


ABSTRACT
Background: The purpose of this study was to perform a systematic literature review and meta-analysis to evaluate the sensitivity, specificity, and accuracy of dual-energy computed tomography (DE-CT) of bone marrow edema and disc edema in spine injuries.
In vertebral injuries, prompt diagnosis is essential to avoid any delays in treatment. Conventional radiography may only reveal indirect signs of fractures, such as when it is displaced. Therefore, to detect the presence of bone marrow or disc edemas, adjunctive tools are required, such as magnetic resonance imaging (MRI) or DE-CT.
Methods: Search terms included ((DECT) OR (DE-CT) OR (dual-energy CT) OR “Dual energy CT” OR (dual-energy computed tomography) OR (dual energy computed tomography)) AND ((spine) OR (vertebral)), and the PubMed, EMBASE, and MEDLINE databases and the Cochrane Library and Google were used. We found 1233 articles on our preliminary search, but only 13 articles met all criteria. Data were extracted to calculate the pooled sensitivity, specificity, and diagnostic odds ratio for analysis using R software.
Results: Within the 13 studies, 515 patients, 3335 vertebrae, and 926 acute fractures (27.8%) defined by MRI were included. The largest cohort included 76 patients with 774 vertebrae. In 12 publications, MRI was reported for comparison. For DE-CT, the overall sensitivity was 86.2% with a specificity of 91.2% and accuracy of 89.3%. Furthermore, 5 studies reported the accuracy of CT with an overall sensitivity of 81.3%, specificity of 80.7%, and accuracy with 80.9%. Significant differences were found for specificity (P < .001) and accuracy (P = .023). However, significant interobserver differences were reported.
Conclusions: DE-CT seems to be a promising diagnostic tool to detect bone marrow and disc edemas, which can potentially replace the current gold standard, the MRI.
Level of Evidence: 2.
Clinical Relevance: This study shows that DE-CT seems to be a promising diagnostic tool with an accuracy of 89.3%.
INTRODUCTION
Vertebral fractures can be life-threatening and cause disabilities if not diagnosed in a timely manner. Therefore, prompt diagnosis is necessary to avoid any delays in treatment. The gold standard includes conventional radiography and computed tomography (CT) where most fractures can be diagnosed. Hereby, conventional radiography may only reveal indirect signs of fractures, such as when it is displaced. Obtaining multiple views, including standing, sitting, and supine views, improves the ability to detect fractures. In the acute trauma setting, CT is typically limited to the supine position, raising concerns that injuries may be underdiagnosed or even missed. However, these tools do not allow for the assessment of the presence of bone marrow edema or disc edema, which are uncommon after fracture consolidation. As such, further studies are often required to exclude nondisplaced fractures with concomitant soft tissue injuries. Typically, the gold standard for the detection of vertebral injuries and relevant soft tissue injury is magnetic resonance imaging (MRI).1 In an acutely injured spine, MRI is better able to detect diagnoses, such as bone marrow edema or acute spinal stenosis. However, use of MRI is limited by its time-intensive nature and high costs, and patients need to be free of any implanted metal devices, such as pacemakers or brain stimulators.2–4
Dual-energy computed tomography (DE-CT) was first described by Brooks in 1977, which has gained popularity in recent years.5,6 It measures the electron density and effective atomic number, which can be converted to Hounsfield numbers by normalizing them to water.7,8 This new tool enables visualization of bone marrow abnormalities directly, which may help detect traumatic or osteoporotic fractures.9 A variety of different indications have been described, including the spine, hip, knee, and ankle with implants as well as metabolic diseases, such as gout or neoplasm.10 Several studies have shown that DE-CT can be useful in the management of metabolic disease.11
The purpose of this study is to perform a systematic literature review and meta-analysis to evaluate the sensitivity, specificity, and accuracy of DE-CT of bone marrow edema and disc edema in spine injuries.
