


Abstract
Background Currently, there are no studies in the literature that specifically compare stand-alone anterior lumbar interbody fusion (ALIF), 360° ALIF, or arthroplasty in patients with recurrent lumbar disc herniation presenting with signs of instability. Thus, the authors sought to fill this knowledge gap by comparing intraoperative and short-term postoperative outcomes of patients with recurrent lumbar disc herniation and signs of instability undergoing stand-alone ALIF), 360° ALIF, or arthroplasty.
Methods This retrospective cohort study was conducted at a single center from August 2019 to January 2024. Inclusion criteria included patients older than 18 years diagnosed with recurrent lumbar disc herniation and signs of instability undergoing stand-alone ALIF, 360° ALIF, or arthroplasty. Exclusion criteria were incomplete data or other indications. Data collected included demographics, surgical specifics (procedure type, operated levels, graft type, and incision type), and clinical outcomes (intraoperative morbidity and short-term postoperative outcomes).
Results Sixty-five patients were evaluated. No intraoperative complications occurred in any group. Mean operative times were 165.8 ± 61.72 minutes for stand-alone ALIF, 236.25 ± 46.3 minutes for 360° ALIF, and 98.43 ± 45 minutes for arthroplasty (P < 0.0001). The mean postoperative hospital stay was 2.46 ± 1.14 days, with no significant difference between groups (P = 0.515). Postoperative complications were minimal: 1 surgical site infection in the stand-alone ALIF group (P = 0.444) and 4 instances of sympathetic changes (P = 0.477), with 1 occurring in the stand-alone ALIF group, 1 in the 360° ALIF group, and 2 in the arthroplasty group. There was no statistical difference between the groups in relation to the visual analog scale and Oswestry Disability Index scores.
Conclusion There was no significant difference in intraoperative morbidity, short-term postoperative outcomes, or length of stay among the 3 groups. All techniques demonstrated good results with low morbidity and short hospitalizations, suggesting that the choice of technique should be based on the surgeon’s experience and the patient’s condition and preferences.
Level of Evidence 4.
- arthroplasty
- anterior lumbar interbody fusion
- ALIF
- retrospective studies
- intervertebral disc displacement
- adults
Introduction
Lumbar disc herniation is a prevalent degenerative condition resulting from a biomechanical imbalance, characterized by the extrusion of the nucleus pulposus through microfractures in the annulus fibrosus.1 This pathology often manifests with debilitating symptoms, including radicular pain mediated by inflammatory chemokines and motor or sensory deficits caused by compression of the dural sac or nerve roots.2 While conservative management, such as physical therapy and pharmacological interventions, is effective in many cases, surgical intervention becomes necessary when these measures fail.3 Primary surgical procedures, such as nerve root decompression, are widely utilized but are associated with recurrence rates ranging from 2% to 25%, often necessitating reoperation.4–10
Recurrent lumbar disc herniations may progress to segmental instability, requiring more advanced surgical approaches beyond simple decompression, including stand-alone anterior lumbar interbody fusion (ALIF), 360° ALIF, and arthroplasty. Stand-alone ALIF provides optimal disc space visualization and sagittal alignment correction while minimizing invasiveness, intraoperative bleeding, and recovery time.11–13 The 360° ALIF, incorporating posterior lumbar instrumentation, enhances spinal stability and fusion rates, albeit with increased surgical complexity and operative duration.13,14 Arthroplasty preserves segmental motion while effectively addressing pain and structural instability.15,16 Despite technical differences, these approaches are recognized as viable options for achieving significant clinical improvements with acceptable safety profiles.17–21
The present study sought to compare stand-alone ALIF, 360° ALIF, and arthroplasty in the treatment of recurrent lumbar disc herniation and signs of instability over a 6-month follow-up period, focusing on the effectiveness of nerve root decompression and resolution of painful spinal instability. By delineating the relative advantages and limitations of these techniques, this analysis seeks to inform surgical decision-making, optimize patient-specific treatment strategies, and advance evidence-based practices in spinal surgery.
Materials and Methods
Study Design
We conducted a retrospective observational study at the Hospital Associação de Assistência à Criança Deficiente (AACD) to evaluate and compare the intraoperative and short-term postoperative outcomes of patients with diagnosed recurrent lumbar disc herniation and signs of instability who underwent stand-alone ALIF, 360° ALIF, or arthroplasty between August 2019 and January 2024. All patients were operated on by the same senior surgical team. The selection of these surgical procedures reflects the diversity of surgical approaches and enables a comprehensive analysis of efficacy and safety aimed at optimizing evidence-based clinical practices. This manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology22 guidelines.
