

Abstract
Background Degenerative spondylolisthesis is associated with a significant segmental kyphosis at the level of the listhesis. We treated 7 disc spaces with Grade 2 listhesis and/or kyphosis of the slipped disc level with Kineflex disc replacement.
Methods Out of a single-center prospective registry, involving 310 lumbar disc replacement patients, 7 patients underwent a single-level Kineflex disc replacement at the level of a degenerative spondylolisthesis with either segmental kyphosis or a Grade 2 slip.
Preoperative and follow-up radiological parameters studied were: pelvic incidence, pelvic tilt, sacral slope, lumbar lordosis L1-S1, degree of segmental listhesis, segmental lordosis, and range of motion (ROM). Clinical outcome measures were Visual Analog Scale pain score (VAS), Oswestry Disability Index (ODI), and patient satisfaction.
Results Five replacements were performed at the L4-L5 level, and 2 were performed at a L3-4 level, above a pre-existing L4-S1 posterolateral fusion. Mean age was 50 (32–62) years. Average follow-up was 23.8 ± 13.1 months. Six of 7 patients considered their outcome as good or excellent. The mean VAS score decreased from 8.4 ± 1.9 to 2.7 ± 2.2 (P < .01). The ODI decreased from 45.2 ± 9.9 preoperatively to 19.7 ± 12.8 (P < .01).
There were increases in lumbar lordosis (from 47.4o ± 10.6 to 61.3o ± 8.0 (P < .03)), in segmental lordosis (from 0.17° ± 7.0° to 16.4° ± 2.0° (P < .03)), and in sacral slope (from 34.5° ± 4.8° to 40.7° ± 4.5° (P < .03)). There were decreases in pelvic tilt (from 22.6° ± 6.3° to 15.5° ± 5.9° (P < .05)), and degree of segmental listhesis (from 24.4% ± 7.7 to 3.7% ± 3.4 (P < .03)). Pelvic incidence and ROM did not change.
Conclusions Disc replacement resulted in significant improvement in clinical outcome and excellent sagittal balance and slip correction. However, the influence of improved sagittal spinal alignment on clinical outcomes needs to be investigated in larger studies including a control group.
Clinical Relevance This study is the first focused on disc replacement in degenerative spondylolisthesis.
- Spondylolisthesis
- total disc replacement
- radiological outcome
- clinical outcome
INTRODUCTION
Degenerative spondylolisthesis (DSPL) is a condition where degenerative changes in disc and facet joint complex lead to vertebral displacement, resulting in spinal stenosis, recess stenosis, and segmental kyphosis.1 Reports are mostly retrospective, and randomized studies have only compared surgical treatment consisting of posterolateral fusion with or without instrumentation and with posterior decompression alone.2
The influence of sagittal alignment on the generation of lower back pain (LBP) and degeneration of the lower back is not well understood. Despite existing suspicion that pre- existing differences in sagittal alignment may influence the occurrence of LBP and that outcome of fusion surgery may be dependent on restoration of lumbar lordosis during surgery,3 only recently a classification system to measure and classify sagittal alignment has been published.4 It has been applied to pathological conditions of the lumbar spine such as DSPL.5
Anterior lumbar interbody fusion (ALIF) surgery reliably corrects sagittal imbalance and listhetic slip in significant segmental kyphosis associated with DSPL.1, 6, 7 Anterior column support was recommended by Sengupta and Herkowitz for patients with Grade 2 spondylolisthesis or higher or when kyphosis was present.8
Dynamic posterior motion preservation in DSPL renders significant clinical improvement despite minimal sagittal alignment changes2, 9–12 and despite increase in facet arthrosis.11
Despite the potential positive effect on spinal alignment and degree of spondylolisthesis, significant DSPL is considered a contraindication for total disc replacement (TDR). Complications from inadvertently instrumented spondylolytic disc spaces have been presented, but objective confirmation of the outcome of TDR in DSPL is missing.
The Kineflex disc prosthesis (Spinal Motion; Mountainview, California) is a chrome-cobalt-molybdenum (BioDur CCM Plus; Carpenter Technology Corp., Wyomissing, Pennsylvania), unconstrained but recentering disc prosthesis with a variable center of rotation. The mechanism comprises 2 metal endplates articulating over a sliding core, which is positioned between the endplates. It allows 12° of movement into flexion, extension, and left- and right-sided bending. The inferior endplate has a retaining ring that limits the excursion in the inferior articulation to 2 mm in all directions and prevents dislodgement of the sliding core. The mechanism therefore only allows 4 mm of translation before distraction of the disc space; a recentering force is produced that counteracts the translation. The disc is inserted as a single unit with a freely mobile mechanism during the final insertion process to facilitate placement posteriorly within the disc space. The objective in the development of this prosthesis was to facilitate reliable midline and posterior placement of the implant within the disc space in severely degenerative disc spaces, through a minimally invasive approach.13
The insertion technique of this disc prosthesis is unique. After the initial engagement into the disc space of the fully assembled 3-component prosthesis, the insertion tools allow independent advancement of the superior and inferior prosthetic endplates. During this process the advancing endplate pivots over the sliding core, taking pressure off the leading prosthetic endplate/bone interphase.13 We therefore postulated that, through independent advancement of the inferior endplate, this particular disc prosthesis should be able to assist spondylolisthesis reduction during the insertion process.
We are reporting on the operative reduction technique in DSPL and on the outcome of 7 patients with either a Grade 2 spondylolisthesis and/or kyphosis of the slipped disc level and who were treated with Kineflex disc replacement.
MATERIAL AND METHODS
Out of a single-center prospective registry involving 310 lumbar disc replacement patients, 7 patients were retrieved from our databank of patients who had undergone a single-level Kineflex disc replacement at the level of a degenerative spondylolisthesis with either segmental kyphosis or a Grade 2 slip.
