


ABSTRACT
Complications with cervical arthroplasty can be generalized to errors in patient selection or surgical technique. Patients with advanced spondylosis or osteophytic disease, severe facet arthropathy, osteoporosis, sagittal deformity, or preoperative instability are poor candidates for arthroplasty and are more prone to complications. Poor surgical technique can result in subsidence, expulsion, and kyphosis, and it can contribute to heterotopic ossification. Additionally, all of the inherent complications from an anterior cervical approach may occur with cervical artificial disc placement. This article will focus on the complications uniquely associated with cervical arthroplasty.
INTRODUCTION
Complications with cervical arthroplasty can be generalized to errors in patient selection or surgical technique. Complications can also be categorized by those associated, in general, with the anterior cervical approach and those specifically associated with cervical total disc replacement (cTDR). Patients with advanced spondylosis or osteophytic disease, severe facet arthropathy, significant bony foraminal stenosis, osteoporosis, sagittal deformity, or preoperative instability are poor candidates for arthroplasty and are more prone to complications. Poor surgical technique can result in subsidence, expulsion, residual radiculopathy, and kyphosis, and it can contribute to heterotopic ossification (HO). Additionally, all of the inherent complications from the anterior cervical approach may occur with cervical artificial disc placement. This article will focus on the complications uniquely associated with cervical arthroplasty and will compare complication rates of cTDR and anterior cervical discectomy and fusion (ACDF).
SUBSIDENCE, EXPULSION, DISLOCATION, AND OSTEOLYSIS
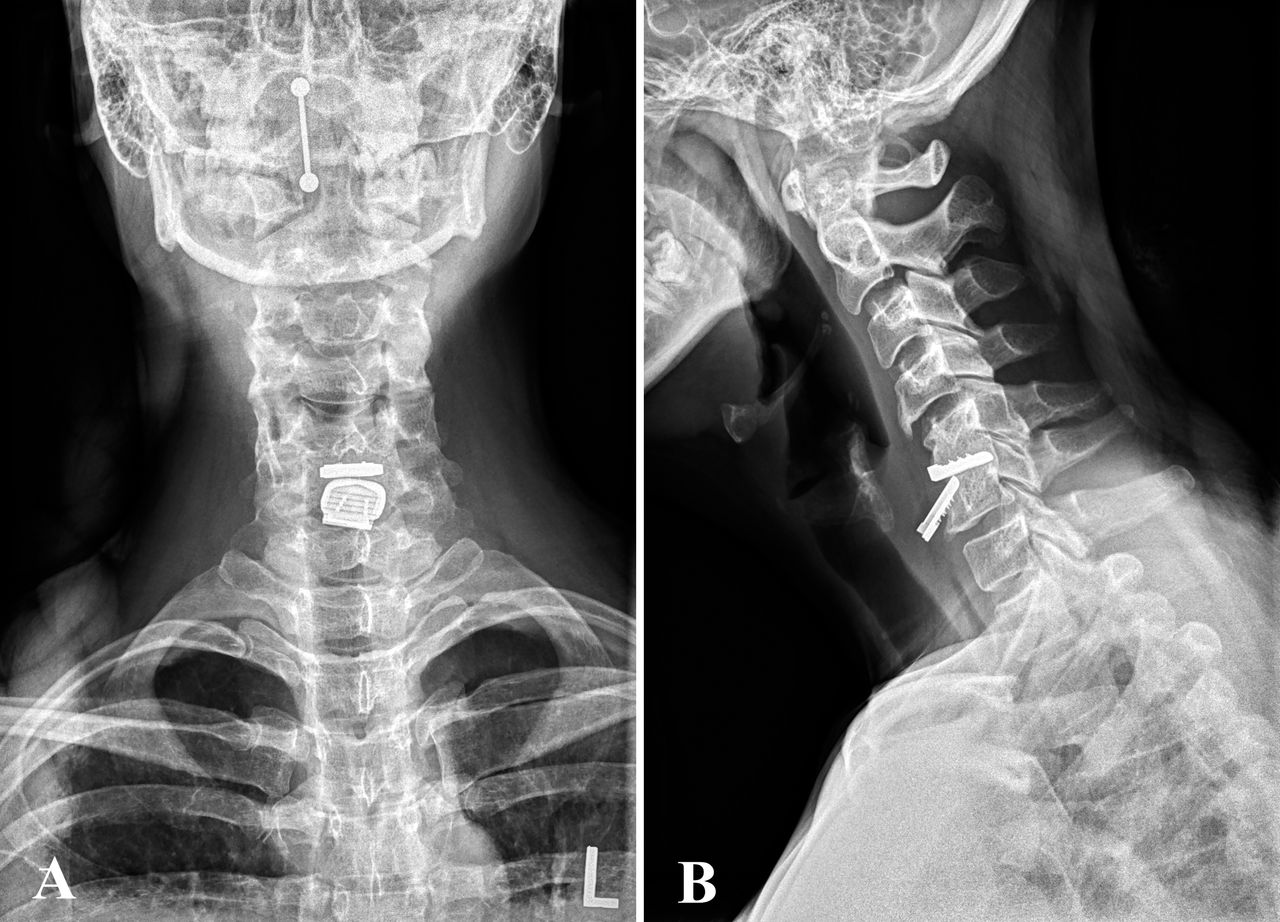
Complications related to surgical technique and patient selection include subsidence and device migration or dislocation, as well as residual radiculopathy. Subsidence can present as axial neck pain due to structural instability or can present as radiculopathy related to disc space collapse and resultant foraminal stenosis with nerve root compression. Subsidence has been reported in patients up to 4 years after artificial disc placement.1 Radiographic subsidence rates widely vary in the literature based on definition and length of follow-up, with rates ranging from 0% to 33.3%. But clinically significant subsidence is an uncommon complication, generally reported to be less than 3% in most large series.2–4 From a patient selection perspective, patients with underlying osteopenia (T-score <1.5) and osteoporosis (T-score < 2.5) or bone metabolism disorders are poor candidates for arthroplasty and have an increased risk of subsidence. From a surgical technique perspective, end plate violation during disc preparation and implant undersizing can create a predisposition to subsidence and