


Abstract
Introduction Lumbosacral traumatic spondylolisthesis L5–S1 is a rare clinical entity that compromises the stability of the L5 vertebra by displacing it anteriorly, laterally, or posteriorly on the S1 vertebral body secondary to osteotendinous and/or articular compromise of this segment due to trauma. This pathology is difficult to classify and manage; although surgical management remains the gold standard, short- and long-term results in the literature are scarce and highly variable.
Patient Presentation We present the case of a 53-year-old patient with lumbar trauma due to a free fall from a height of 6 meters. The fall resulted in cauda equina syndrome secondary to lumbosacral traumatic spondylolisthesis L5-S1, which required immediate surgical management.
Intervention and Outcome For surgical management, we used a posterior approach for L5–S1 transpedicular screw fixation, spinal decompression, bilateral root foraminotomy of L5, and L5–S1 open transforaminal lumbar interbody fusion with open reduction. After the operation, the patient reported immediate improvement of postoperative lower extremities pain and was discharged on the third postoperative day after achieving clinical improvement with physical therapy and bladder rehabilitation exercises.
Conclusion Lumbosacral traumatic spondylolisthesis L5–S1 is an unusual pathology that requires further study as there is currently no standardized classification. Surgical management is the gold standard and includes open reduction with short transpedicular screw fixation in segment L5–S1 and other surgical interventions such as extension to the pelvis with iliac screws, screws to the L4 vertebral body, and use of lumbar interbody fusion cages.
Level of Evidence 4.
INTRODUCTION
Lumbar spondylolisthesis is a common entity among the pathologies of the lumbar spine.1 It is classified according to the Wiltse classification2 as dysplastic, isthmic, degenerative, traumatic, or pathological.1,3 Lumbosacral traumatic spondylolisthesis at L5–S1 is the most unusual presentation.4,5
L5–S1 lumbosacral traumatic spondylolisthesis is a rare clinical entity with few cases described since it was first reported in 1940 by Sir Watson Jones.4,6 In such cases, secondary to a lumbosacral trauma, there is joint and/or ligament compromise of the facet joint of the L5–S1 vertebral segment, which can be unilateral or bilateral, causing an anterior, posterior, and lateral displacement of the L5 vertebral body on S1.7–9
Traumatic lumbar spondylolisthesis is an entity more frequently associated with males; it typically occurs between the ages of 35 and 55 years.10 The majority of presentations (53%) result from accidents or high-energy traumas (eg, traffic accidents) in the L5–S1 segment. Other causes include crush injuries (36%) and free fall (11%),5 which generate flexion/extension, rotation, and translation forces at this level.11,12 In addition, low back pain is the main presenting symptom, reported by about 82% of patients, followed by neurological deficits in 50% and cauda equina syndrome in 10%.5
Different classifications have been proposed; however, this pathology is complex, and there is no classification that standardizes its management.12,13 A large number of authors agree on the lack of literature found on this pathology, and a limited group of case reports and case series can be found.1,4,5,8