Operative Technique
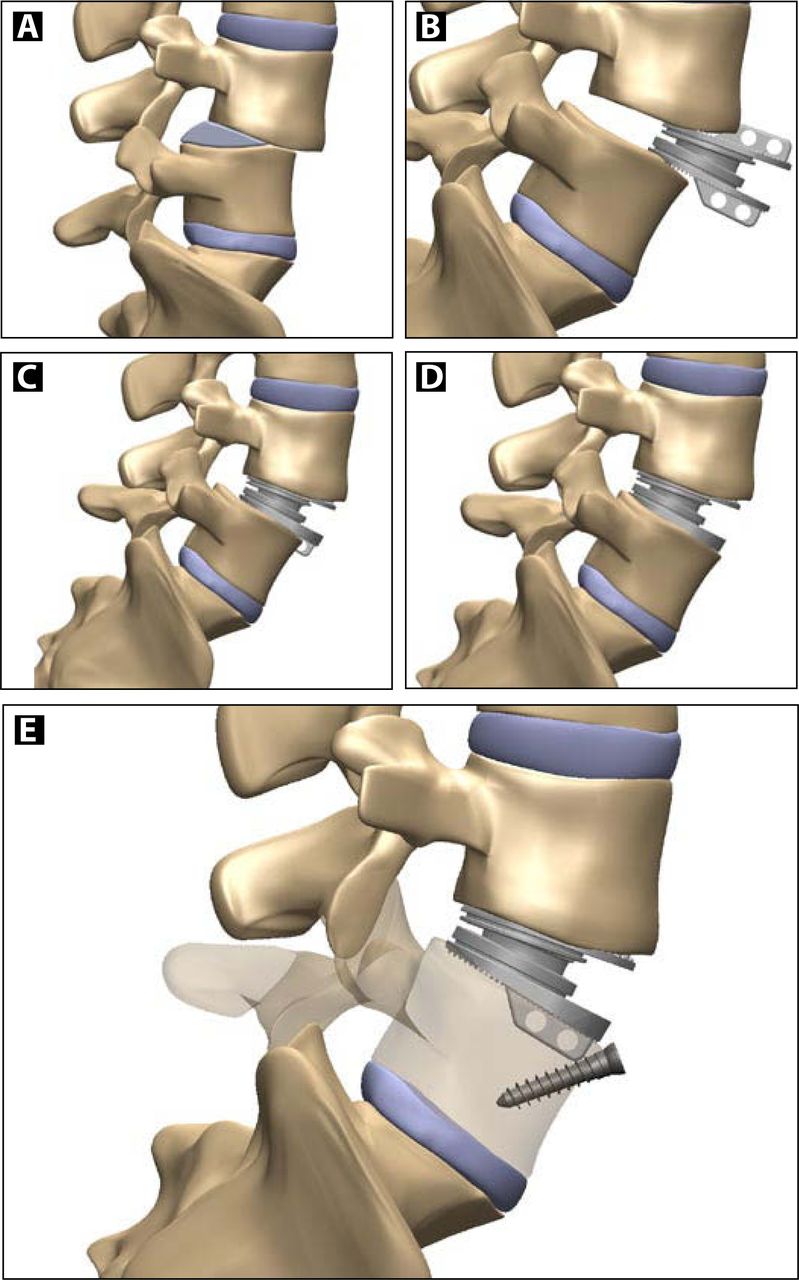
The operations were performed through a left-sided retroperitoneal approach, followed by the creation of a wide exposure of the disc space. After a midline anuloplasty, a complete nucleotomy was performed, and the inner, desiccated layers of the annulus were removed. The disc space was mobilized, and the bony endplates were prepared. The correct-sized prosthesis was selected. As hypermobility was an anticipated complication, the disc height selected was one size larger than we would have chosen in a standard disc replacement. After initial engagement of the prosthesis, the mechanism of the prosthesis was released, and the endplates were advanced until almost flush with the posterior wall of the inferior vertebral endplate of the cephalad vertebra. Thereafter, the inferior prosthetic endplate was further advanced until almost full spondylolisthesis reduction was achieved. Additional screw fixation of the inferior endplate was performed, whenever further primary fixation was thought to be necessary, in order to absorb excessive forces through the inferior prosthetic endplate/bone interphase (Figure 1).
Insertion Technique
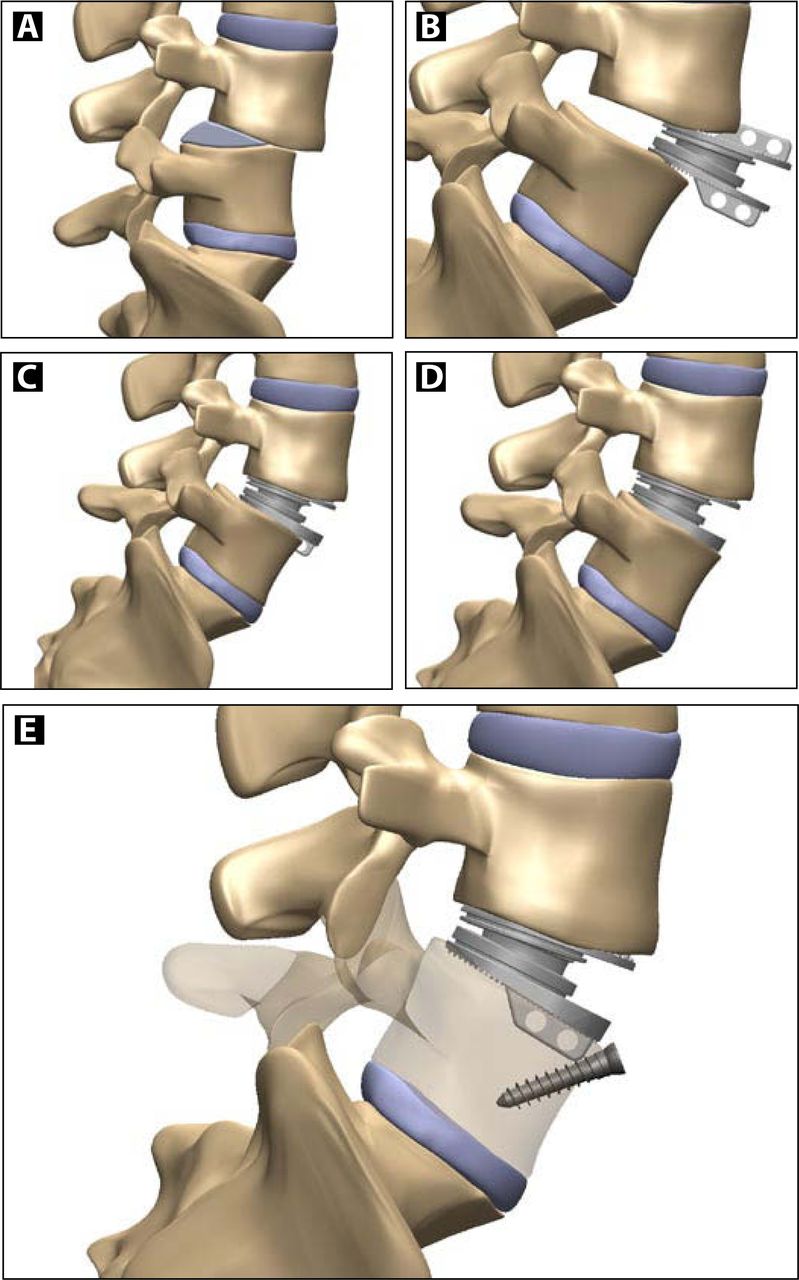
Position A: Spondylolisthetic disc space before operation. Position B: Initial engagement of the prosthesis into the disc space after full nucleotomy, disc space mobilization, and cutting of the insertion grooves. The further insertion is performed with a fully freed prosthetic mechanism. Position C: Advancement of the prosthesis into the disc space, until almost flush with the posterior wall of the cephalad vertebral body. The prosthetic endplates are individually advanced, alternating between top and bottom prosthetic endplate. Position D: Further advancement of the bottom prosthetic endplate, until almost flush with the posterior wall of the caudad; full reduction of the spondylolisthesis. During this advancement the inferior endplate pivots around the articulating mechanism of the prosthesis, reducing the pressure between the leading edge of the inferior prosthetic endplate and the bony endplate. Position E: Securing of the final reduced position by placement of a screw into the into the insertion groove of the inferior vertebra. This counteracts the displacing forces (For more information on insertion technique, see Hähnle et al.13)
Radiographic Evaluation
All patients had a preoperative magnetic resonance image (MRI) or lumbar myelography followed by computer tomography (CT), or both.