METHODS
Systematic Review
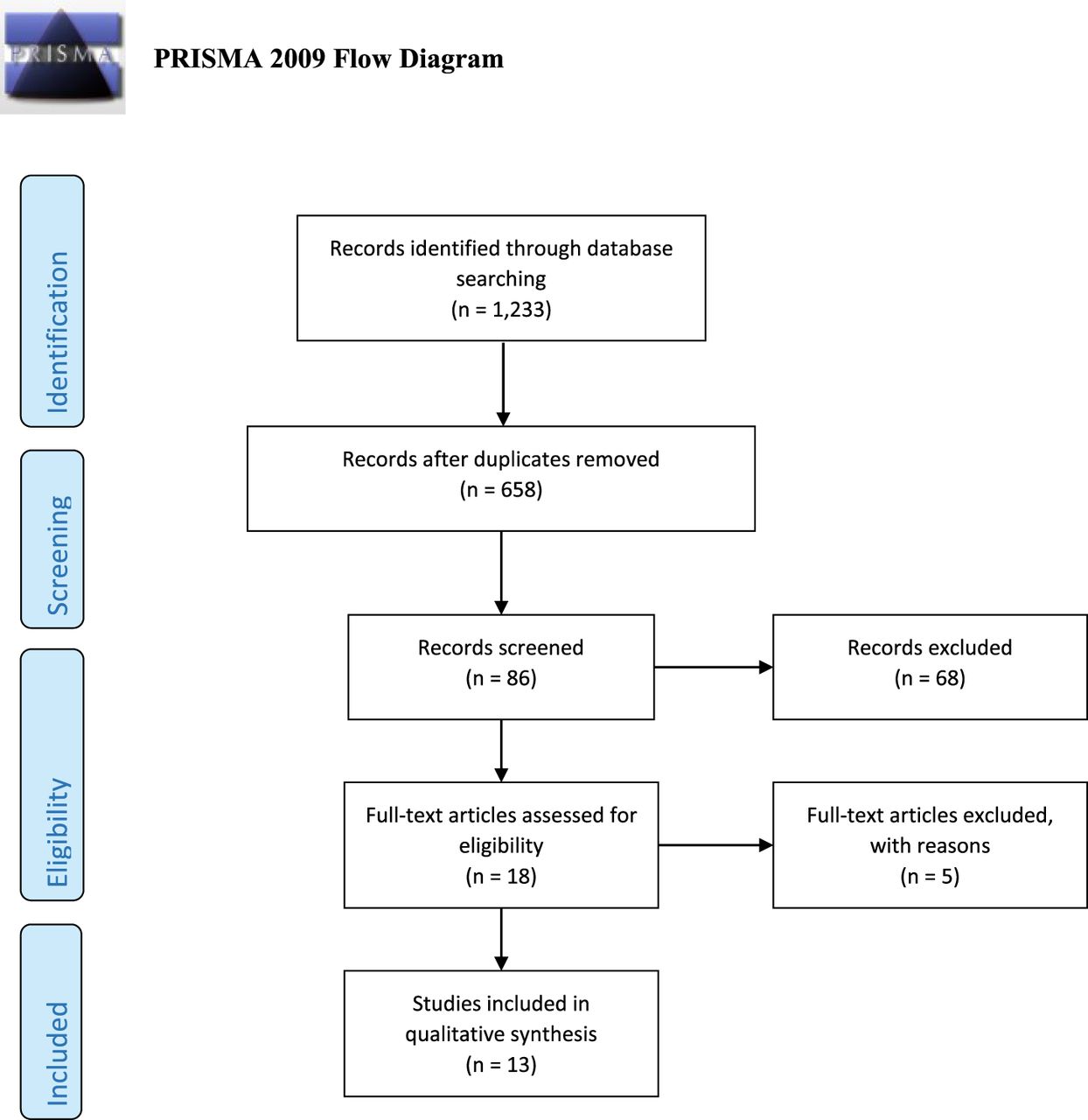
On December 1, 2019, a systematic review using the PRISMA guidelines was performed.12 The PubMed, EMBASE, and MEDLINE databases and the Cochrane Library and Google were used, and search terms included ((DECT) OR (DE-CT) OR (dual-energy CT) OR “Dual energy CT” OR (dual-energy computed tomography) OR (dual energy computed tomography)) AND ((spine) OR (vertebral)). All articles in French, German, and English investigating the sensitivity, specificity, and accuracy of DE-CT in spine injuries were included. Any duplicate results, lack of full access to the original article, review articles, and editorial articles were excluded. In total, 1233 articles were found on our preliminary search, but only 13 articles met all criteria. These 13 articles are included in our systematic review and meta-analysis (Figure 1).

Included articles according to the PRISMA guidelines.
Statistical Evaluation
For the meta-analysis, we extracted data on the authorship, year of publication, study design (prospective or retrospective), and demographic characteristics of the participants, such as age, sample size, number of scanned vertebrae, CT, and MRI scanner. Furthermore, the true positive, false positive, true negative, and false negative results were collected and used for the meta-analysis.
The data obtained were used to calculate the pooled sensitivity and specificity as well as positive predictive value (PPV), negative predictive value (NPV), positive and negative likelihood ratios, and the diagnostic odds ratio. All sensitivities, specificities and diagnostic odds ratios were illustrated in forest plots from individual studies. To pool the sensitivity and specificity, a bivariate random effect model was applied.13–15 Further, the random effects model the method-of-moments (DerSimonian-Laird) was used to calculate the τ2 as well as the I2 test to assess heterogeneity. Hereby, I2 was defined as no presence of heterogeneity between 0% and 40%, moderate heterogeneity between 30% and 60%, substantial heterogeneity between 50% and 90%, and considerable heterogeneity between 70% and 100%.16 To analyze the correlation between the sensitivity and false positive rate, the Spearman's correlation coefficient was calculated, whereby a coefficient of >.6 was thought to be considerable.
For statistical analysis, R software version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria) was used, applying the mada package. All continuous variables are presented as means and a 95% confidence interval. Categorical variables were stated as percentages, and statistical significance was set to P < .05.
In all studies, MRI was used as a standard of reference. The accuracy per vertebra was investigated when compared with DE-CT. Furthermore, Karaca et al as well as Bierry et al distinguished not only between the imaging modalities but also between the height of vertebral injury for both thoracic and lumbar segments. Diekhoff et al compared the DE-CT findings with and without prior spine surgery. Foti et al defined a per vertebra-based 50-HU cutoff.17–20 In a further study, different material decomposition, including adaptive iterative dose reduction with different iterations (mild, standard, and strong), were investigated.21 Seven of 13 articles included report the accuracy of conventional CT.
