


Abstract
Background Harrington instrumentation for adolescent idiopathic scoliosis (AIS) was revolutionary and allowed patients to mobilize faster as compared with patients treated with uninstrumented fusion. However, Harrington instrumentation provided correction of the deformity in 1 plane, resulting in limited sagittal plane control. Patients who received these 2 surgeries are aging, and to date, ultralong follow-up of these patients has not been reported.
Objective The purpose of this study was to evaluate long-term patient-reported outcomes and radiographic parameters after Harrington nonsegmental distraction instrumentation vs uninstrumented fusion in the treatment of AIS.
Methods Fourteen adult patients with AIS who were previously instrumented (n = 7) or uninstrumented (n = 7) were identified. Recent x-ray image measurements such as pelvic incidence (PI), sagittal vertical axis (SVA), pelvic tilt (PT), lumbar lordosis (LL), and pelvic incidence minus lumbar lordosis (PI-LL) were used to analyze deformities. Scoliosis Research Society-7 (SRS-7), Neck Disability Index (NDI), and Oswestry Disability Index (ODI) were used to evaluate patient-reported outcomes. Complications and rates of revision surgery were also evaluated.
Results The mean age was 67.1 ± 5 years in the instrumented group and 64.1 ± 9 years in the uninstrumented group. There were no significant differences between instrumented and uninstrumented in SRS-7 (23.4 ± 2.9 vs 23.6 ± 2.6, P = 0.93), NDI (5.7 ± 4.5 vs 10.6 ± 4.5, P = 0.08), and ODI (9.7 ± 13.7 vs 9.4 ± 8.7, P = 0.99). Radiographic measurements of instrumented vs uninstrumented resulted in comparable PT (24.0 ± 7.9 vs 30.5 ± 4.7, P = 0.09), PI (61.3 ± 16.9 vs 67.2 ± 9.5, P = 0.47), LL (34.9 ± 14.4 vs 42.8 ± 11.0, P = 0.29), PI-LL (26.4 ± 25.1 vs 24.3 ± 10.4, P = 0.43), and SVA (38.1 ± 30.1 vs 52.3 ± 21.6, P = 0.37). There were 2 patients in the instrumented group who developed adjacent segment disease that required operative intervention compared with none in the uninstrumented group (P = 0.46).
Conclusion In long-term follow-up of instrumented and uninstrumented fusion, patients had similar patient-reported outcomes and radiographic parameters, although the instrumented cohort had higher rates of adjacent segment disease.
Level of Evidence 4.
- nonsegmental distraction rod instrumentation
- scoliosis surgery
- spinal fusion
- deformity
- Harrington
- surgical outcome
INTRODUCTION
Adolescent idiopathic scoliosis (AIS) is the most common 3-dimensional deformity of the spine and affects 1% to 2% of the population.1–3 Prior to the introduction of spinal instrumentation, uninstrumented in situ fusions were performed, often in conjunction with casting, to halt curve progression, albeit with high complication rates.4 Louis Goldstein, a visionary leader in spinal deformity surgery, was at the forefront of both uninstrumented and instrumented treatment of AIS. He reported the use of fresh autogenous iliac bone grafts and turnbuckle casts in AIS treatment with lower incidence of pseudarthrosis and excellent outcomes.5,6 He was also an early adopter of Paul Harrington’s novel internal fixation method for treatment of scoliosis.7,8 The Harrington nonsegmental distraction instrumentation system, introduced in the 1960s, was the first widely used internal fixation system for the correction of idiopathic scoliosis when combined with a spinal arthrodesis.9 Harrington instrumentation had many advantages, such as minimal invasion of the spinal canal, low incidence of neurological complications, and earlier return to ambulation.10 It also had documented disadvantages and complications, such as limited sagittal plane control, pseudarthrosis, adjacent segment disease, and the crankshaft phenomenon.11,12 Harrington distraction rods were significant in enabling an operative correction of scoliosis, and posterior spinal arthrodesis and instrumentation remain a common form of operative treatment for AIS.13 Previous follow-up studies of Harrington instrumentation and fusion have found that radiologic correction in the coronal plane may be maintained after 5 to 12 years.13–17 Additionally, patient-reported outcomes following Harrington instrumentation are well studied.18–21
To our knowledge, there have been no ultralong (>45 years) follow-up studies comparing Harrington instrumentation vs uninstrumented fusion with fresh autogenous iliac bone graft and turnbuckle plaster cast correction for AIS. As patients who underwent these procedures age, it is important for surgeons to better understand long-term outcomes of these procedures that are less commonly performed today. Consequently, the objectives of this case-control study were as follows: (1) to compare patient-reported outcomes such as Neck Disability Index (NDI), Oswestry Disability Index (ODI), and Scoliosis Research Society-7 (SRS-7) between the Harrington instrumentation and uninstrumented fusion patients and ( 2) to compare radiographic parameters such as pelvic tilt (PT), pelvic incidence (PI), lumbar lordosis (LL), pelvic incidence minus lumbar lordosis (PI-LL), and sagittal vertical axis (SVA) between the Harrington instrumentation and uninstrumented fusion patients.