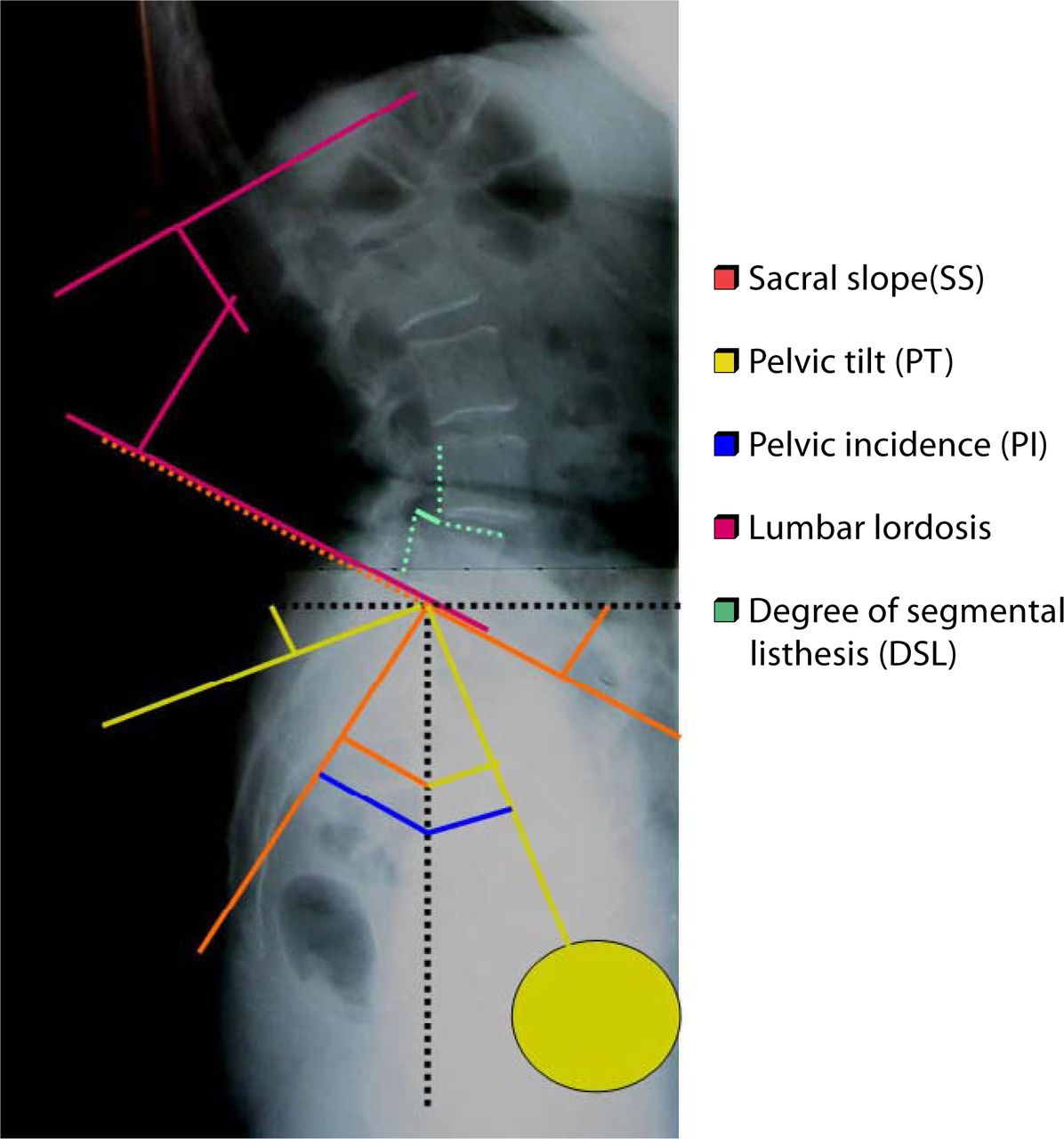
Preoperatively and postoperatively at 3 months, 6 months, and yearly, anteroposterior (AP), lateral standing radiographs that included the bottom endplate of the T12 vertebra and the top half of both femoral heads were performed. In addition, a lateral, whole-spine, standing radiograph was included. The patients were asked to stand straight with arms crossed over the chest and knees fully extended. Lateral flexion/extension radiographs were also performed at these follow-ups. The spinal balance evaluation was based on the studies of Duval Beaupere et al.14–16 and Lazennec et al.17 (Figure 2). We looked at pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), lumbar lordosis (cephalad endplate L1–cephalad endplate S1) (LL), and segmental lordosis (SL) within the instrumented disc space. If the femoral heads were not exactly superimposed on each other, the middle of the line connecting the centers of the femoral heads was used to determine the PI and PT. We further studied the degree of segmental listhesis (DSL) on a percentage basis. The range of motion (ROM) at the level of DSPL was measured on flexion/extension radiographs by 2 of the investigators (U.H. and I.W.), preoperatively by the Cobb method and postoperatively by the fin method.18
Lumbar Disc Replacement in DSPL Measurements
Lumbar disc in DSPL-measured parameters. Pelvic incidence (PI), sacral slope (SS); pelvic tilt (PT), lumbar lordosis (cephalad endplate L1–cephalad endplate S1) (LL)
Clinical Evaluation