RESULTS
In total, 515 patients, 3335 vertebrae, and 926 fractures (27.8%) were included. Three studies were retrospective, and 9 authors reported that they blinded their cohort. Most of the studies assessed individual vertebrae.17,22,23 In one study, the primary end point only included bone edema,18 and 6 studies performed additional comparisons with CT. One publication described a different cutoff for the Hounsfield unit of 50 HU, whereas another study described different reconstruction algorithms, such as material decomposition and calcium subtraction.20,21 Likewise, the number of DE-CT image interpreters varied as well across studies, ranging between 2 readers18,20,24 and 5 readers.25 Furthermore, different MRI sequences were used in different studies. The majority of authors used a 1.5-Tesla3,17,19–23,25 and short tau inversion recovery sequence.17,18,19,21–24,26 Remaining studies used turbo inversion-recovery magnitude sequences.20,25,27 One study did not report MR tomography for comparison.28
The mean age of patients was 67.6 ± 5.95 years old. Females represented 61.4% (n = 205/334) of cases. In 2 studies, no sex distribution was reported (Table 1).22,26 Two studies did not describe detailed individual DE-CT findings, only the overall sensitivity, specificity, and accuracy.22,27
Demographics of included studies.
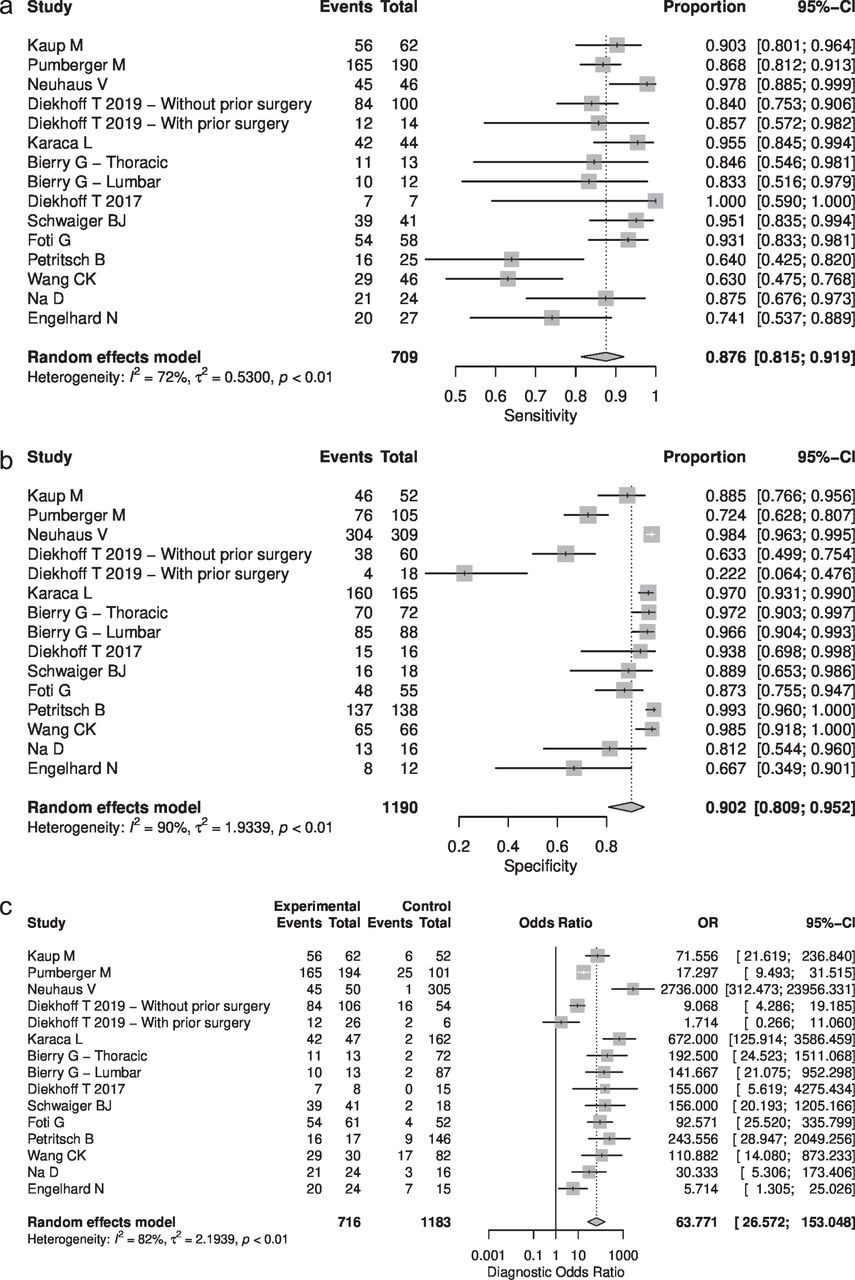
The largest cohort included 76 patients with 774 vertebrae.20,23 Among the individual DE-CT readers, the sensitivity for two-material decomposition filtered back projection ranged from 4.2%,21 76.9%,19 to 100%17,24 and specificity per vertebrae for two-material decomposition raw data ranged from 53.3%,21 66.7%,23 to 100%.17 The overall sensitivity was 86.2% with a specificity of 91.2%. PPV was 85.3% and NPV was 91.7%. The accuracy for two-material decomposition filtered back projection ranged from 38.5%,21 50%,17 to 98.6%,26 with a mean of 89.3%. All findings for DE-CT are presented in Table 2. Heterogeneity was found to be considerable (Higgins I2 > 70%) in all cases (sensitivity, specificity, and diagnostic odds ratio). All findings are illustrated in Figures 2 and 3.