Recurrent lumbar disc herniation is defined as a disc herniation refractory to conservative treatment and primary decompressive surgery. In our case series, patients with recurrent disc herniation also presented with signs of spinal instability.
Ethical Considerations
This study was approved by the Associação de Assistência à Criança Deficiente Hospital Research Ethics Committee, ensuring compliance with ethical standards for research involving human subjects. Informed consent was waived due to the retrospective nature of the study and the use of anonymized data.
Study Population
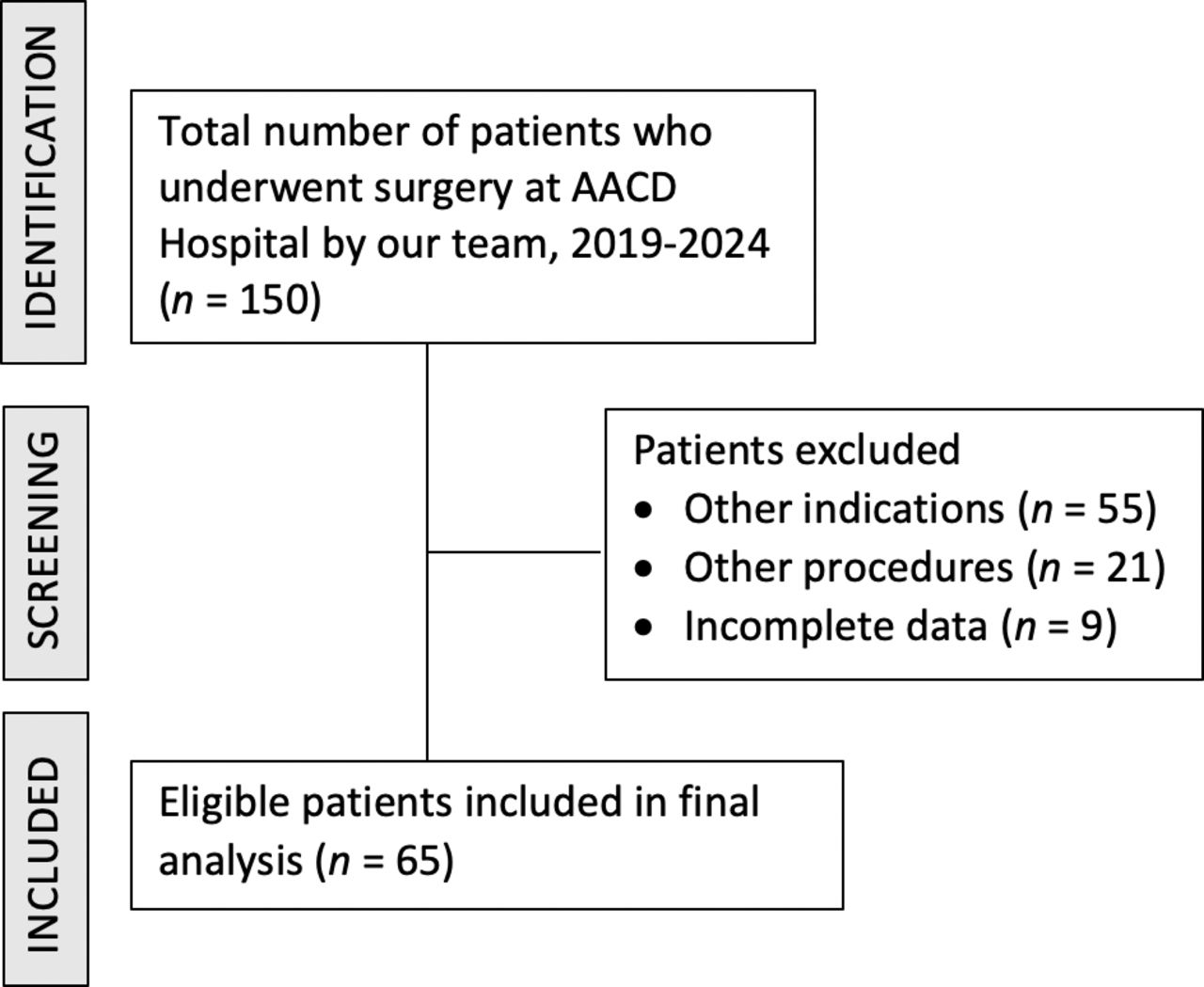
Initially, 150 patients operated on by our team during the specified period were evaluated. Participant selection was based on the analysis of medical records, following well-defined inclusion and exclusion criteria to ensure the comparability and representativeness of the study groups. Patient selection is summarized in the Figure 1.