Clinical outcome was measured using the visual analogue pain score (VAS), Oswestry Disability Index (ODI),19 patient satisfaction, and “return to work” data. Complications were described.
Statistical Analysis
Data were reported as mean ± standard deviation with SAS V9.1 (SAS Institute Inc., Cary, North Carolina) for statistical analysis and comparisons. Changes in measured variables pre- and postoperatively were compared using a nonparametric Wilcoxon matched pairs test with a P value < .05 regarded as significant.
RESULTS
Seven patients were retrieved from our databank who had undergone a single-level Kineflex disc replacement at the level of a spondylolisthesis with either segmental kyphosis or a Grade 2 slip or both and had undergone the index procedure at least 1 year before. They were called in for clinical and radiological follow-up; these patients form the base of this study.
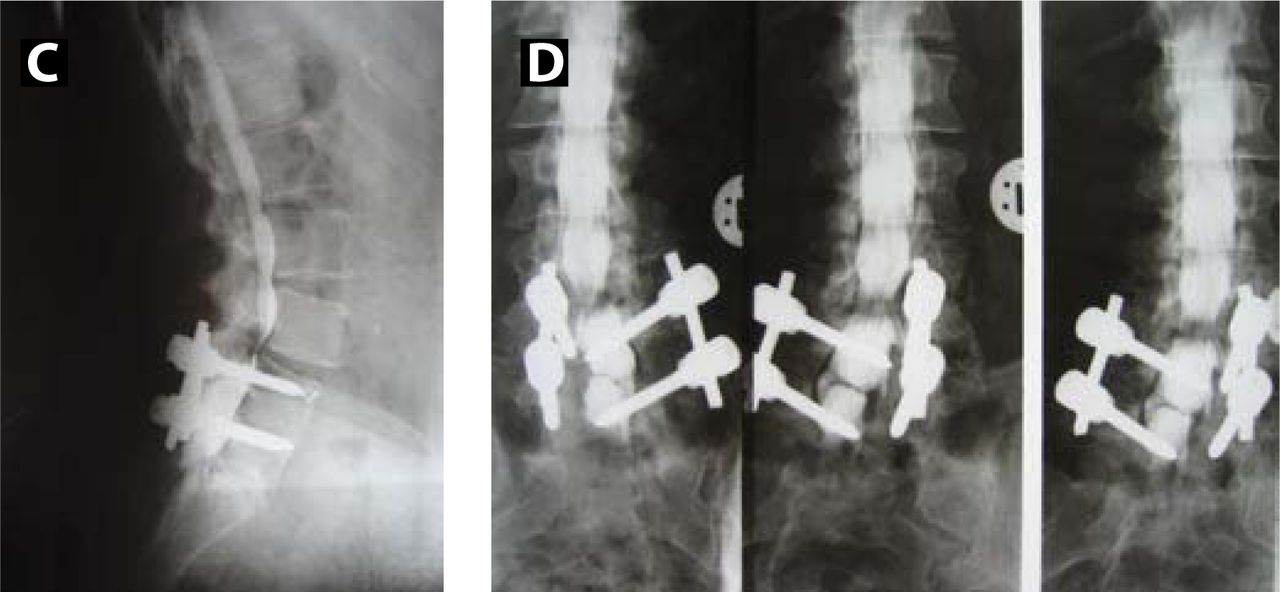
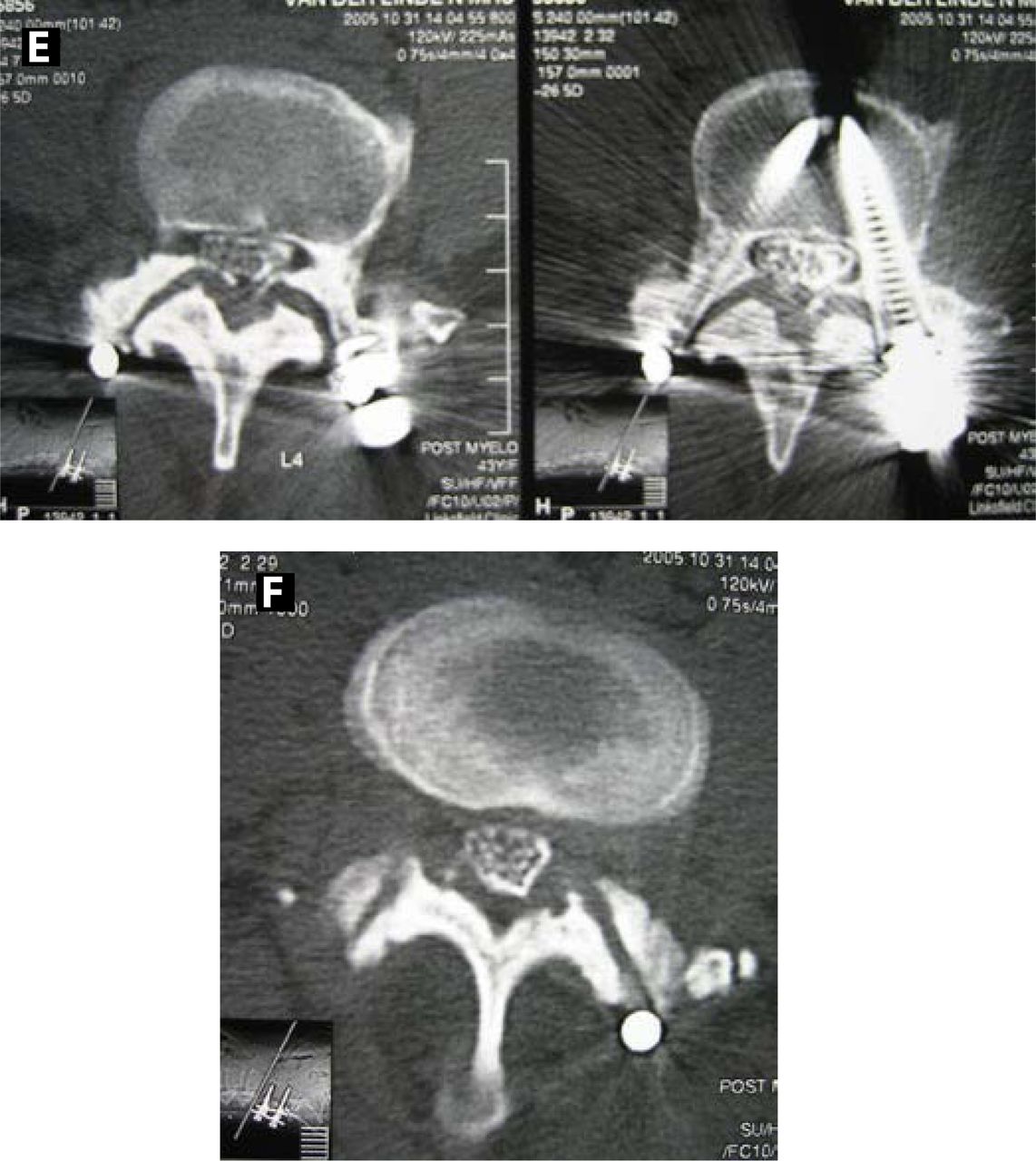
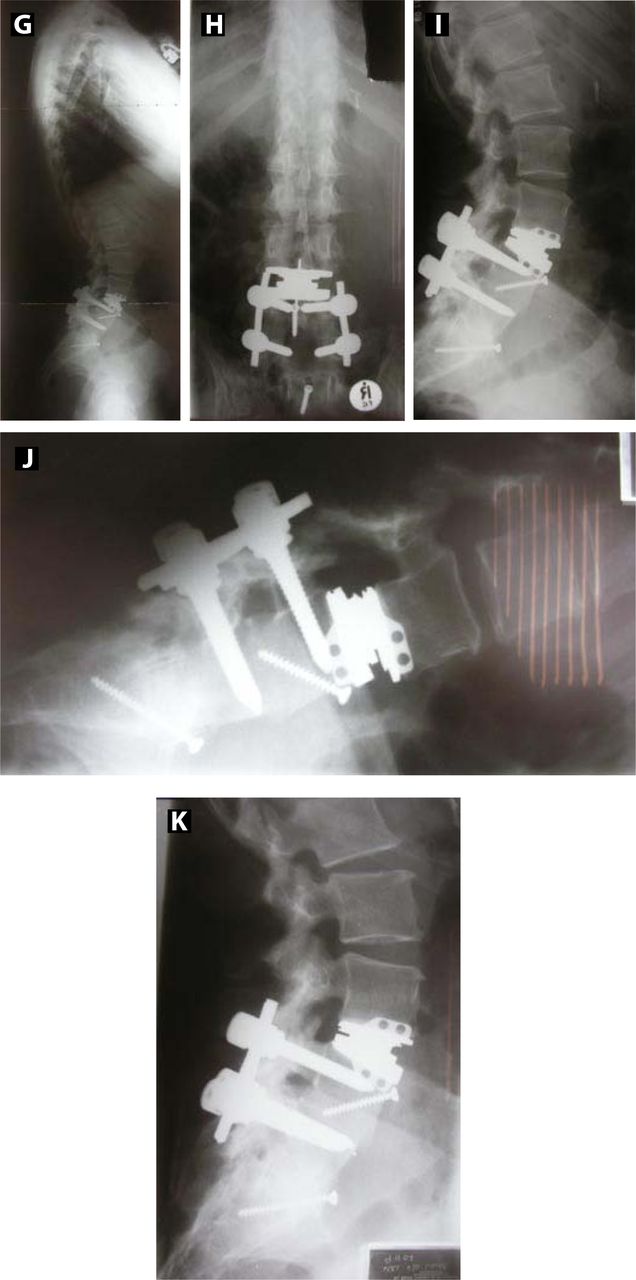
Five disc replacements had been performed at the L4-L5 lumbar level. In one operation a posterior motion preservation device, inserted 2 years prior to the index operation, had first been removed through a posterior approach before the prosthetic disc insertion during the same anesthetics. Two disc replacements had been performed at a L3-L4 level, above a pre-existing L4-S1 posterolateral fusion (Figure 3). The average age at the time of the index procedure was 50 (32–62) years. Five of the patients were female. All patients had originally presented with symptoms of mechanical LBP and leg pain. Five patients had complained with symptoms of spinal stenosis.
