine for their support, and Mr. Bryan Roderick Hamman under the aegis of the KKU Publication Clinic for assistance with the English language presentation of the manuscript.
Footnotes
Funding This study received support grants from the Faculty of Medicine, Khon Kaen University (IN64135) and Research and Graduate Studies, Khon Kaen University, Thailand.
Declaration of Conflicting Interests The authors report no conflicts of interest with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.