Strengthening the Reporting of Observational Studies in Epidemiology study flowchart.
Inclusion and Exclusion Criteria
The inclusion criteria for this study were adult patients (age ≥18 years) diagnosed as having recurrent lumbar disc herniation that progressed to clinical signs of spinal instability, as previously defined, and who underwent reoperation using stand-alone ALIF, 360° ALIF, or arthroplasty. Patients who underwent different procedures, had incomplete medical records, or were treated for conditions other than disc herniation, such as pseudarthrosis or spinal stenosis, were excluded from the analysis.
Data Collection
Data collection was carried out by 2 independent researchers following a standardized protocol for reviewing medical records, ensuring the anonymization and confidentiality of the information.23 We extracted demographic data (age, body mass index, and gender), surgical data (type of procedure, levels operated, graft used, and type of incision), and main complaints.
Intraoperative complications were thoroughly assessed and categorized based on predefined criteria. Vascular injuries were defined as significant damage to arterial or venous structures requiring management with local hemostasis or vascular suturing, such as partial avulsions or superficial injuries treated with local hemostasis or simple repairs, as well as major injuries requiring more complex interventions. Injuries to intra- and extraperitoneal organs were recorded when direct trauma or associated complications were identified during the procedure. Damage to the dural sac and nerve roots was considered in cases of intraoperatively observed laceration, avulsion, or compression. Each recorded complication was analyzed alongside the repair strategies employed during the procedure.
Postoperative complications were evaluated retrospectively based on medical records, which documented follow-up visits previously conducted 1 week, 1 month, 3 months, and 6 months after the procedure. During these visits, patients had been interviewed regarding symptoms suggestive of complications, and comprehensive physical examinations had been performed to identify potential adverse events. The complications assessed included cavitary hematoma, wall hematoma, surgical wound infection, retroperitoneal infection, lymphocele, evisceration, deep vein thrombosis, retrograde ejaculation, and sympathetic alterations.
Additionally, the visual analog scale (VAS) was used to measure pain levels before and after the procedure, as documented in the medical records. The Oswestry Disability Index (ODI) was also used to retrospectively evaluate functional disability and the impact of surgical intervention on the patient’s daily activities. Together, these tools provided a comprehensive assessment of the effectiveness of the surgical procedures in alleviating symptoms, restoring functionality, and improving overall patient outcomes.
Subgroup Analysis
We conducted a subgroup analysis based on the operated levels (1 level, 2 levels, and 3 levels) concerning the parameters of operative time and postoperative hospitalization duration. The number of operated levels may act as a potential confounder in our study, as these parameters can vary according to the number of treated levels. Additionally, the groups may exhibit heterogeneity regarding the operated levels, which could distort the average operative time and hospitalization duration in each group.
Surgical Technique
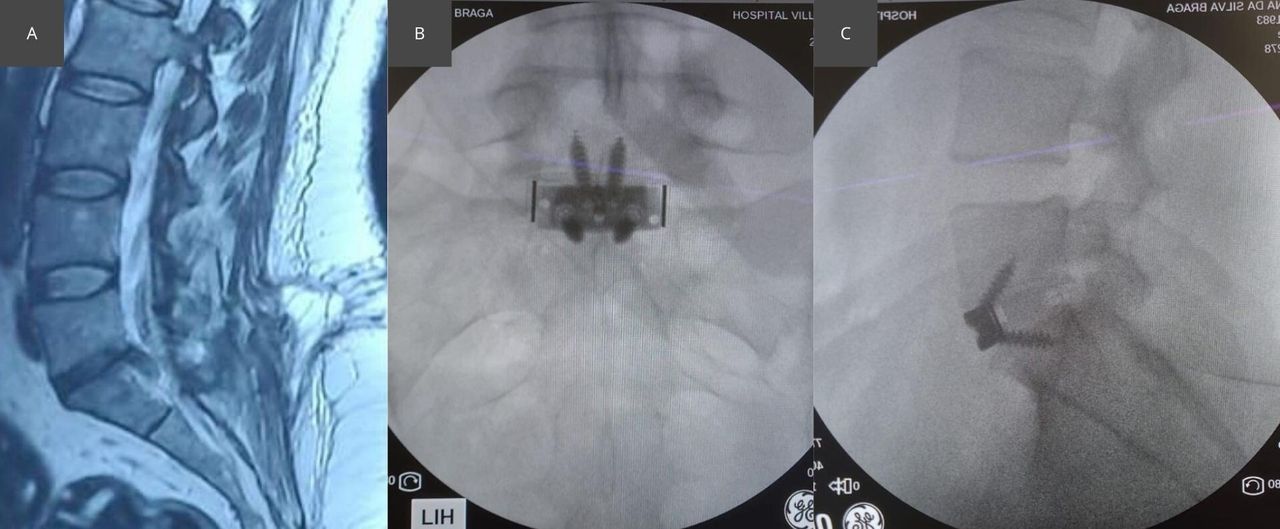
Stand-alone ALIF: This technique involves an anterior approach for lumbar interbody fusion, providing direct access to the lumbar spine without significant damage to the posterior musculature. We utilized a retroperitoneal access route to minimize impact on intra-abdominal organs. Complete discectomy was performed, followed by the insertion of an interbody implant filled with autologous, heterologous, or combined graft (Figure 2).