METHODS
This study was approved by the institutional review board. Patients at a single institution with a history of AIS treated with either an uninstrumented fusion or Harrington instrumentation with ultralong follow-up defined as a minimum 45 years follow-up were identified. Those in the uninstrumented fusion group had an in situ posterior spinal fusion with fresh autogenous iliac bone grafts as well as preoperative and postoperative casting. Patients in the Harrington instrumentation group had a posterior instrumented fusion along with postoperative casting. Patients who had additional unrelated spinal surgeries, hemivertebrae resections, or osteotomies were excluded.
Patients were identified from the institutional database of spine procedures, were contacted via mail to participate in the study, and, after providing consent, were asked to undergo scoliosis radiographs. Those who responded, completed all questionnaires, and underwent recent radiographic studies were included. Those who were unable to obtain recent radiographs, deceased, or did not complete patient-reported questionnaires were excluded. Patient-reported outcomes survey questionnaires that were administered included the NDI, ODI, and SRS-7. All enrolled patients underwent scoliosis anterior-posterior and lateral radiographic examinations of the spine. Medical records were reviewed for patient demographics such as age, sex, date of surgery, type of surgery, and complications or revision surgeries.
The enrollment radiographs were evaluated for pelvic and sagittal parameters using PT, PI, LL, PI-LL, and SVA measurements. Patient demographics were compared between the Harrington instrumentation and uninstrumented groups to assess potential group differences at baseline. Patient-reported outcome measures and radiographic parameters were also compared to evaluate for between-group differences.
Statistical Analysis
Statistical analysis was performed by calculating and performing independent t tests to compare differences between 2 groups. P values were obtained from 2-tailed distributions with the alpha level set at 0.05. Descriptive statistics of mean, SD (±), and range were calculated and reported along with the tests of variance.
RESULTS
Demographics
A total of 14 patients were included (Table 1). Seven patients had Harrington nonsegmental distraction instrumentation and were in the instrumented group, and 7 patients had spinal fusion for AIS without instrumentation and were in the uninstrumented group. The instrumented group compared with the uninstrumented group was not significantly different in terms of mean age (67.1 ± 5 vs 64.1 ± 9 years, P = 0.47) and female sex (6/7 vs 6/7, P = 1). The final follow-up and years since surgery were also similar, with a mean of 51.7 ± 3.7 years (range, 45–57 years) in the instrumented group compared with a mean of 52.2 ± 6.1 years (range, 45–59 years) in the uninstrumented group (P = 0.89).
Patient characteristics.