Meta-analysis and findings for dual-energy computed tomography.a
Extended.
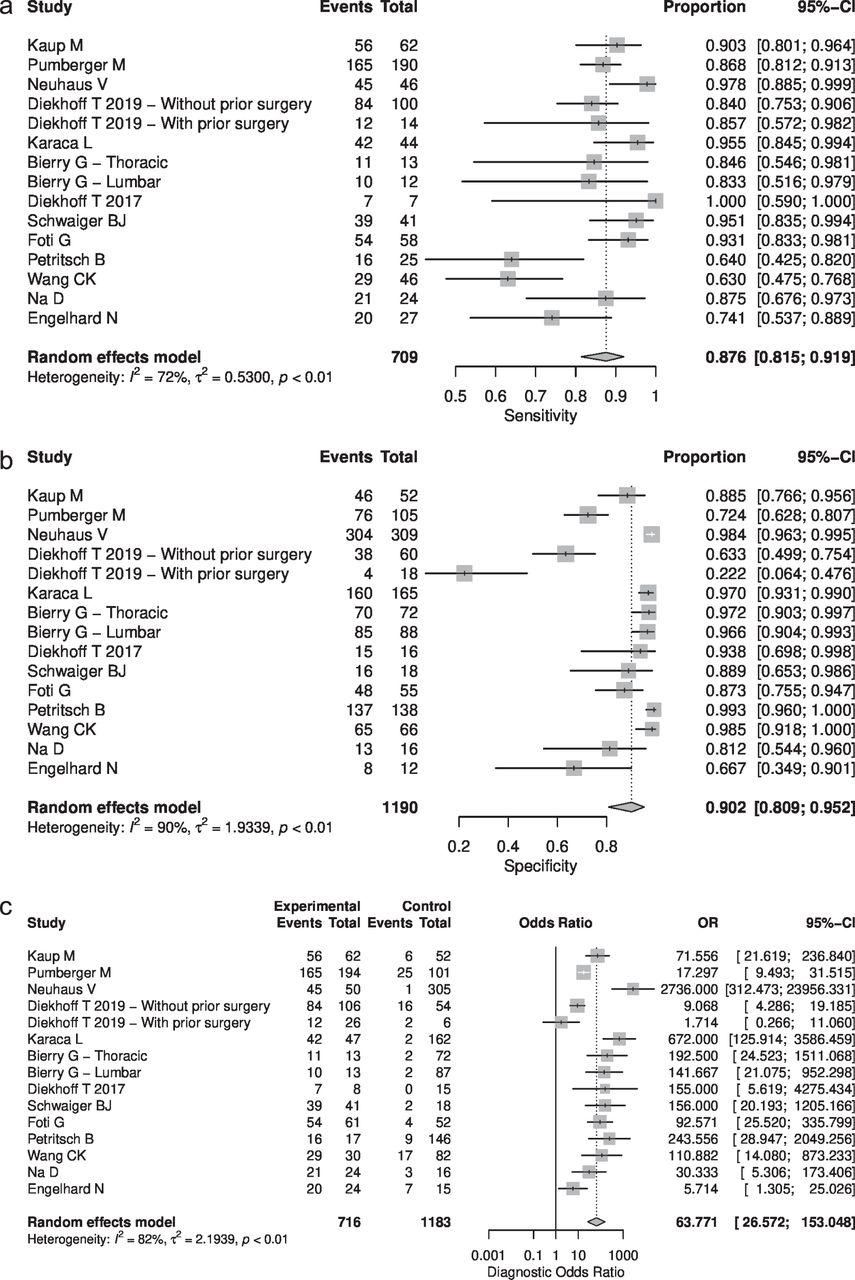
(a) Forest plots for sensitivity, (b) specificity, and (c) diagnostic odds ratio showing the individual proportions including 95% confidence interval and the heterogeneity.