displacement (Figure 1). Risk of subsidence can be minimized by avoiding drilling and preserving the vertebral end plates during disc preparation. Additionally, proper implant sizing can decrease the risk of subsidence and dislocation by avoiding implants with too large a height for the disc space (“overstuffing”) or implants that do not cover most of the end plates (“undersizing”). Residual radicular symptoms may be due to inadequate direct decompression secondary to osteophytic foraminal stenosis. Indirect foraminal decompression is typically less than what is accomplished with ACDF given the smaller implant size of cervical artificial discs (generally 4–6 mm) compared with interbody spacers (generally 6–9 mm). Osteolysis with lytic end plate destruction is an extremely rare complication of cervical arthroplasty likely related to wear debris and/or immunologic response to biomaterials. Theoretically, the risk would be increased with a metal-on-metal device.1
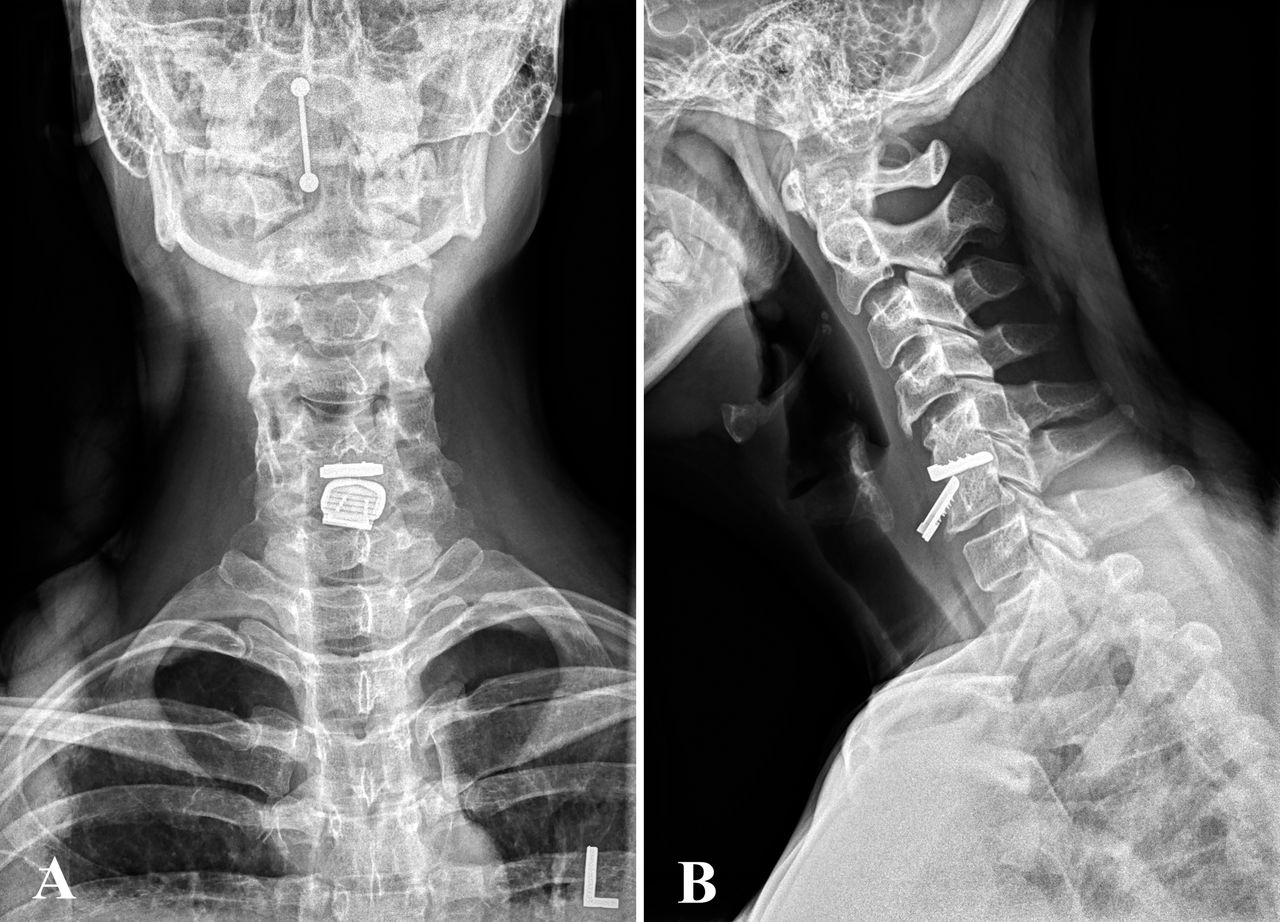
(A) Anteroposterior and (B) lateral radiographs of implant dislocation.
Subsidence, expulsion, dislocation, and osteolysis typically require anterior revision surgery with device removal and conversion to fusion, either ACDF or anterior corpectomy. Recurrent radiculopathy due to recurrent/residual foraminal stenosis can generally be revised with posterior minimally invasive laminoforaminotomy, also a motion-preserving and minimally invasive procedure.