Patient-Reported Outcomes (Figure 1)

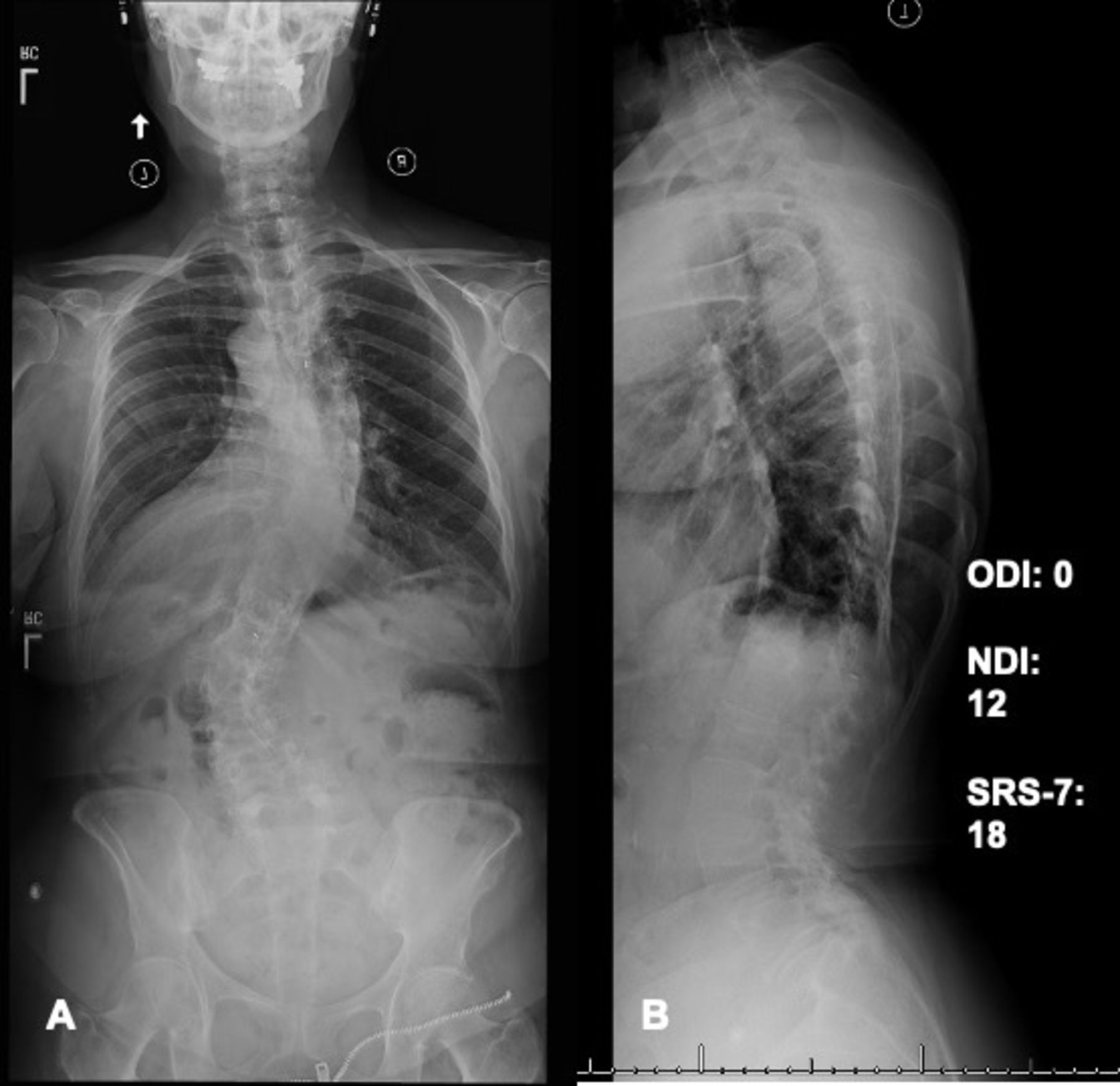
(A) Anterior-posterior and (B) lateral scoliosis radiographs of a 73-y-old woman 60 y after uninstrumented fusion for adolescent idiopathic scoliosis. Patient-reported outcomes demonstrated minimal pain/disability. NDI, Neck Disability Index; ODI, Oswestry Disability Index; SRS-7, Scoliosis Research Society-7.
There were no significant differences in the patient-reported outcome measures for the instrumented group compared with the uninstrumented group (Table 2). The instrumented group reported a mean SRS-7 score of 23.4 ± 2.9 (range, 19–27), while the uninstrumented group reported a mean SRS-7 score of 23.6 ± 2.6 (range, 18–27), P = 0.93. Specifically, for the pain portion of the SRS-7, 43% (n = 3) of the instrumented patients reported “moderate pain” in the past 6 months with the rest reporting mild to no pain compared with 14% (n = 1) in the uninstrumented group with the rest reporting mild to no pain. Mean NDI scores for the instrumented and uninstrumented groups were 5.7 ± 4.5 (range, 0–10) and 10.6 ± 4.5 (range, 2–18), respectively (P = 0.08). Mean ODI scores were comparable for the instrumented and uninstrumented groups, at 9.7 ± 13.7 (range, 0–34) and 9.4 ± 8.7 (0–22), respectively (P = 0.97). In the instrumented group, 71% (n = 5) were in the “minimal disability” ODI category and 29% (n = 2) were in the “moderate disability” ODI category. In the uninstrumented group, 86% (n = 6) were in the “minimal disability” ODI category, and 14% (n = 1) were in the “moderate disability” ODI category.