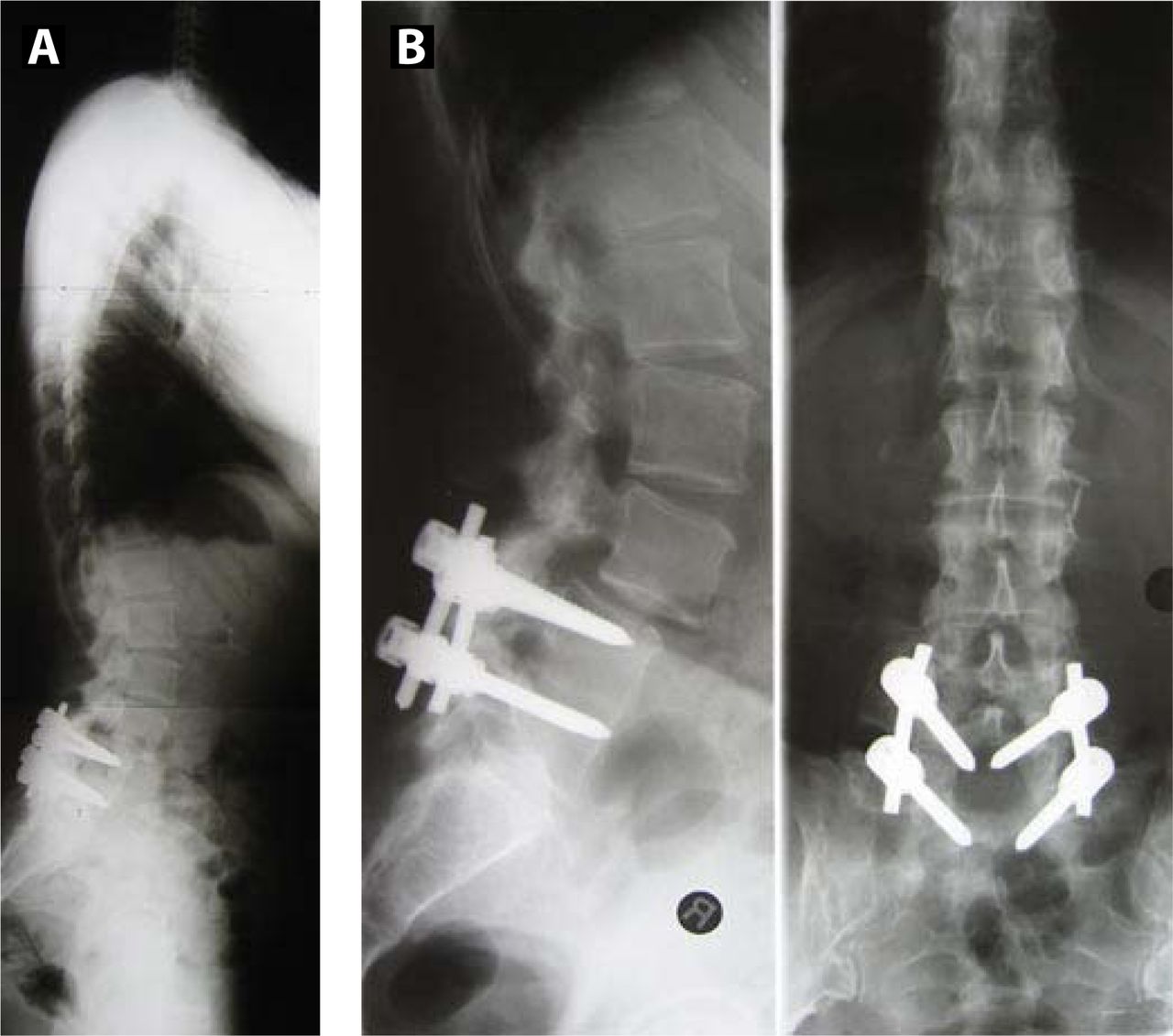
43-year-old active lady with severe LBP and SS symptoms. Posterolateral fusion L4-S1 4 years before.
One of the 7 patients had a previous posterior dynamic system inserted by another surgeon 2 years prior to our operation. This person is not a DSPL patient, but the previous surgery resulted in a radiologically similar picture. The operation had left her with significant posterior distraction, segmental kyphosis, and instability. She refused fusion surgery. We therefore performed posterior implant removal followed by anterior TDR surgery.
The postoperative hospital stay averaged 3.3 days (2–8 days) with all patients returning to work after 27 days (3–42 days). The average follow-up was 23.8 ± 13.1 months. One of the patients considered the outcome as fair, 2 as good, and 4 as excellent. Six patients “would undergo the operation again,” and one “doesn't know.” The VAS score decreased from 8.4 ± 1.9 to 2.7 ± 2.2. The ODI decreased from 45.2 ± 9.9 preoperatively to 19.7 ± 12.8.