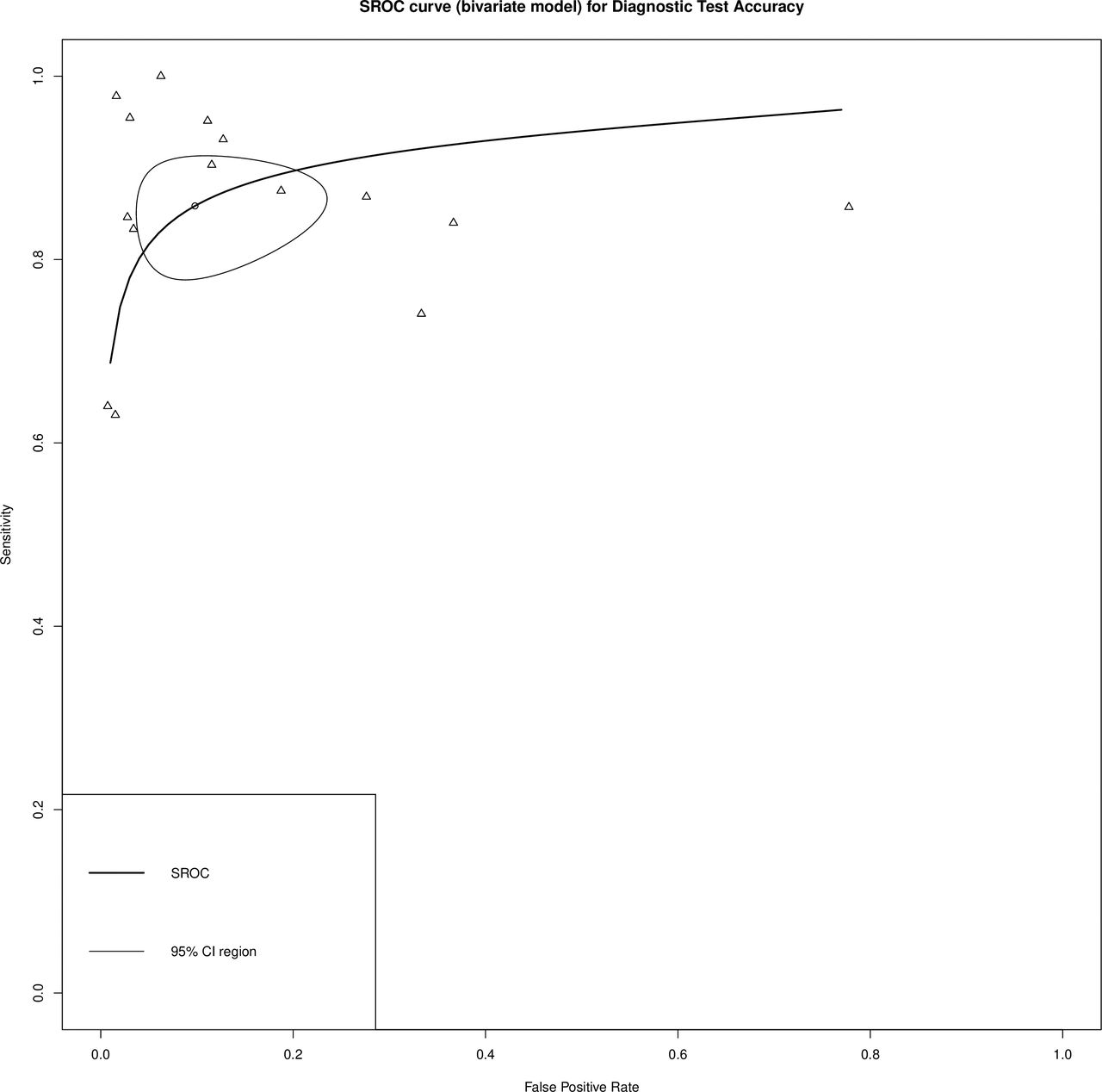
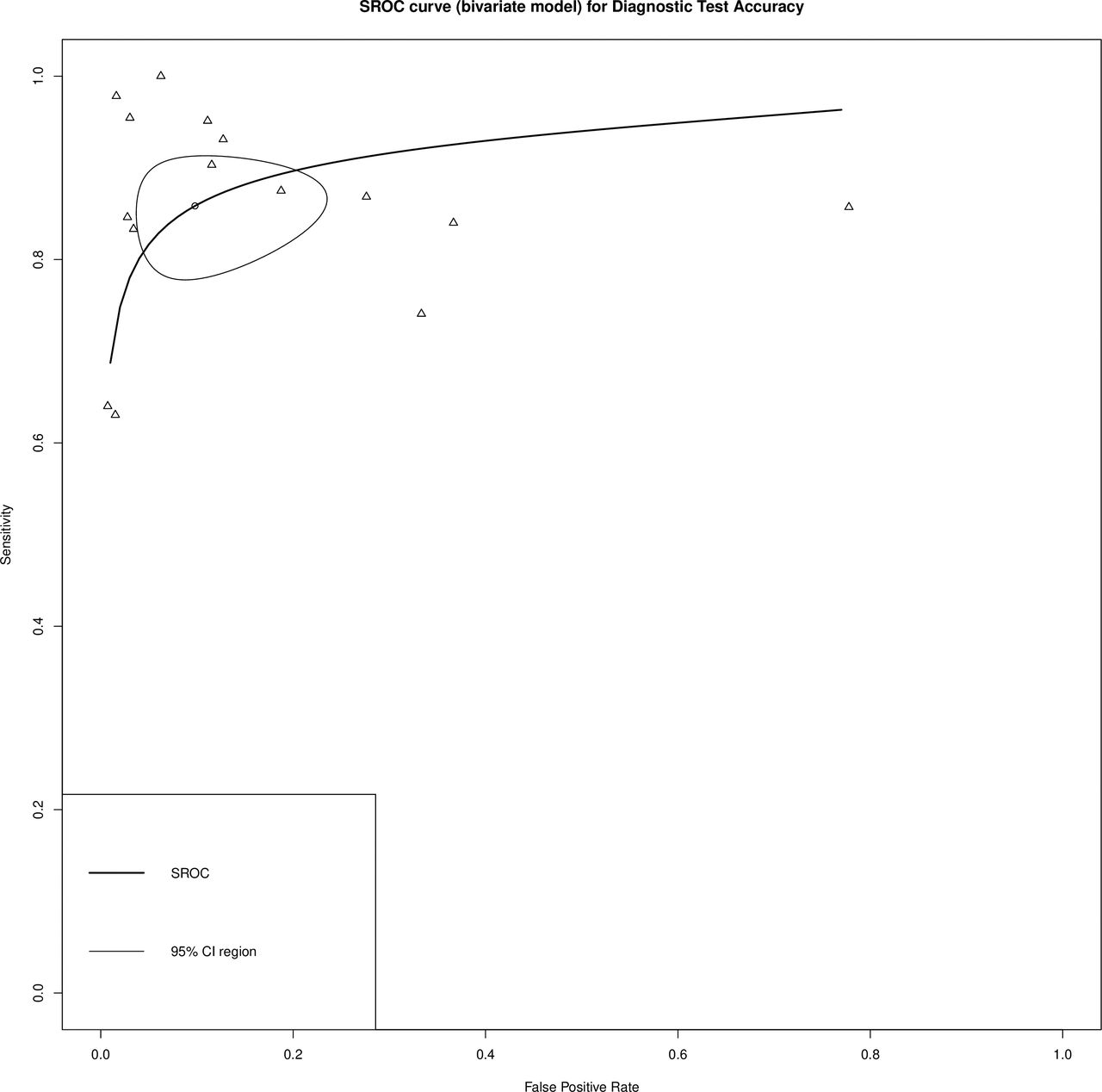
SROC (summary receiver operating characteristic) curve for diagnostic test accuracy between sensitivity and false positive rate for dual-energy computed tomography.
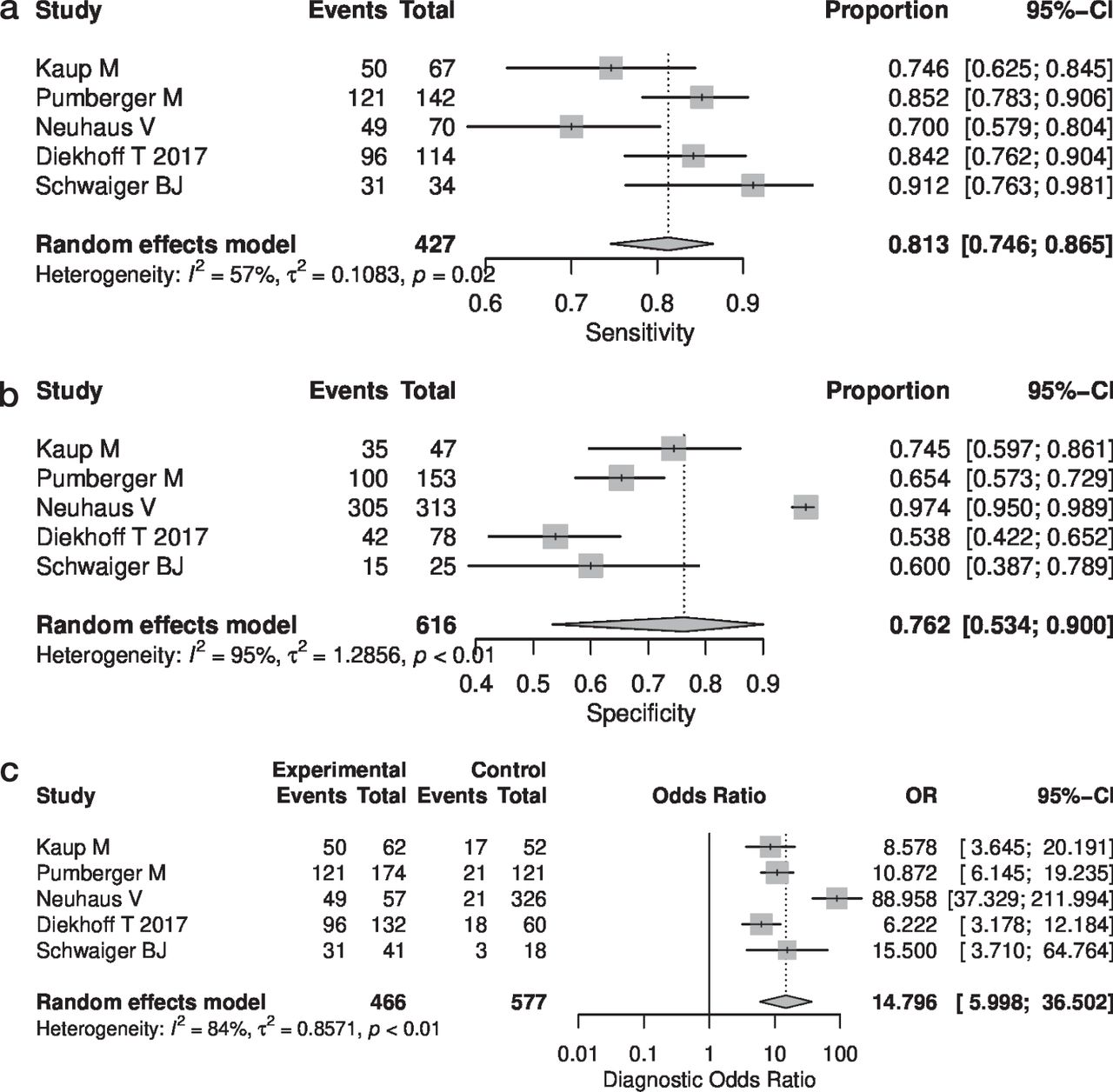
For CT readings, the sensitivity ranged from 69.5%22 to 87.1%25 and specificity was between 40.4%25 and 93.6%.26 Average sensitivity was reported to be 81.3% and 80.7% for specificity. The mean PPV was 74.5% and NPV was 86.1%, with a mean accuracy of 80.9% (Table 3). Hereby, the sensitivity showed only moderate heterogeneity (Higgins I2 = 52%), whereas for the specificity and diagnostic odds ratio, this was considerable (Figures 4 and 5).