Stand-alone anterior lumbar interbody fusion: (A) Preoperative image. (B and C) Postoperative images.
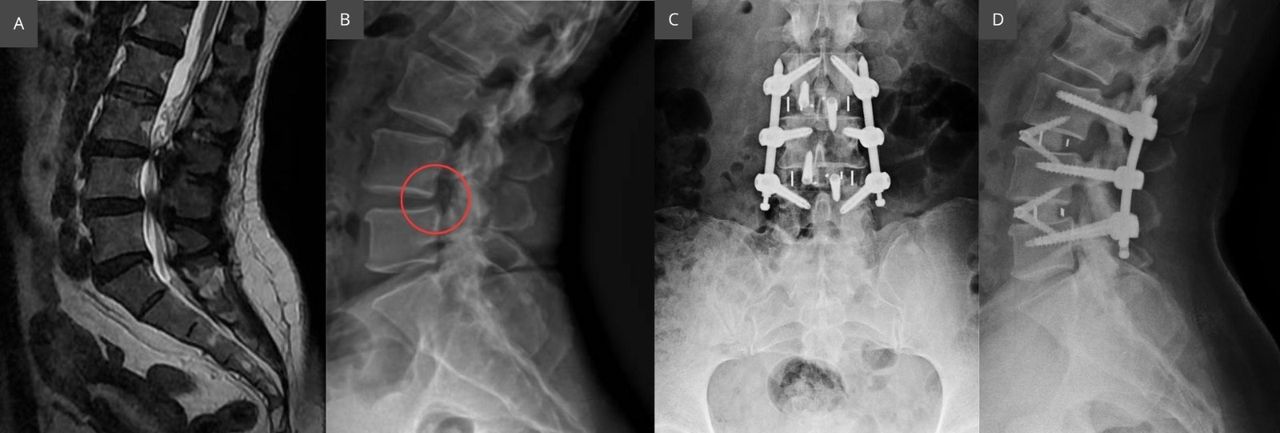
360° ALIF: This approach combined the stand-alone ALIF technique with posterior instrumentation to provide additional stability and increase fusion rates. Following the ALIF procedure as described above, the patient was repositioned for the dorsal approach, where fixation with pedicular screws and rods was performed, completing the 360° fusion (Figure 3).

360° anterior lumbar interbody fusion: (A) Preoperative magnetic resonance imaging. (B) Preoperative x-ray image. The red circle indicates segmental instability due to listhesis. (C and D) Postoperative x-ray images.