Patient-reported outcomes and radiographic parameter results examined in this study.
Radiographic Parameters (Figure 2)
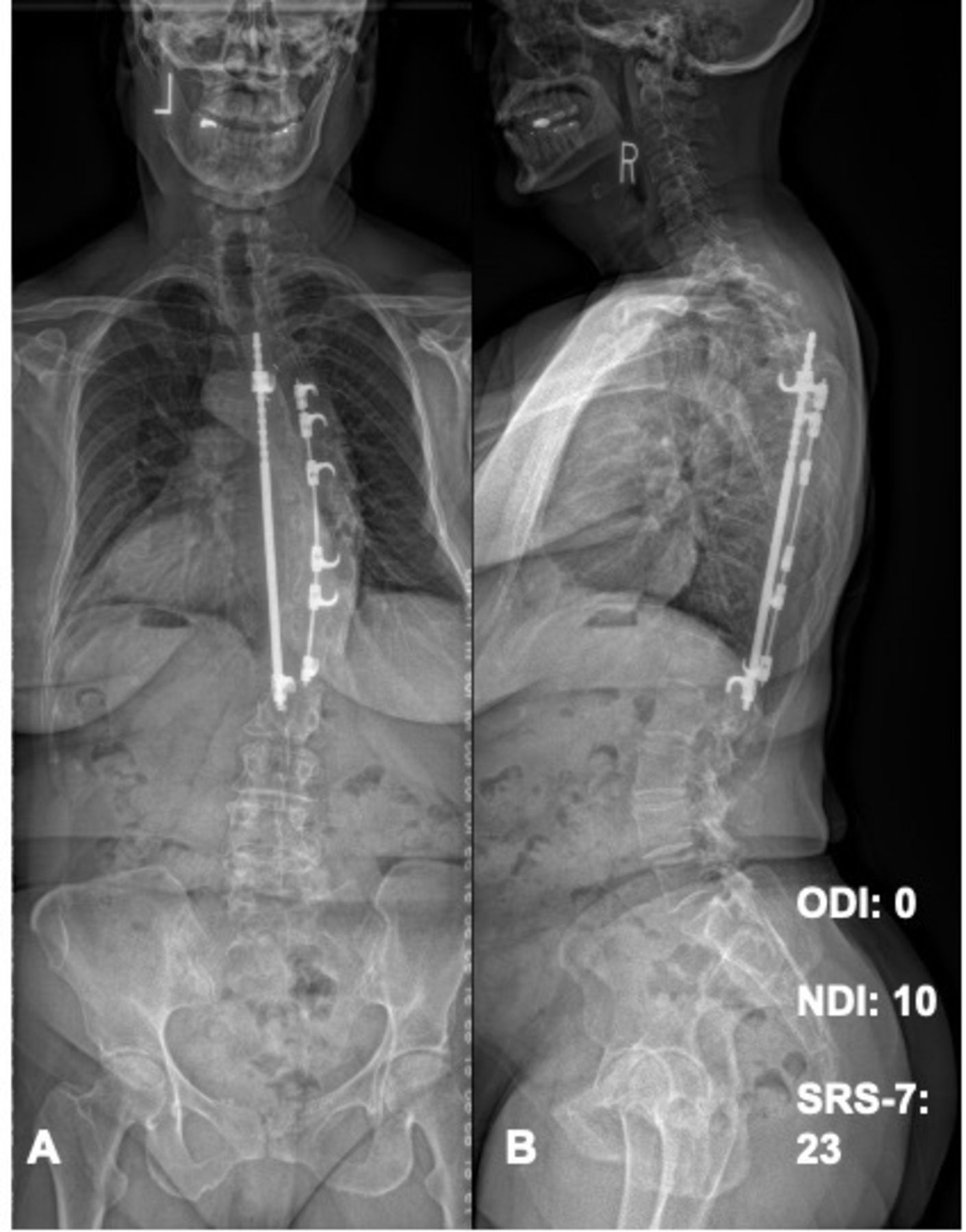
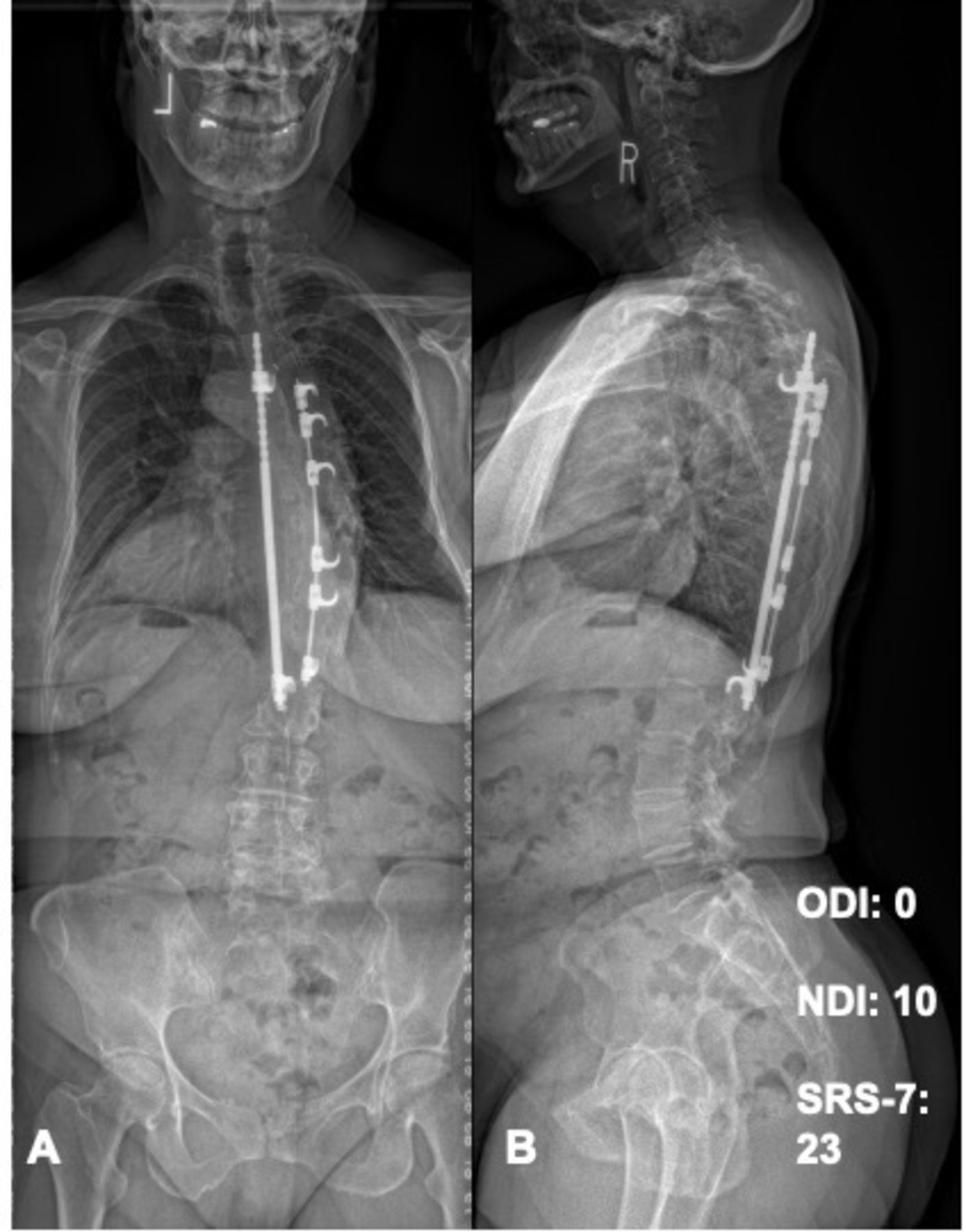
(A) Anterior-posterior and (B) lateral scoliosis radiographs of a 69-y-old woman 57 y after instrumented fusion for adolescent idiopathic scoliosis. Patient-reported outcomes demonstrated minimal pain/disability. NDI, Neck Disability Index; ODI, Oswestry Disability Index; SRS-7, Scoliosis Research Society-7.
Final radiographic parameters measured were also not significantly different between the 2 groups (Table 2). PT tended to be lower in the instrumented group at 24.0° ± 7.9° compared with 30.5° ± 4.7° (P = 0.09). PI (61.3° ± 16.9° vs 67.2° ± 9.5°, P = 0.47), LL (34.9° ± 14.4° vs 42.8° ± 11.0°, P = 0.29), PI-LL (26.4° ± 25.1° vs 24.3° ± 10.4°, P = 0.43), and SVA (38.1 ± 30.1 vs 52.3 ± 21.6 mm, P = 0.37) were comparable between the instrumented and uninstrumented groups, respectively.