HETEROTOPIC OSSIFICATION
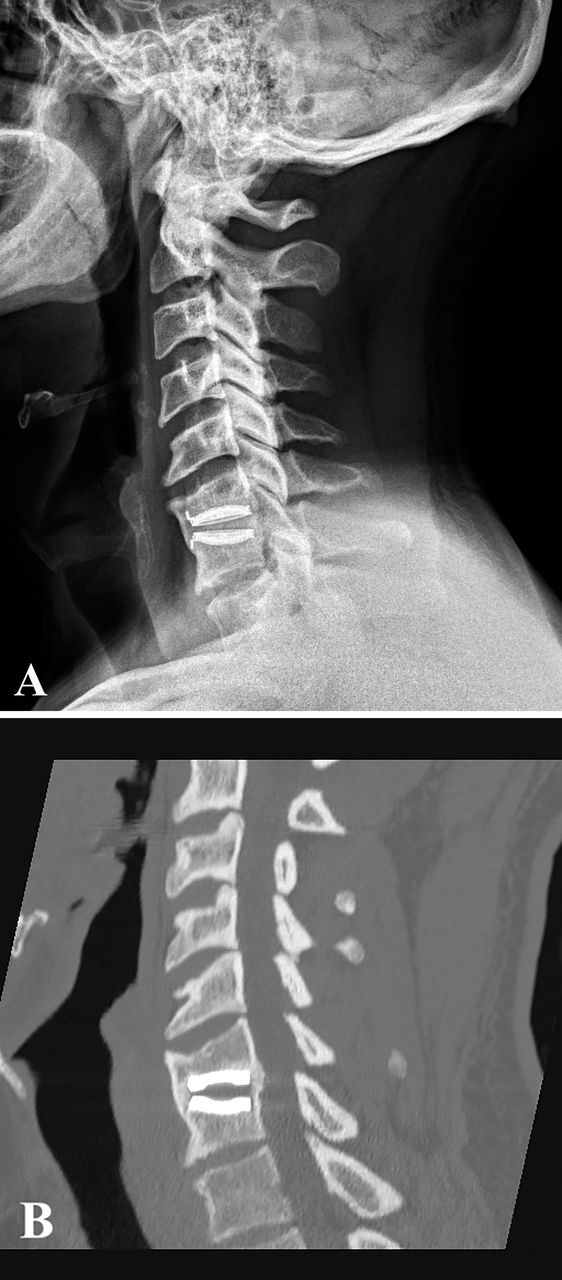
HO can be broadly defined as formation of bone outside the skeletal system. It is a phenomenon well documented after total hip and knee arthroplasty. Radiographically, HO can decrease the range of motion at the level of arthroplasty and can even result in a functional fusion due to bridging ossification, which is contrary to the fundamental aim of arthroplasty (Figure 2). Clinically, there appears to be no correlation between HO and worsened outcome. In fact, a recent study found that radiographically severe HO after CDA with the Prestige LP disc at 2 levels did not significantly affect efficacy or safety (severe AEs or secondary surgeries).5 HO after cervical arthroplasty was first reported by Parkinson and Sekhon.6 The incidence of HO is highly variable in the literature and is particularly affected by length of follow-up and definition of the degree of HO. McAfee et al7 developed a classification for HO after lumbar total disc replacement based on the Brooker et al8 classification of HO of the hip following hip replacement. They describe extent of HO from class 0 (no HO present) to class IV (inadvertent arthrodesis with <3° of motion in lateral flexion-extension radiographs). Mehren and colleagues9 described a cervical classification for HO similar to the McAfee classification system. For the cervical spine, HO is graded from 0 (no HO present) to grade IV (complete fusion without movement in flexion/extension; Table). Male sex and older age have been reported as risk factors for the development of HO.10 A recent meta-analysis by Kong et al11 reported the prevalence of HO within 1 to 2 years, 2 to 5 years, and 5 to 10 years to be 38.0%, 52.6%, and 53.6%, respectively. Further, the prevalence of severe HO (grade III or IV) was 10.9%, 22.2% and 47.5%, respectively. Intuitively, severe HO limits motion of the arthroplasty device and should be studied and minimized when possible. Patient selection may help minimize this complication because patients with advanced spondylosis and osteophytic disease will likely require more extensive bony preparation and drilling that may lead to HO. Excessive drilling results in bone debris and exposure of cancellous bone, which can predispose to HO. Proper surgical technique, including copiously irrigating during any drilling as well as application of bone wax to any exposed cancellous bone, may also aid in avoiding this complication. Furthermore, proper implant sizing with selection of an implant that has near complete end plate coverage may limit HO. Patients can be placed on nonsteroidal anti-inflammatory drugs during the early postoperative period (generally for 2 weeks), which also may reduce the risk of HO. Given the lack of clinical symptoms associated with HO, this “complication” does not typically require revision surgery.