We present the case of a patient with lumbosacral traumatic spondylolisthesis L5 to S1 and classify and define the patient’s clinical and surgical management.
CASE REPORT
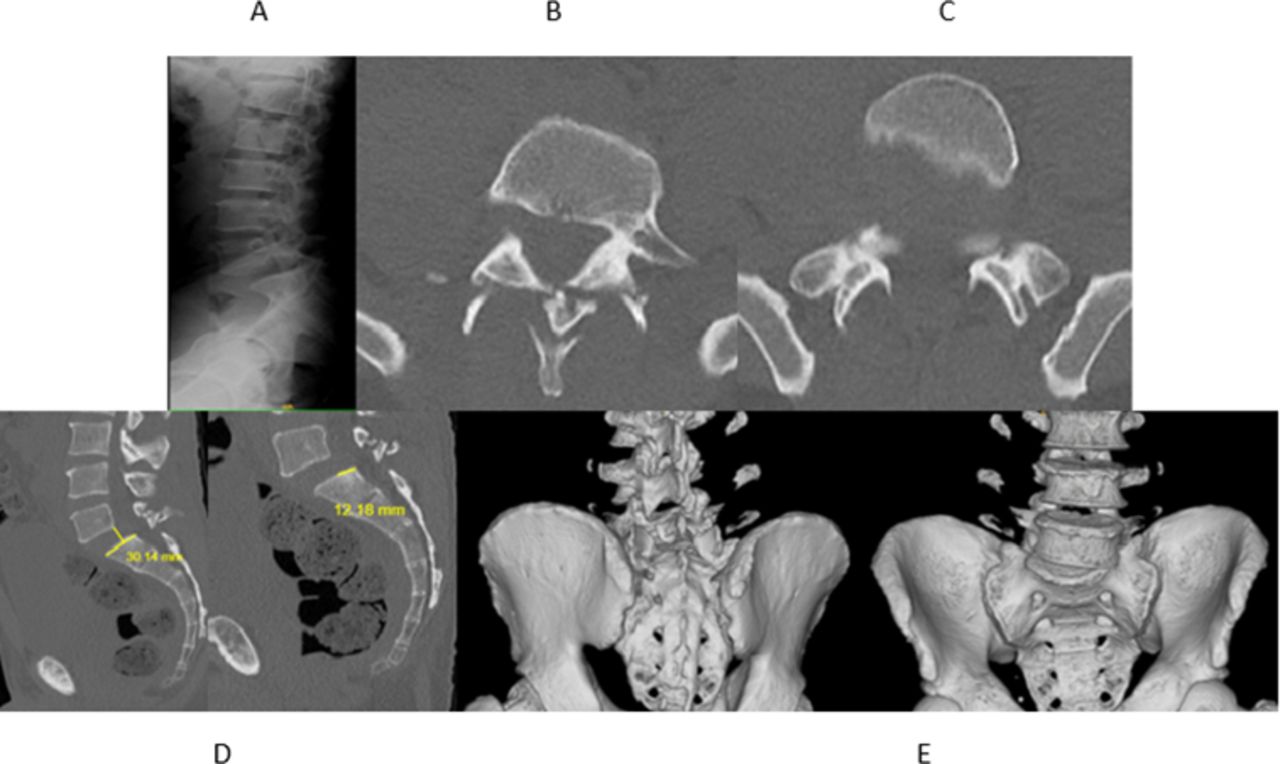
A 53-year-old male patient consulted the emergency department 72 hours after incurring trauma to the lumbar region after falling from a height of approximately 6 meters. After the incident, the patient had a subsequent inability to walk due to pain and loss of strength in the lower limbs. The patient presented with cauda equina syndrome characterized by sphincter involvement, muscle strength in myotomes L5 and S1 of 3/5 of the lower limbs, and saddle anesthesia in the perianal region. Imaging studies were ordered, including lateral x-ray imaging (Figure 1A), computed tomography (CT) axial and sagittal slices (Figure 1B, C and D), 3-dimensional reconstruction (Figure 1E), and magnetic resonance imaging (MRI) of the lumbosacral spine (Figure 2). Images revealed a traumatic spondylolisthesis at L5–S1 with disruption of spinal canal, lesion of intervertebral ligaments, and soft tissue involvement. Using the classification of Vialle et al (Table), the spondylolisthesis was classifyied as Type III-B.

(A) Lateral lumbosacral radiograph showing spondylolisthesis at L5–S1. (B and C) Lumbosacral computed tomography (CT) axial slice showing a fracture of the facet joint L5 and S1 with translation of L5 on S1. (D) Sagittal lumbosacral axial CT showing translation of the vertebral body L5 on S1 with measurement of the translation. (E) Axial CT with 3-dimensional reconstruction of the lumbosacral spine showing the facet joint fractures and rotation mechanism in the L5–S1 segment.

Nuclear magnetic resonance imaging for simple lumbosacral spine showing ligamentous and disc compromise of the L5–S1 segment with invasion of the spinal canal.
Description made by the authors based on the illustrations of Vialle et al.9
For surgical management, we used a posterior approach for L5–S1 transpedicular screw fixation, spinal decompression, bilateral root foraminotomy of L5, and L5–S1 open transforaminal lumbar interbody fusion with open reduction (Figure 3).

Axial computed tomography of the lumbosacral spine with 3-dimensional reconstruction. Arthordesis and instrumentation of the L5–S1 segment with placement of a transforaminal cage (transforaminal lumbar interbody fusion) is indentified with axial and sagittal slices, which show reduction of anterior translation and rotation of the vertebral body of L5.
After the operation, the patient reported an immediate improvement of lower extremities pain; discharge was indicated on the third postoperative day due to his clinical improvement with physical therapy and bladder rehabilitation exercises with intermittent catheterization. He was reassessed at 15 days with the improvement of muscle strength in myotome L5 and S1 of 4/5 without the presence of pain and improvement of sphincter compromise due to normal retention of bladder function. At 6-month follow-up, the patient had a favorable clinical evolution; neurological examination revealed recovery of paresis in the left lower limb and absence of pain in the surgical area and lower extremities.