Individual findings for sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for computed tomographies.
Extended.
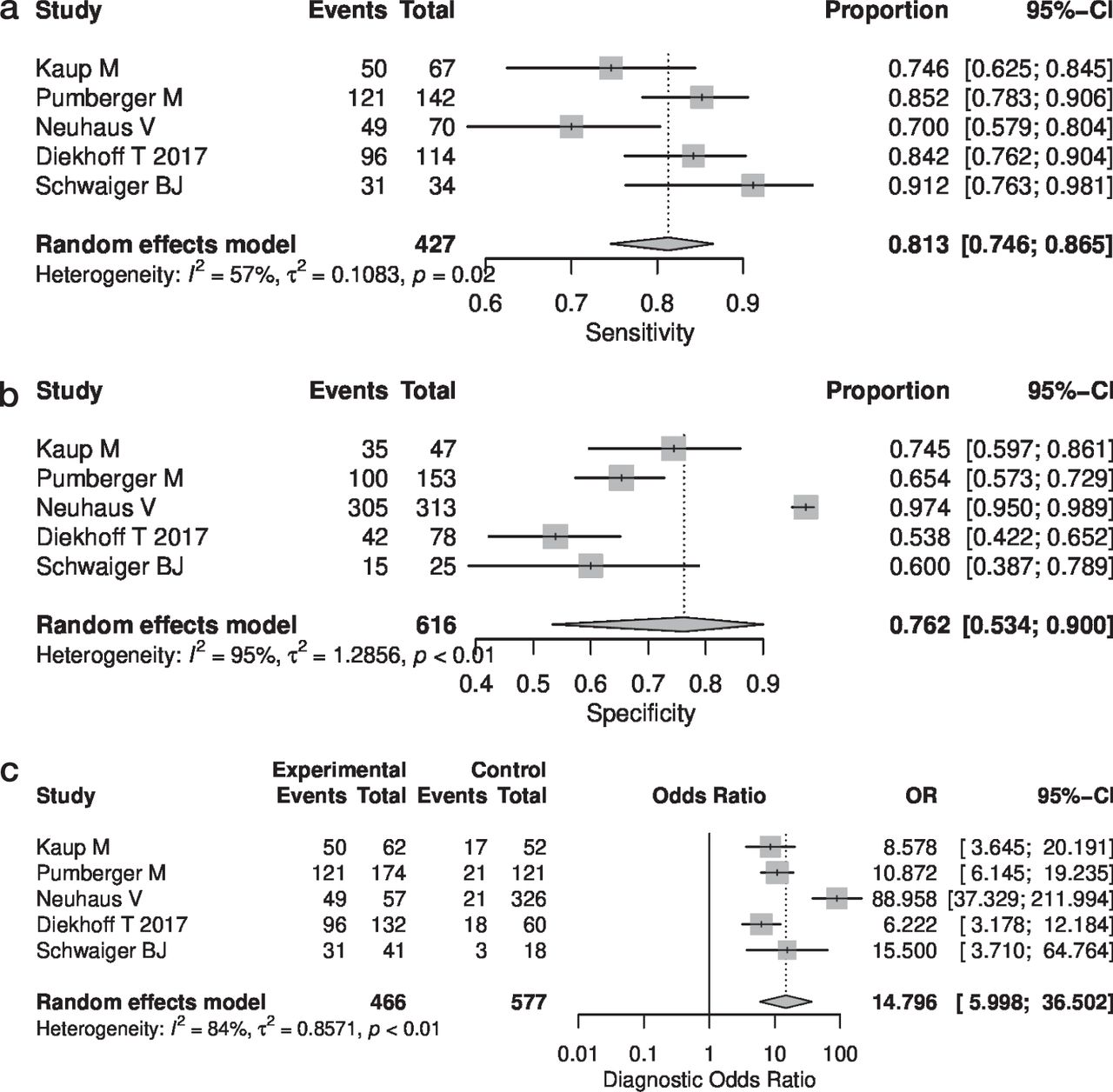
(a) Forest plots for sensitivity, (b) specificity, and (c) diagnostic odds ratio showing the individual proportions including 95% confidence interval and the heterogeneity.