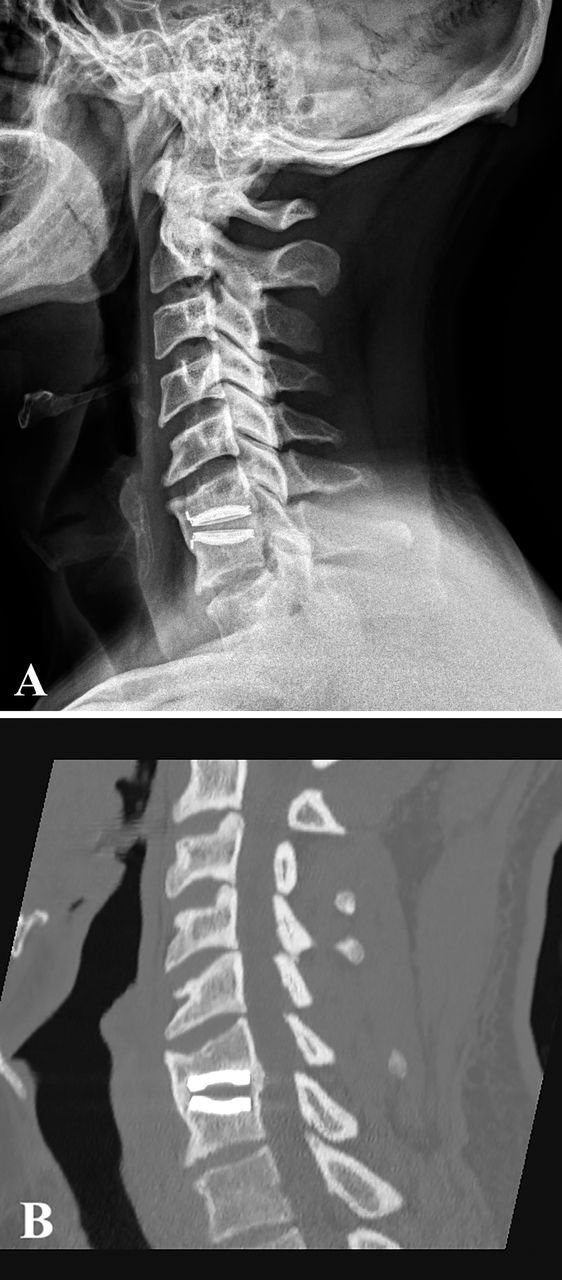
(A) Lateral radiograph and (B) sagittal computed tomography showing heterotopic ossification resulting in complete fusion.
Mehren classification of heterotopic ossification (HO).