DISCUSSION
Lumbosacral traumatic spondylolisthesis at L5–S1 is the anterior or posterior displacement of the L5 vertebra on the S1 vertebra.1 It is mainly produced by high-energy trauma7–14 in which traffic accidents, free fall, and crush injuries predominate;7–9,14 lumbosacral traumatic spondylolisthesis at L5–S1 is possible, but it is a rare entity and comprises only 1% of spinal fractures.12
The mechanisms of hyperextension, compression, lateral hyperflexion, and rotation are the cause of anterior dislocation, with the L5 to S1 segment being most frequently affected.7,12 On the other hand, a combination of anteriorly directed shear forces with hyperextension due to high-energy impact against the posterior pelvis will result in posterior dislocation.7
The clinical presentation varies depending on the location of the pain; however, the physical examination must be thorough because patients may present bruises on the flanks, abrasions, palpable scaling of the spinous processes,12 and neurological compromise evidenced by hypoesthesia in the limbs, lower legs, radicular pain, intestinal, and/or bladder dysfunction or sexual dysfunction; these symptoms are indicators of severity of the injury.11–13
Within the neurological lesions, there is the cauda equina syndrome8,12,13 or the disruption of the lumbosacral plexus,12 which generates a surgical emergency in this pathology, and the patient must be taken to decompression of the spinal canal and nerves immediately.
In the lumbosacral spine radiograph in anteroposterior projection, obliquity of the L5 vertebra, fractures of the transverse processes, widening of the paravertebral soft tissue lines, widening of the interpeduncular distance, or rotational deformity of the spinous processes can be observed; note increased interspinous distance, lumbosacral kyphosis, anterior disc height narrowing, anterior or posterior subluxation of the L5-S1 segment, or amplification of lumbar lordosis.7,12
For imaging diagnosis, x-ray imaging of the spine can be performed in anteroposterior, lateral, and dynamic projections when the clinical impairment permits the mobilization of the patient, CT axial and sagittal slices with 3-dimensional reconstruction, and MRI.7,11,14
The axial CT associated with 3-dimensional reconstruction allows the visualization of injuries of the posterior elements or of fractured facets with the displacement of the vertebra or the sacrum, as well as the “naked facet” sign, which can be observed in the axial plane and is presented by the overlapping of facets of L5 on those of S1.12
MRI of the lumbosacral spine allows us to visualize the involvement of soft tissues and, in cases where there is disc disruption or neural foramen involvement,9 provide more information than what is found in tomography studies. MRI also helps surgeons establish the best surgical plan for patients with neural compression and define which approach should be performed on the patient.12
With the advent of imaging studies, since 1960, it has been possible to create classifications for this pathology, and different classifications have emerged, but due to its difficulty in grouping this type of injury, there are only 2 classifications at present: (1) the classification proposed by Aihara et al in 199815 and the classification proposed by Vialle et al in 2007.9 The latter is based on injury patterns and lumbosacral dislocations (Table).9
For patient management, there are 2 options: surgical and nonsurgical management. Nonsurgical management consists of conservative measures such as closed reduction, traction, and corset immobilization. In the long term, these measures do not generate benefits in the patient’s clinical status, and later, patients typically require surgical management with larger instrumentation due to greater instability or kyphotic compromise.12,14 In surgical management, the gold standard for the management of lumbosacral traumatic spondylolisthesis is open reduction and internal fixation with transpedicular screws to prevent the progression of the lesion, instability, and neurological complications.7–10,14
The posterior approach management is the most recommended due to the fact that this approach has fewer intraoperative complications and requires less surgical time when compared with anterior approach management. However, different studies and reviews of the literature have been described in which, depending on the compromise or extrusion of the intervertebral disc, lumbosacral interbody fusion, duraplasty, and decompression of the lumbar canal are required, performing anterior and posterior surgery to provide greater stability and correction of the injury.8,9,12
CONCLUSION
Lumbosacral traumatic spondylolisthesis L5–S1 is an unusual pathology that requires further study because there is currently no standardized classification. Surgical management is the gold standard with short transpedicular screw fixation in segment L5–S1 and other surgical management, such as extension to the pelvis with iliac screws, screws to the L4 vertebral body, and use of lumbar interbody fusion cages.
Acknowledgment
Thanks to Diego Alejandro Muñoz Montoya for his help and support.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures The authors have nothing to report.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.