SROC (summary receiver operating characteristic) curve for diagnostic test accuracy between sensitivity and false positive rate for computed tomography.
Specificity and accuracy reported above were found to be statistically significant at P < .001, P = .067, and P = .029, respectively. No significance was found for sensitivity at a P value of .119.
DISCUSSION
This systematic review included 13 studies, totaling 515 patients, 3335 vertebrae, and 926 fractures. Although DE-CT shows higher sensitivity, specificity, and accuracy when compared with conventional CT, significant interobserver differences were identified. Previous literature reviews on DE-CT did not focus on its use in the context of spine injury.10,29,30 Our review is the first study of its kind to our knowledge.
For conventional CT scans, the sensitivity was between 69.5% and 87.1%, and specificity was between 40.4% and 93.6%, with a PPV ranging from 61.3% to 90.9% and an NPV ranging from 53.8% to 97.4%. For DE-CT, the sensitivity ranged from 76.9% to 100% and specificity from 66.7% to 100%. PPV was found to be between 64% and 100% and NPV between 22.2% and 100%. However, Engelhard et al reported high variability for different reconstruction algorithms of DE-CT; two-material decomposition with filtered back projection showed the lowest sensitivity of 4.2% and specificity for raw data at 53.3%.21
Some differences were observed between the individual reader sensitivity and specificities. According to Pumberger et al, the sensitivity was much higher for a radiologist at 89%, a medical student at 86%, and a specialized orthopaedic surgeon at 73%. For specificity, radiologists were reported at 93%, orthopaedic surgeons at 59%, and medical students at 54%.22
According to Bierry et al, accuracy of DE-CT was superior for the thoracic spine as compared with the lumbar spine. While a 50-HU cutoff has been reported to be superior to attenuation measurement of bone bruises in the knee joint, the investigation by Foti et al regarding the usefulness of the 50-HU cutoff for distinguishing between fresh and old vertebral fractures did not find any statistical significance.31
Reconstruction algorithms after calcium subtraction showed slightly better sensitivity of 91.7% when compared with reconstruction algorithms without calcium subtraction (87.5%).28 Additionally, the three-material decomposition algorithm was found to be better than the two-material decomposition algorithm.32 For adaptive iterative dose reduction, no differences between the mild, standard, or moderate iterations were reported.21 In other studies, multienergy CT was observed to have better noise reduction with prior information included.32
Besides the initial diagnostic with conventional radiography and CT, the gold standard for diagnosing bone marrow edema and disc edema, such as in nondisplaced spine trauma, is MRI, although its ability to detect fractures may vary depending on the etiology, namely osteoporotic versus malignant causes.1,33 MRI identifies subtle bony edema seen in compression fractures that would otherwise be missed by conventional radiography. For stress fractures in the lumbar spine, the sensitivity was reported at 99.6%, specificity at 86.7%, and accuracy at 97.2%. Higher accuracy has been reported at the lower lumbar levels.34 Interestingly, greater interobserver variation was observed in patients with intact pars interarticularis.35
According to Lenchik et al, DE-CT sensitivity for bone marrow edema in osteoporotic vertebral fractures is described to be 92% with a specificity of 96%. Yang et al performed a meta-analysis on 7 studies assessing the accuracy of DE-CT for vertebral fractures. Sensitivity and specificity was described to be 89% and 98%, respectively.30 This is much higher than what was found in our systematic review.36 Although CT shows less accuracy than DE-CT for detecting vertebral fractures, the experience and familiarity of most image interpreters with regular CT may bias this result. Another important factor is the time elapsed between the accident and the time of imaging, as the sensitivity increased if the interval was more than 2 days.30 Use of MRI is limited by metal implants in patients, availability of MRI in clinics, and individual risk factors, such as cardiopulmonary instability or claustrophobia. In those cases, DE-CT can be a reasonable alternative to MRI.
A DE-CT, uses 2 scintillation layers (2 sources of x-ray), 1 normal and a second less powerful x-ray with 2 corresponding detectors. In rapid kVp switching, the tube voltages follow a pulsed curve, which is collected twice for every projection at high and low tube voltage. Therefore, the 2 scintillation layers enable a separation between the high and low energy spectra.37
There are several limitations to this study as this is a systematic analysis and meta-analysis. Four studies were performed by Dr Diekhoff's group.17,21–23 Individual findings for the different observers were not consistently reported. Only a few studies reported both the intraobserver and interobserver reliability.18–20,24 Furthermore, different kinds of MRI were used as gold standards for comparison to detect bone marrow and disc edemas. Although all studies wanted to report the accuracy of DE-CT, the studies did not use the same reconstruction algorithms or cutoffs across the board, making comparison difficult. The largest cohort included only 76 patients.20,23
CONCLUSION
DE-CT seems to be a promising diagnostic tool to exclude bone marrow and disc edema in any acute spine injuries where MRI cannot be performed, as evidenced by our systematic review and meta-analysis. However, the literature still supports the use of MRI as the gold standard. But as familiarity and access to DE-CT improves, inter- and intraobserver agreement will likely improve as well. DE-CT has the potential to replace MRI as the diagnostic modality of choice for spine injuries in some settings.
Footnotes
Disclosures and COI: The authors declare no conflict of interest related to this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.