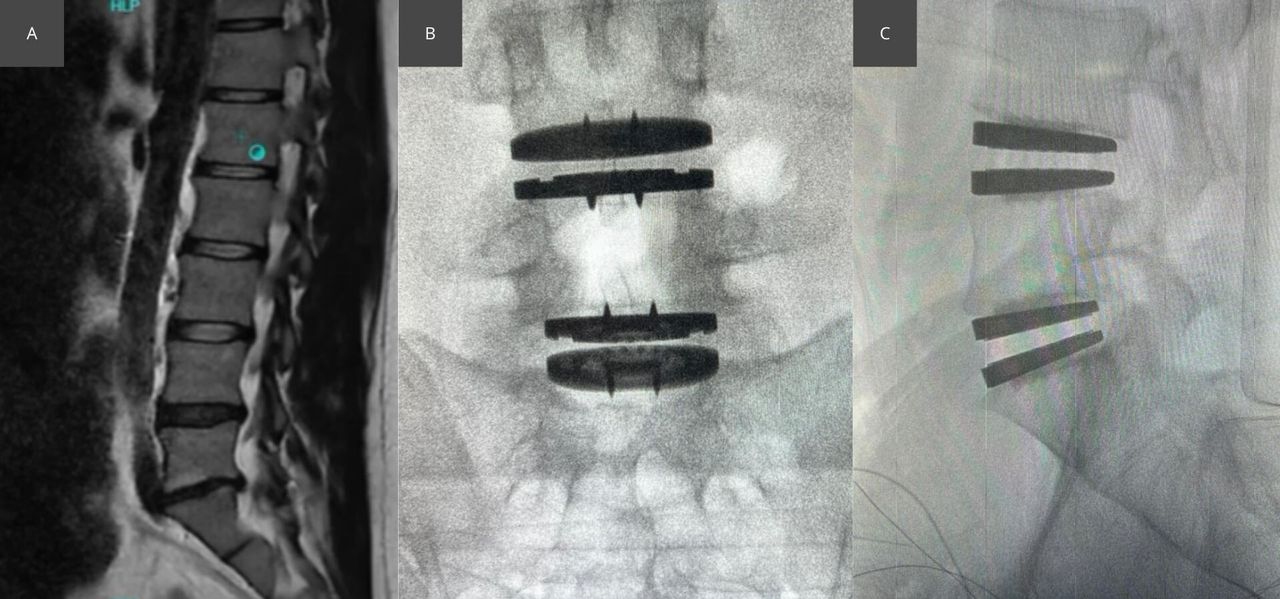
Arthroplasty: Total disc replacement was performed using an anterior approach similar to that used for stand-alone ALIF. Discectomy was followed by meticulous preparation of the disc space to accommodate the artificial disc implant, aiming to preserve motion and alleviate pain while avoiding spinal fusion (Figure 4).

Arthroplasty: (A) Preoperative image. (B and C) Postoperative images.
All techniques were performed under general anesthesia, following strict asepsis protocols. The standardization of surgical techniques, combined with the surgical team’s experience, ensured consistency and reproducibility of the procedures, allowing for an accurate assessment of postoperative outcomes and complications associated with each technique.
We performed stand-alone ALIF in patients with recurrent lumbar disc herniation who exhibited mild degenerative findings on preoperative imaging, including minimal facet joint degeneration, preserved segmental stability on flexion-extension radiographs (axial translation <2 mm), adequate bone quality, and only mild signs of posterior musculature degeneration, such as minimal fatty infiltration or slight muscle atrophy.
ALIF 360° was indicated for patients with more complex profiles, including moderate to severe facet joint degeneration, large facet cysts, spondylolisthesis with pars defects, segmental instability (axial translation >2 mm), multilevel involvement, high pelvic incidence with a sacral slope greater than 40° at L5–S1, reduced bone quality (eg, osteoporosis, diabetes, smoking, or sarcopenia), and more advanced degeneration of the posterior paravertebral musculature. In these cases, the addition of posterior instrumentation was deemed necessary to ensure mechanical stability and promote fusion.
Arthroplasty was selected for patients with preserved disc height, normal facet joints, absence of segmental instability, and good bone and muscle quality, representing optimal candidates for motion-preserving techniques.
Although surgical planning was based on objective radiographic and clinical parameters, the final decision regarding technique was made at the discretion of the operating surgeon, ensuring an individualized approach aligned with each patient’s anatomical and functional characteristics.
Statistical Analysis
We implemented a robust statistical analysis strategy to compare the variables collected among the procedure groups. Initially, normality tests were performed to determine the choice between parametric and nonparametric analyses. Continuous variables were compared using analysis of variance or the Kruskal-Wallis test, while categorical variables were assessed using the χ 2 test or Fisher’s exact test, with corrections for multiple comparisons when necessary. When initial analyses revealed statistically significant differences between the surgical procedure groups, post-hoc analyses were conducted to identify which specific groups differed. For these multiple comparisons, the Tukey test was used for adjustments, ensuring rigorous control of type I error. These post-hoc analyses not only identified the presence of significant differences but also clarified the nature of these differences among specific types of surgical procedures.
The significance level for all analyses was set at P < 0.05 with a 95% confidence interval. Statistical analysis was conducted using Python version 3.11, which provide robust analysis for the proposed models and necessary post-hoc comparisons.
Results
Patient Details
A total of 65 patients were evaluated, with no significant differences in gender distribution (P = 0.562) or body mass index (P = 0.475) among the groups. However, a significant difference in mean age (P < 0.0001) was identified, primarily between the arthroplasty and 360° ALIF groups (P = 0.0007). Neither the stand-alone ALIF and 360° ALIF groups nor the ALIF Stand-Alone and arthroplasty groups showed significant age differences (P = 0.0685 and P = 0.142, respectively; Table 1).
Characteristics of patients (N = 65) undergoing stand-alone ALIF, 360° ALIF, or arthroplasty for recurrent lumbar disc herniation.