ADJACENT SEGMENT DISEASE
Adjacent segment degeneration and disease following cervical spine surgery are controversial topics. Adjacent segment degeneration is defined as new radiographic changes at a spinal level immediately above or below a surgically treated level. When this adjacent segment degeneration results in clinical symptoms of radiculopathy, myelopathy, or mechanical instability, the appropriate terminology of adjacent segment disease applies. The most significant manifestation of adjacent segment disease results in adjacent segment reoperation. Motion-preserving devices were developed to mimic normal motion and theoretically reduce the stresses placed on adjacent segments compared with fusion, potentially resulting in decreased adjacent-level degeneration and reoperation. The development of adjacent segment disease is multifactorial and includes natural history of the underlying degenerative process, patient selection, type of procedure and implant (decompression alone vs fusion vs arthroplasty), surgical technique, and number of levels treated. Therefore, despite motion preservation, adjacent segment disease would still be expected to occur after arthroplasty, but theoretically at a reduced rate. Given the relatively low rates of adjacent segment reoperation rate following ACDF (<0.7% per year reported in the frequently cited Hilibrand et al12 study), in order to show a difference between arthrodesis and arthroplasty, a study would need to enroll a large number of patients (potentially thousands of patients), review a similarly large number of patients via meta-analysis, or continue to examine patients in long-term follow-up (5–10 years and beyond). Some limited early- and long-term studies support that arthroplasty may lead to less adjacent-level degeneration and disease.13,14
Cadaveric studies have shown that artificial disc placement results in reduced stress on adjacent segments compared with simulated fusion.15 The earliest report of adjacent segment degeneration after artificial disc replacement reported 5-year follow up for 18 patients with no evidence of adjacent segment degeneration.16 A meta-analysis of 3 randomized, multicenter, US Food and Drug Administration (FDA) Invesitigational Device Exemption (IDE) studies evaluated adjacent-level surgery at 24-month follow-up. There was a significantly lower rate of adjacent-level surgery favoring arthroplasty, with a relative risk of 0.460 (95% confidence interval, 0.229–0.926; P = .30; I2 =2.9%).17 A larger meta-analysis performed by Zhang and colleagues18 similarly found a lower rate of adjacent segment degeneration as well as reoperation favoring arthroplasty. Some studies with long-term follow-up have indicated that arthroplasty may result in decreased rates of adjacent-level degeneration and reoperation. Vaccaro et al3 reported a US FDA IDE trial of the SECURE-C device (Globus Medical, Audubon, PA) in 380 patients with 84-month follow-up. For adjacent segment reoperation rates, the incidence for cervical TDR was 4.2% compared with 16.0% in the ACDF group. Another 7-year study evaluated the efficacy of the Prestige ST Disc (Medtronic, Memphis, TN) reported for 541 patients, with an adjacent segment surgery rate of 4.6% in TDR compared with 11.9% in ACDF (P = .008).19
Long-term results for multilevel TDR have also shown that adjacent segment degeneration/disease may occur at a lesser rate compared with ACDF. Gao and colleagues20 reported 2 of 24 patients (8.3%) showing adjacent segment degeneration at 5-year follow-up after 2-level cervical arthroplasty. Radcliff et al21 reported on 5-year follow-up of 330 patients undergoing TDR and ACDF for 2-level TDR as part of the Mobi-C (Zimmer Biomet, Warsaw, IN) IDE trial. Adjacent segment degeneration was identified in 50.7% of the TDR group and 90.5% of the ACDF group (P < .0001). Further, adjacent segment requiring surgical intervention occurred in significantly fewer patients in the TDR group (3.1% vs 11.4%, P = .0004). Radcliff et al22 also reported on longer-term follow-up in this 2-level patient cohort and showed a statistically significant lower rate of subsequent surgeries at both index and adjacent levels in favor of arthroplasty at 7 years. Lanman and associates23 reported the results of the 2-level Prestige LP (Medtronic) IDE study comparing TDR (n = 209) vs ACDF (n = 188) at 7-year follow-up. They showed statistically significantly fewer second surgical procedures at the index level for TDR (4.2%) versus ACDF (14.7%) as well as a trend toward lower rates of adjacent-level surgery (6.5% vs 12.5%, respectively), which continues to diverge with longer follow-up.