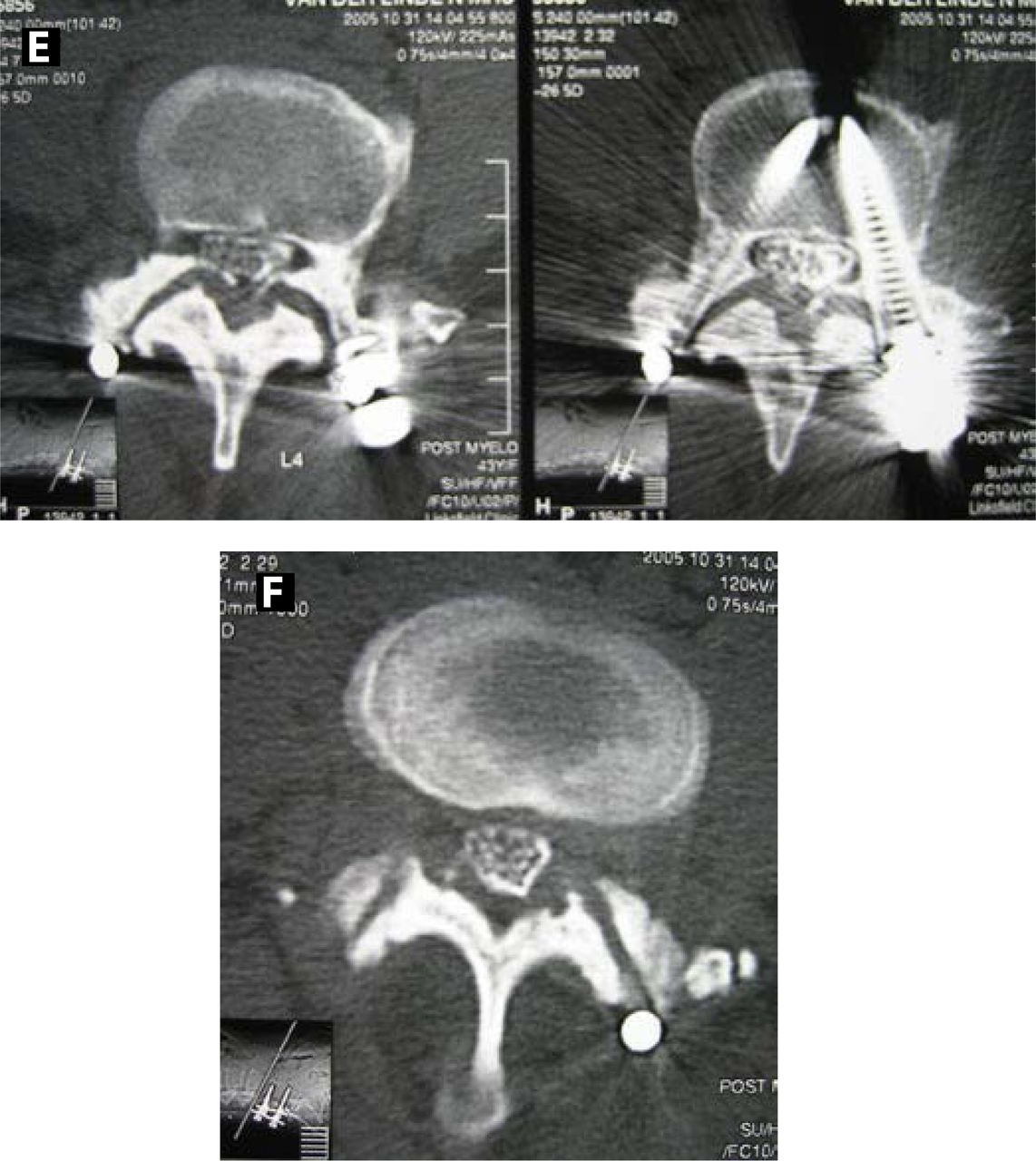
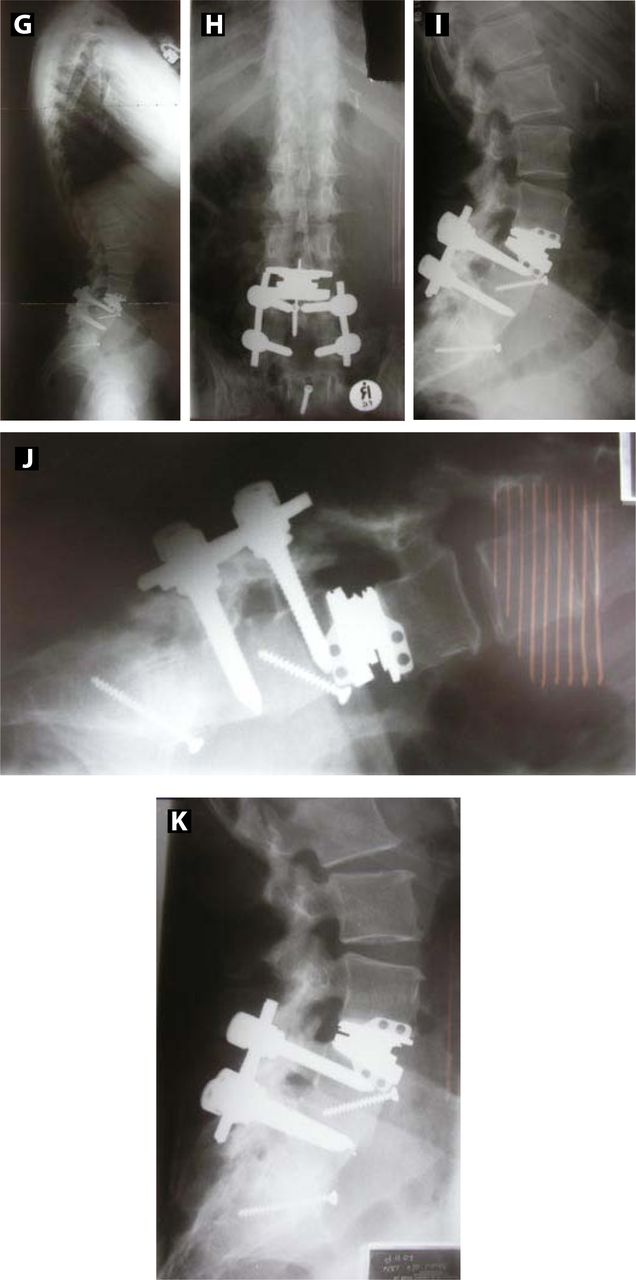
One patient was reoperated at 1 week postoperatively for partial extrusion of the inferior prosthetic endplate over the malpositioned buttress screw (Figure 4). One patient developed a left iliac deep vein thrombosis (DVT).

Myelogram confirms severe SS
CT Myelogram shows severe facet arthrosis.
2-year follow-up: good clinical (ODI = 22, VAS = 2) and radiological outcome.
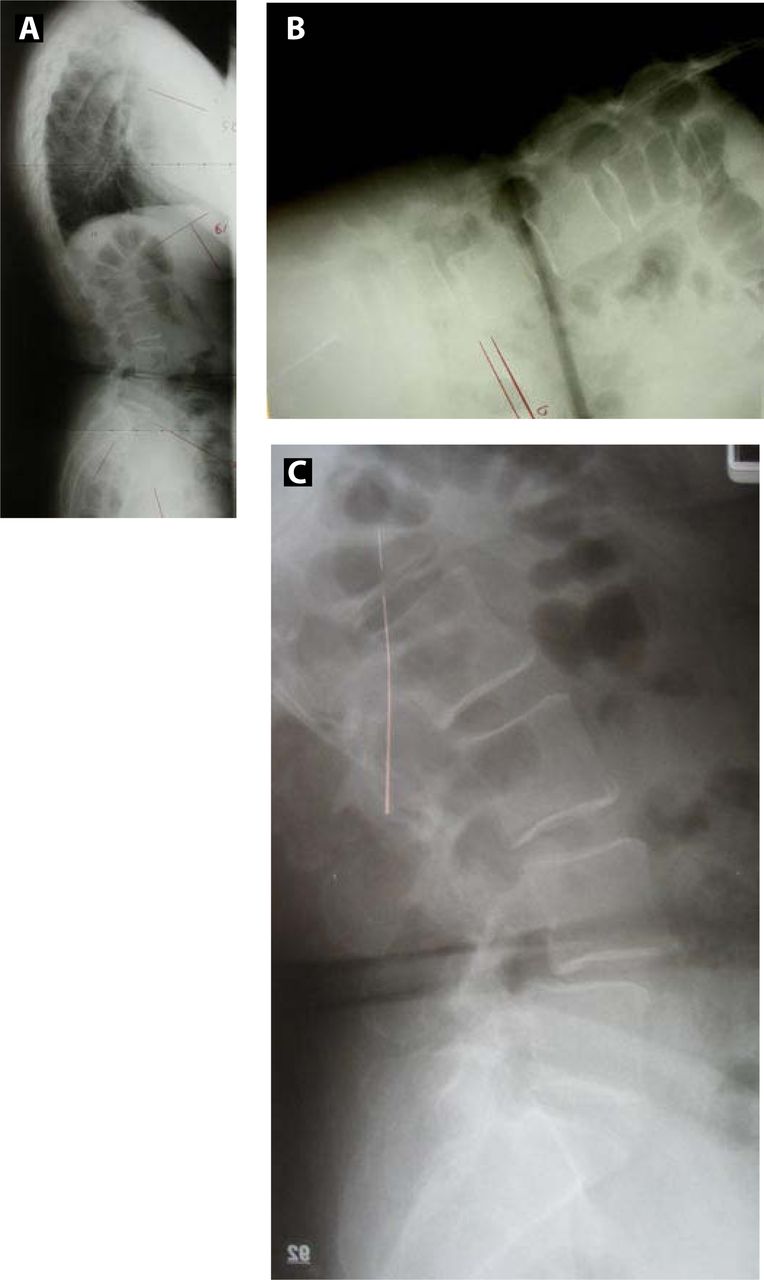
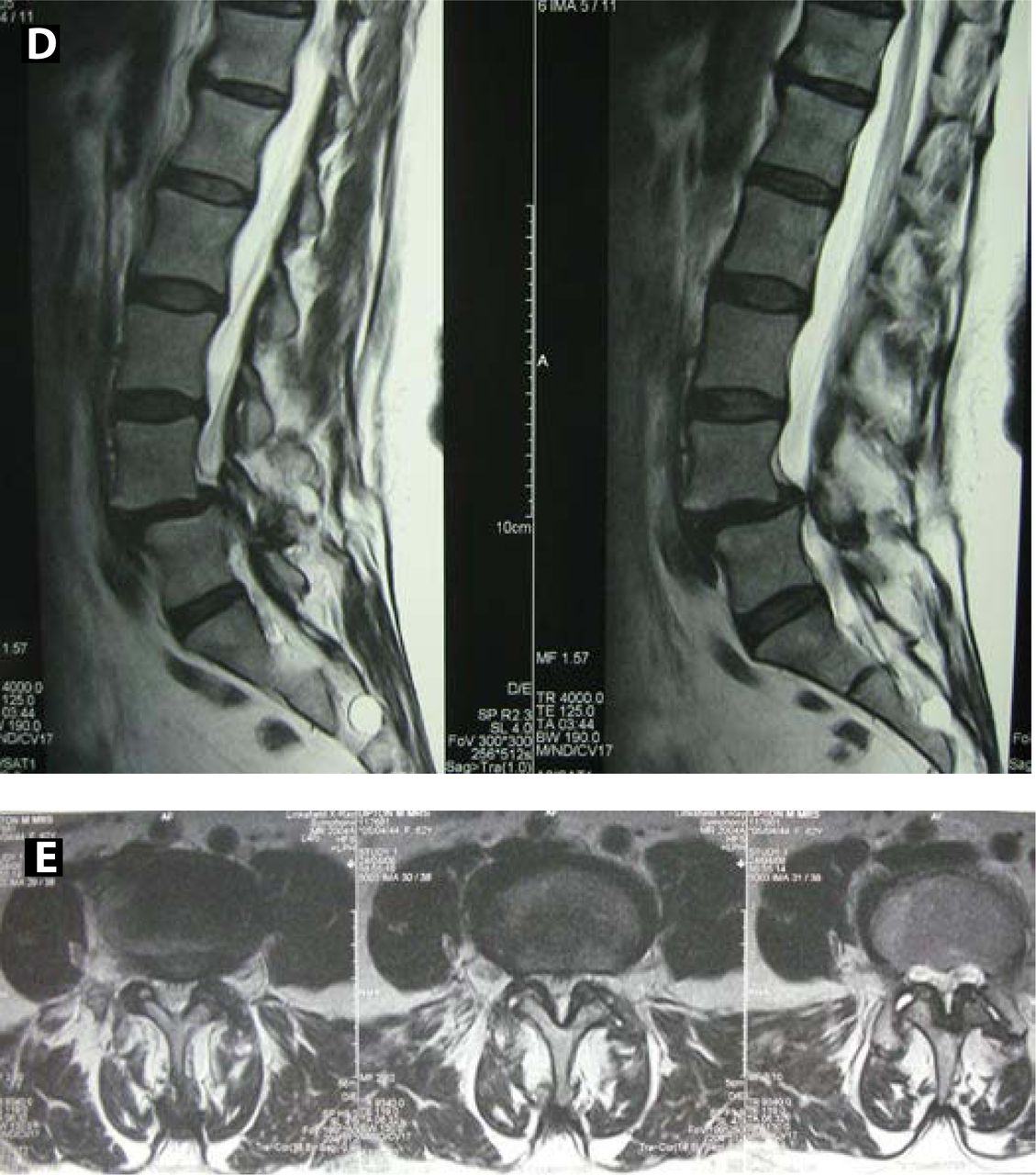
62-year-old patient with severe mechanical LBP and right-side leg pain for 2 years.

MRI scanning shows partial reduction of listhesis in lying position, significant L4-L5 facet degeneration and DDD.

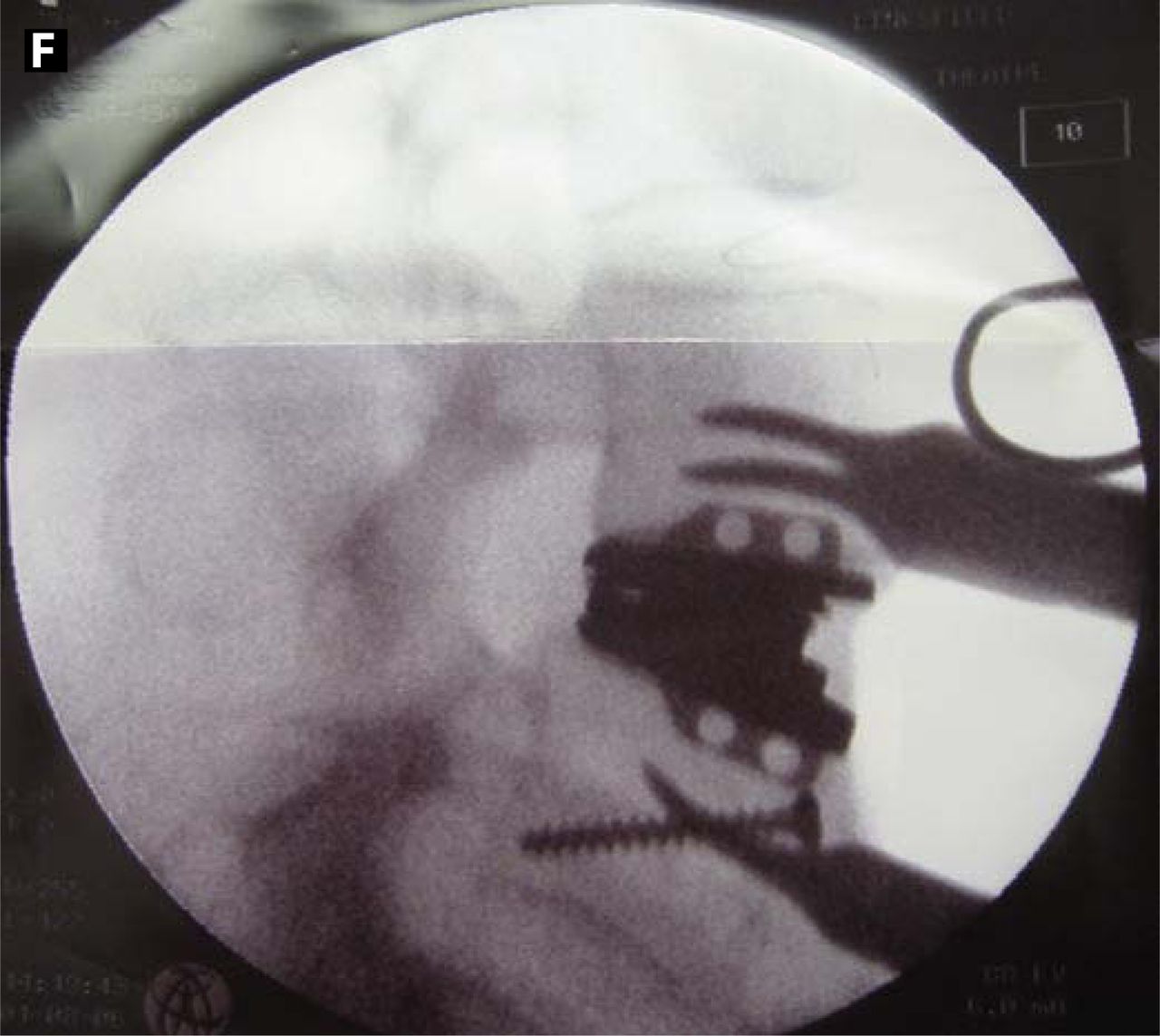
Intraoperative radiograph shows good alignment and listhesis reduction.

(G) Partial extrusion of inferior prosthetic endplate at 2 days. (H) Further extrusion of inferior prosthetic endplate at 6 days.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2 years after reoperation to reposition inferior endplate: excellent clinical (ODI = 0; VAS = 0) and radiological outcomes.
The lumbar lordosis (LL), segmental lordosis (SL), and sacral slope (SS) increased. LL increased from 47.4° ± 10.6° to 61.3° ± -8.0° (P < .03); SL from 0.17° ± 7.0° to 16.4° ± 2.0° (P < .03); and SS from 34.5° ± 4.8° to 40.7° ± 4.5° (P < .03). The pelvic tilt (PT) and the degree of segmental listhesis (DSL) decreased. PT decreased from 22.6° ± 6.3° to 15.5° ± 5.9° (P < .05); DSL from 24.4% ± 7.7 to 3.7% ± 3.4 (P < .03). The pelvic incidence (PI) did not change (preoperative PI was 56.25 while the latest follow-up was 56.5). The change in ROM was insignificant (11.9° ± 5.0° preoperatively to 11.6° ± 3.6° at the latest follow-up). Due to the small cohort no correlation could be drawn between clinical outcome and changes in radiological parameters.