All patients had previously undergone 1 to 3 decompression surgeries (mean: 1.8 ± 0.6) for the treatment of herniated discs. However, these procedures were insufficient for complete pain resolution. Consequently, the patient returned to the clinic with a recurrence of sciatic pain, indicative of nerve root compression. Over time, this pain pattern evolved, and patients began experiencing both sciatic and axial pain, suggesting the development of instability-related symptoms.
Perioperative Details
A total of 91 spinal levels were operated on across all procedures. The L5-S1 level was the most frequently treated (41.53%), followed by L4-L5-S1 (24.61%) and L4-L5 (23.08%). In the stand-alone ALIF group, 39 levels were treated, with the majority at L4-L5-S1 (40%) and L5-S1 (32%). Similarly, the 360° ALIF group involved 35 levels, with L5-S1 (37.5%) and L4-L5 (25%) being the most common. The arthroplasty group had 17 levels operated on, predominantly at L5-S1 (62.5%).
Longitudinal incisions were the most common (83.07%), followed by Pfannenstiel (9.23%) and transverse (7.7%). This pattern was consistent across groups, with longitudinal incisions being predominant in stand-alone ALIF (80%), 360° ALIF (87.5%), and arthroplasty (81.25%). Bone grafts were utilized in 49 ALIF procedures, comprising 15 heterologous grafts (30.61%), 16 autologous grafts (32.66%), and 18 combined grafts (36.73%). Stand-alone ALIF patients predominantly received autologous grafts (44%), while 360° ALIF patients most frequently received combined grafts (41.67%). In autologous grafts, no complications were observed at the donor site following cortical bone harvesting (Table 2).
Perioperative details of patients (N = 65) undergoing stand-alone ALIF, 360° ALIF, or arthroplasty for recurrent lumbar disc herniation.
Outcome Details
No intraoperative complications were observed, such as major vascular injuries, nerve root damage, dural sac lesions, or injuries to adjacent organs, in any of the groups.
The average hospital stay was similar across groups, with 2.2 ± 0.76 days for stand-alone ALIF, 2.75 ± 1.48 days for 360° ALIF, and 2.43 ± 1.03 days for arthroplasty, showing no statistical differences (P = 0.515).
Short-term postoperative complications were minimal (Table 3). One patient (1.53%) in the stand-alone ALIF group developed a surgical wound infection, successfully treated with oral cephalexin. Four patients (6.15%) experienced transient sympathetic alterations, with 1 case in the stand-alone ALIF group, 1 in 360° ALIF, and 2 in the arthroplasty group, all resolving within 5 to 7 days. No significant differences were observed for infection rates (P = 0.444) or sympathetic alterations (P = 0.477).
Outcomes of patients (N = 65) undergoing stand-alone ALIF, 360° ALIF, or arthroplasty for recurrent lumbar disc herniation.
Subgroup Analysis
The mean operative time increased with the number of operated levels: 166.27 ± 80.35 minutes for 1 level, 188.82 ± 58.98 minutes for 2 levels, and 223.75 ± 64.72 minutes for 3 levels. In subgroup analysis, significant differences were observed between techniques for all level counts. For 1 level, the operative times were 164.61 ± 65.29 minutes for stand-alone ALIF, 238 ± 50.73 minutes for 360° ALIF, and 96 ± 45.48 minutes for arthroplasty (P < 0.0001). For 2 levels, times were 172.5 ± 62.37 minutes for stand-alone ALIF and 246.42 ± 25.28 minutes for 360° ALIF (P = 0.02), with 1 arthroplasty patient requiring 134 minutes. For 3 levels, times were 190 ± 14.14 minutes for stand-alone ALIF and 257.5 ± 88.38 minutes for 360° ALIF (P < 0.0001).
Hospitalization duration also increased with the number of operated levels but showed no significant differences between techniques. The mean stay was 2.37 ± 1.24 days for 1 level, 2.7 ± 0.92 days for 2 levels, and 2.95 ± 0.65 days for 3 levels. For 1 level, stays were 1.93 ± 0.76 days for stand-alone ALIF, 2.8 ± 1.65 days for 360° ALIF, and 2.33 ± 0.97 days for arthroplasty (P = 0.172). For 2 levels, stays were 2.5 ± 0.7 days for stand-alone ALIF and 3 ± 1.15 days for 360° ALIF (P = 0.334). For 3 levels, stays were 2.7 ± 0.71 days for stand-alone ALIF and 3.2 ± 0.62 days for 360° ALIF (P = 0.293).