Dysphagia
Dysphagia is a relatively common complication of anterior cervical surgery, although the etiology of this complication is poorly understood and is likely multifactorial. Some authors have postulated that dysphagia is an inevitable outcome of anterior cervical procedures, and not a complication.24 The reported rates of dysphagia are high immediately after surgery, with some studies reporting up to 71% in the immediate postoperative period.25 Predictors of dysphagia after anterior cervical surgery include increased age, duration of degenerative disease before surgery, increased operative time, blood loss, multilevel surgery, diabetes, and smoking, among other factors.26,27 Because most artificial discs are zero- or low-profile devices, some authors have theorized that cTDR placement would lead to lower rates of dysphagia. But most studies have shown no statistically significant difference in the rates of dysphagia between arthroplasty and ACDF,28 whereas others showed a lower incidence of dysphagia in patients undergoing arthroplasty.29–31 A meta-analysis performed by Findlay et al29 showed that ACDF was not superior to arthroplasty in any outcome category, including neck disability index, SF-36, range of motion, adjacent segment disease, patient satisfaction, dysphagia, and postoperative employment.
Generally accepted techniques of minimizing dysphagia with anterior cervical exposure should be employed, including meticulous hemostasis, retractor placement in the longus colli muscles with retractor release every 15 to 20 minutes, extensive muscle/soft tissue release during dissection, including resection of the omohyoid muscle if necessary, release of the endotracheal cuff following retractor placement, and maintenance of superficial temporal artery flow following retraction as well as the administration of perioperative corticosteroids.
Vascular Complications and Infection
Rates of adverse vascular events and surgical site infection are generally low in anterior cervical surgery.2 In one randomized control trial of 541 patients undergoing either ACDF or arthroplasty for single-level degenerative disc disease, the reported mean blood loss was 57.5 and 60.1 mL, respectively, with no statistically significant difference.19 This same study reported a total of 2 intraoperative vascular injuries resulting in hematoma formation in the arthroplasty group, and 1 intraoperative vascular injury resulting in venous bleeding in the fusion group. Of the 541 patients in this study, none developed a surgical site infection. Other studies have demonstrated very low rates of adverse vascular events and infections in patients undergoing arthroplasty or ACDF. In an RCT comparing the Prestige LP artificial disc to ACDF, Lanman et al23 reported no significant difference in vascular events between arthroplasty and ACDF (0.5% and 0%, respectively). In a study of 24 patients undergoing arthroplasty with the Prestige LP for contiguous 2-level cervical disease by Gao et al,20 no patients developed infection or local hematoma. Other studies comparing ACDF and arthroplasty routinely report no superficial or deep wound infections postoperatively.4,14
CONCLUSIONS
Complications associated with the anterior cervical approach are not common and are similar between ACDF and cTDR. Dysphagia is the most common complication, but arthroplasty is not associated with increased risk when compared with ACDF. Vascular complications and infection are rare, and rates are also not significantly different between ACDF and arthroplasty.
Complications uniquely associated with cervical artificial disc placement include subsidence, displacement, and osteolysis, as well as HO. These complications are uncommon and can be somewhat mitigated by proper patient selection and attention to surgical technique. Cervical arthroplasty is ideally indicated in patients with 1- and 2-level cervical soft disc disease with mild spondylosis without significant facet disease or osteoporosis. Surgical technique varies somewhat with various implants, but it generally includes accurate midline verification, symmetrical decompression with proximal uncovertebral joint resection, minimal drilling, and respect of the bony end plates, as well as proper implant sizing and placement in close proximity to the disc's natural center of rotation. Failed cervical disc arthroplasty revision is typically straightforward, and the approach typically depends on the mode of failure.
Adjacent segment disease is a multifactorial process that can be seen following arthroplasty or arthrodesis. It has been biomechanically established that artificial disc placement results in less adjacent-level stress compared with fusion. The clinical ramifications of those decreased stresses remains debatable, although some meta-analyses and studies with long-term follow-up indicate that cervical arthroplasty may result in decreased adjacent segment degeneration and disease.
Footnotes
Disclosures and COI: Dr Coric is a consultant for or receives royalties from Globus Medical, Spine Wave, Medtronic, Stryker Spine, and Integrity Implants; receives royalties from RTI Surgical; is a consultant for or holds stock in Premia Spine; and is on the Spine Advisory Board for United Healthcare.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}