Complications
Two patients in the instrumented group developed lumbar adjacent segment disease and required operative intervention. No patients in the uninstrumented group developed complications or required further surgical intervention. These complication rates were not significantly different (P = 0.46).
DISCUSSION
This is the first ultralong follow-up (>45 years) comparative outcomes study of patients with AIS treated with either Harrington instrumentation or uninstrumented fusion as described by Dr. Goldstein.5 Most studies identified in the literature evaluating outcomes after Harrington instrumentation have reported up to only 2 decades of follow-up data.14,15,18,22,23 In the past 5 decades, much has changed in treatment and management of AIS. While Harrington rod instrumentation and uninstrumented fusion have largely been replaced by other surgical instrumentation and techniques, it is important for surgeons to understand long-term outcomes and prognoses as patients who underwent these procedures age and require more complex management considerations.
In an average 21-year follow-up of AIS patients treated using Harrington instrumentation, Helenius et al reported 13% of patients having low back pain often or very often at rest according to the SRS questionnaire.23 Another 23-year follow-up by Mariconda et al found no significant differences in the SRS-7 scores between those with Harrington instrumentation and the general population without AIS, concluding that the procedure may maintain a long-lasting, high degree of patient-reported satisfaction.18 The findings from the present study are consistent with these 2 studies, with 3 out of 7 patients in the instrumented group reporting “moderate pain” in the SRS questionnaire and 1 out of 7 patients in the uninstrumented group reporting “moderate pain” in the SRS questionnaire. No patients reported severe pain. Furthermore, based on the ODI, patients in the present study also reported low disability scores, consistent with the long-term patient-reported satisfaction reported by the other studies.
Long-term complication rates were similar to previously reported studies. Two patients in the instrumented group had adjacent segment disease while no patients in the uninstrumented group reported any complications. Simony et al followed 159 AIS patients treated with Boston brace or Harrington instrumentation fusion over 22 years and reported 24% of fusion patients with distal segment degeneration and 3.2% requiring additional surgery, consistent with the 29% adjacent segment disease found in the present study.22 While radiographic parameters were also not significantly different, the instrumented group tended to show more flattening of thoracic and lumbar curvatures. This is consistent with a 1983 study by Cochran et al with 22-year follow-up of patients undergoing Harrington instrumentation. About 52% of patients had flattened or kyphotic cervical spines, nonsignificant flattening of the thoracic kyphosis, and significant lowering of the lumbar lordosis.14
The study was limited by a small sample size due to the challenges associated with identifying and enrolling cases and controls that underwent these procedures more than 45 years ago at a single institution. Furthermore, selection bias must be considered, as long-term follow-up may select for patients who generally have good outcomes. Another limitation was the absence of any baseline or previous radiographs to assess changes over time. The records of the surgeries and radiographs from the 1960s and 1970s when these operations took place were not archived within the electronic health record. Future studies may consider identifying a larger sample size of patients with uninstrumented fusion from multiple centers as well as those surgically managed with Harrington instrumentation with similar length of follow-up in order to increase the power of the comparative analyses. Further studies on complication rates such as adjacent segment disease of all surgical management options for AIS with or without instrumentation may further inform clinical decision-making and help guide surgical management.
CONCLUSION
In the long-term follow-up of AIS patients who underwent Harrington instrumentation and uninstrumented fusion with fresh autogenous iliac bone graft and turnbuckle plaster casting greater than 45 years prior, patient-reported outcomes and radiographic parameters did not show significant differences in results between the 2 groups. While complication rates were not significantly different, the instrumented group reported higher rates of adjacent segment disease compared with the uninstrumented group.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Paul Rubery declares a grant from AO Spine. James Sanders declares grants from SRS and POSNA and consulting fees from Orthopaediatric. Emmanuel Menga declares a grant from Globus Medical, royalties from Evolution Spine, and consulting fees from Globus Medical. Addisu Mesfin declares grants from Globus Medical and AO Spine and consulting fees from Medtronic and DePuy Synthes. The remaining authors have no disclosures.
Ethics Approval Approval was obtained from the ethics committee of the University of Rochester Medical Center. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.