Pain and Functional Disability Outcomes
Both pain intensity, measured by the VAS, and functional disability, assessed through the ODI, demonstrated significant improvement across all 3 surgical techniques. The mean preoperative VAS scores were 8.4 ± 1.2 for the stand-alone ALIF group, 8.5 ± 1.0 for the 360° ALIF group, and 8.3 ± 1.3 for the arthroplasty group, reflecting severe pain levels. At the 6-month follow-up, the mean VAS scores decreased to 2.4 ± 0.8, 2.3 ± 0.9, and 2.2 ± 0.7 for stand-alone ALIF, 360° ALIF, and arthroplasty, respectively. Statistical analysis revealed no significant differences in VAS improvement between the groups (P = 0.572), indicating similar efficacy in pain reduction.
The ODI scores showed a parallel improvement. Preoperative ODI scores were 68.0 ± 8.5 for the stand-alone ALIF group, 69.5 ± 7.8 for the 360° ALIF group, and 67.3 ± 9.1 for the arthroplasty group, consistent with severe disability. At the 6-month follow-up, the ODI scores decreased to 22.1 ± 5.7, 21.8 ± 6.0, and 21.5 ± 5.2 for stand-alone ALIF, 360° ALIF, and arthroplasty, respectively. No statistically significant differences in ODI improvement were observed among the groups (P = 0.623), indicating comparable functional recovery across all techniques.
Discussion
Recurrent lumbar disc herniation is defined as a disc herniation refractory to conservative treatment and primary decompressive surgery. In our case series, patients with recurrent disc herniation also presented with signs of spinal instability. These signs include persistent axial pain, progressive functional limitations, and, in some cases, exacerbation of radicular symptoms due to loss of disc height and consequent foraminal narrowing. In this scenario, a repeat decompression alone would not be sufficient to provide lasting symptom relief, as it would fail to address the underlying biomechanical instability, a key factor in the perpetuation of pain.
Segmental instability can lead to abnormal motion of the functional spinal unit, resulting in mechanical overload on the facet joints and adjacent structures, which may contribute to symptom recurrence and further local degeneration. Moreover, simple removal of the herniated fragment without adequate structural support may not restore the original disc height, potentially maintaining indirect neural compression and compromising long-term functional outcomes. For this reason, surgical approaches that combine nerve decompression with stabilization techniques, such as interbody fusion or disc arthroplasty, are preferred in patients with recurrent disc herniation associated with spinal instability.
Our study compared 3 surgical strategies used in the management of this condition—stand-alone ALIF, 360° ALIF, and arthroplasty—with the aim of evaluating their effectiveness in nerve root decompression and the treatment of painful instability. The results observed reinforce the importance of segmental stabilization in improving clinical outcomes, preventing further degeneration, and optimizing functional recovery.
Age Differences in Surgical Selection
The statistically significant age difference observed between patients undergoing arthroplasty and 360° ALIF (P = 0.0007) can be attributed to our selection criteria for surgical techniques. Arthroplasty was chosen for younger patients who demonstrated preserved disc height, normal facet joints, absence of segmental instability, and good bone and muscle quality—including minimal fatty infiltration or atrophy of the posterior paravertebral musculature. In contrast, 360° ALIF was indicated for older patients who typically presented with more complex degenerative profiles, including moderate to severe facet joint degeneration, large facet cysts, segmental instability (axial translation > 2 mm), spondylolisthesis with pars defects, multilevel involvement, high pelvic incidence with a sacral slope >40° at L5–S1, reduced bone quality (eg, osteoporosis, diabetes, smoking, or sarcopenia), and more advanced degeneration of the posterior musculature. These factors necessitated the use of posterior instrumentation to ensure adequate mechanical stability and promote successful fusion.
Comparison of Surgical Outcomes
The findings of this study indicate that stand-alone ALIF, 360° ALIF, and lumbar arthroplasty yield equivalent clinical outcomes in terms of pain relief (VAS) and functional improvement (ODI) for the treatment of recurrent lumbar disc herniation associated with painful instability. Although statistically significant differences in operative time were observed among the groups, these variations did not impact hospitalization duration or complication rates. These findings align with previous studies comparing interbody fusion and arthroplasty in the management of degenerative disc disease. However, this study provides a relevant contribution by considering a specific group of patients who had previously undergone multiple decompression procedures without achieving complete pain relief.
The absence of significant differences in complication rates among the groups is consistent with the findings of Shultz et al,24 who also reported no substantial variations in perioperative outcomes between ALIF and lumbar arthroplasty, except for a higher need for blood transfusion in the ALIF group. Additionally, the biomechanical benefits of ALIF were highlighted in the study by Khedr et al,25 which demonstrated that anterior interbody fusion contributes to the restoration of lumbar lordosis, disc height, and foraminal diameter—factors essential for nerve root decompression.