DISCUSSION
The etiology of degenerative spondylolisthesis (DSPL) is poorly understood. Sagittal orientation of the facet joint has been implicated as a predisposing factor20 but might be instead a consequence of the remodelling taking place during development of facet arthritis.21 Controversy exists as to whether the pathology starts primarily in the facet joints22 or within the intervertebral disc.1 Whatever the etiology, the result is segmental spondylolisthesis, segmental kyphosis, spinal and recess stenosis, and facet joint arthritis.
Our cohort of patients consisted of 3 different entities: degenerative spondylolisthesis proper, adjacent segment disease (ASD) with resulting (degenerative) spondylolisthesis at the adjacent segment, and 1 iatrogenic spondylolisthesis caused by an over-distracted posterior device. The resulting clinical and radiological picture is very similar. Clinical patients complained about mechanical LBP and leg pain, inability to stand or walk longer distances. Radiologically, the deformity resulted in low lumbar flat back deformities with compensatory retrolisthesis of the higher lumbar motion segments and flexion of the pelvis on lateral standing radiographs. In each of the 3 entities the resulting surgical treatment aim is similar: decompression of neural structures, stabilization of the motion segment, and restoration of the spinal balance. As we are primarily describing a surgical technique aimed to treat these different components, we considered it justifiable to sum these patients together.
Most surgical outcome studies on DSPL were retrospective and not controlled. Randomised studies have only compared surgical treatment consisting of posterolateral fusion with or without instrumentation and with posterior decompression alone.2 Long-term outcome of surgical treatment seems more favorable with fusion than without fusion.23, 24
Anterior lumbar interbody fusion (ALIF) surgery reliably corrects sagittal imbalance and listhetic slip in significant segmental kyphosis associated with DSPL.1, 6, 7 Anterior column support was recommended by Sengupta and Herkowitz for patients with Grade 2 slips or higher or when frank kyphosis is present.8
More recently Choi and Sung reported on a large patient group, 14 patients with DSPL, using single-level standalone rectangular cages. At 27 months follow-up there was subsidence of over 2 mm in 77% of patients and a 13% nonunion rate, but neither correlated with recurrence of symptoms.25 In ALIF there is a nonunion rate which might be asymptomatic,25 but in case of a later established symptomatic anterior nonunion, supplementation with an instrumented posterior fusion does not always relieve the clinical symptoms. ALIF, as a standalone procedure, has a risk of anterior dislodgement in spondylolisthesis. Furthermore, the primary contact area of fusion cages is far less than the endplate surface area of the disc prosthesis.
Brantigan et al.26 reported 10-year results on a subgroup of an original US Food and Drug Administration trial, using carbon fiber posterior lumbar interbody fusion (PLIF) cages in conjunction with a posterior screw and plating system (360° fusion) with excellent clinical and radiological outcomes. McAfee et al.27 reported on 120 patients with spondylolisthesis, half of them with DSPL, who were treated with a 360-degree fusion through a single posterior approach with a 98% fusion rate, good radiological outcome, and few complications.
In a prospective study, Konno and Kikuchi9 compared surgical decompression, together with posterior dynamic Graf ligament stabilization, to decompression surgery alone. They found better clinical outcome in the Graf ligament group. Significant clinical improvement was confirmed in other studies using dynamic stabilization,2, 10–12 despite an increase in facet arthrosis.11 Posterior tension-band-like devices, in the absence of anterior support, should increase the load on the facet joints, and they are unable to significantly improve sagittal alignment. Taking this into consideration, the improvement in clinical outcome in these patients is remarkable. Recently McAfee et al. reported clinical improvement with a motionpreserving facet replacement system (TOPS).28
Despite the success with posterior motion-preserving techniques in DSPL, even in the absence of spondylolisthesis and kyphosis reduction,2, 10–12 DSPL over 3 mm is considered a contraindication for TDR.27 Nevertheless, objective confirmation of the outcome of TDR in DSPL is missing. Considerable reduction of the spondylolisthesis should be desirable in order to restore the normal 3-joint anatomy (disc and 2 facet joints) of the motion segment. This could not be achieved with posterior motion-preserving procedures.2, 10–12
The potential advantages of disc replacement with an unconstrained disc and non-rigidly held prosthetic endplates during insertion are, at least in theory, the following (see also Figure 1 and Hähnle et al.13:)
During the insertion process the prosthetic endplates can follow the shape of the bony endplates as they are able to pivot around the mechanism. The leading edge of a rectangular cage, or rigidly held disc prosthesis, is more likely to be impacted into the bony endplate, possibly resulting in endplate fracture and subsidence.
Once the Kineflex disc prosthesis is almost lying flush with the posterior vertebral body wall of the cephalad vertebra, the inferior endplate can be further advanced to facilitate reduction of the spondylolisthesis. As during this process part of the impact of the further advancement is absorbed in the prosthetic mechanism, the cephalad prosthetic endplate stays behind, avoiding protrusion of the superior prosthetic endplate into the spinal canal. With a cage or an unconstrained disc prosthesis, this manuever would easily result in impaction of the implant into the posterior part of the vertebral endplate of the cephalad vertebra (endplate fracture) or in protrusion of the implant into the spinal canal.
During mobilization of the patient the forces that could lead to expulsion of the inferior prosthetic endplate are at least partially dampened within the prosthetic mechanism, which allows translation but at the same time is recentering. Furthermore, flexion/extension motion through the operated segment does not lead to cyclical loss of contact (rocking) of the implant/bone surfaces and possible nonunion or nonintegration, as the contact is maintained by the adaptive movement of the prosthetic endplate.
With the Kineflex insertion technique used, we achieved excellent sagittal balance and slip correction in all patients. The continuous advancement of the inferior prosthetic endplate, after seating the prosthesis close to the posterior edge of the apical vertebral endplate, allowed additional reduction of the spondylolisthesis. The postoperatively high translational forces on the inferior prosthetic endplate could be counteracted with additional screw fixation used as a buttress. No postoperative hypermobility developed at the replaced levels. One reoperation was performed early after the index procedure with excellent clinical and radiological final outcome (Figure 4).
The most common level in DSPL is the L4-5 motion segment. At this level dislodgement of the implant would be of particular concern because of the proximity of important vascular structures. We would generally try to avoid anterior revision surgery at this level after 17–18 days and would rather wait past 3 months when the postoperative inflammation has completely settled. We therefore performed our anterior revision surgery for partial endplate extrusion early, after the first follow-up at 8 days postoperatively, despite good clinical relief of symptoms at that early stage (Figure 4).
The indications for TDR have hardly been modified since the onset of modern type TDR over 20 years ago.29 Only recently Siepe et al.30 published clinical outcome of TDR dependent on indications. There is a need for arthroplasty surgeons to publish results of off-label TDR procedures, in order to establish their validity for different indications and in order to learn from the experience of other surgeons.
CONCLUSION
This is a pilot study with significant limitations: Only 7 patients were involved with no control group, and the follow-up is short. Early results are promising, but because of the limitations, one has to be careful about the clinical outcome results. With the insertion technique of the tested device we achieved excellent sagittal balance and slip correction in all patients. No postoperative hypermobility developed at the replaced levels. The influence of improved sagittal spinal alignment on clinical outcome needs to be investigated in larger studies.
Acknowledgement
The authors thank Stephanie Hanekom and Aldorin Gehring for their enthusiastic support with patient management and follow-up.
Footnotes
Institutional Review Board approval was obtained from the University of the Witwatersrand Ethics Committee.
- Received December 16, 2007.
- Accepted April 21, 2008.
- Copyright SAS - Spine Arthroplasty Society 2008
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ulrich R. Hähnle, Ian R. Weinberg, and Malan de Villiers are co-developers of the Kineflex Disc Prosthesis and shareholders in Spinal Motion (Mountainview, California)