The results of the present study suggest that the choice of surgical procedure should be individualized, considering the patient’s anatomical characteristics, the severity of instability, and expectations regarding functional recovery. Arthroplasty remains an attractive option for mobility preservation, whereas ALIF may be more appropriate for cases of pronounced instability. Thus, this study enhances the understanding of surgical approaches for recurrent lumbar disc herniation, providing more applicable evidence for a patient group that frequently challenges conventional treatment strategies.
Subgroup Analysis of Operative Time
The subgroup analysis of operative time reinforced the significant differences observed among the 3 surgical techniques, particularly for single-level procedures, where arthroplasty demonstrated the shortest operative time. This difference is possibly observed because arthroplasty is typically performed in younger patients with better abdominal and intervertebral disc conditions. In contrast, patients undergoing ALIF often present with more advanced degenerative disease, characterized by osteophytes, anterior longitudinal ligament adhesions, and absence of the areolar plane—factors that require greater surgical caution and longer dissection time. For 2 and 3 levels, the absence of sufficient cases in the arthroplasty group precluded meaningful comparisons, but the pattern of longer operative times for 360° ALIF compared to stand-alone ALIF persisted, reflecting the additional complexity of posterior instrumentation.
This analysis also confirmed a descriptive increase in operative time with the number of levels operated, aligning with previous findings by Ho et al,26 which reported significantly longer operative times for procedures involving 3 or more levels. These results highlight the impact of both the technique and the surgical complexity on operative time, underscoring the importance of procedural planning to optimize outcomes and resource utilization.
Length of Hospital Stay
Previous studies have shown that ALIF with posterior instrumentation is associated with longer hospital stays compared to stand-alone ALIF.27,28 Factors, such as advanced age, prolonged operative time, and significant blood loss, are commonly cited as contributors to increased hospitalization duration in anterior spine surgeries. However, in our study, no statistically significant differences in hospital stay were observed among the 3 groups, which may be attributed to the absence of intraoperative complications.
Subgroup analysis based on the number of operated levels revealed no significant differences in hospitalization duration between the procedures for 1, 2, or 3 levels. Despite the lack of statistical differences, hospitalization duration descriptively increased with the number of levels operated, a trend consistent with prior findings identifying the number of operated levels as a predictor of longer hospital stays.29
Access Surgeon
In our practice, anterior access is routinely performed by a surgeon with specific training in this approach, which may contribute to the low rates of intraoperative and postoperative complications observed. However, this reflects our institutional experience and may not be generalizable.
Strengths and Limitations
This study provides valuable insights into intraoperative morbidity and short-term postoperative outcomes for 3 surgical techniques—stand-alone ALIF, 360° ALIF, and arthroplasty—performed for recurrent lumbar disc herniation and signs of instability. By including subgroup analyses based on the number of operated levels, the study mitigates potential confounding factors, offering a more nuanced comparison of the techniques. A key strength is the comprehensive evaluation of outcomes, including operative time, hospitalization duration, and functional recovery (VAS and ODI scores), all performed within a consistent clinical protocol and supported by a multidisciplinary team, including an experienced access surgeon.
However, the retrospective design introduces inherent limitations, such as reliance on pre-existing data and the inability to control for all confounding variables. Additionally, the relatively small sample size (n = 65) restricts the generalizability of the findings and limits subgroup analyses, particularly for the arthroplasty group in cases involving multiple operated levels. Future studies with larger and more diverse populations, as well as prospective designs, are recommended to validate and expand upon these results, particularly in long-term outcome assessments and patient-reported satisfaction measures.
Conclusion
The evaluated subgroups demonstrate significant similarity regarding intraoperative morbidity and short-term postoperative outcomes for patients undergoing surgery for recurrent lumbar disc herniation and signs of instability. A statistically significant difference was identified in operative times among the techniques, with arthroplasty having the shortest surgical duration and ALIF 360° the longest. The results suggest that short-term health outcomes are comparable among the 3 groups. All techniques demonstrated good results with low morbidity and short hospitalization times postprocedure, suggesting that the choice of technique should be based on the surgeon’s experience and the patient’s condition and preferences. Future studies that include extended follow-up of these patients may be essential for better determining long-term morbidity.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Institutional Ethics Committee Approval This study was approved by the Associação de Assistência à Criança Deficiente (AACD) Ethics Committee (Approval code: 38429220.8.0000.0085).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.