

Abstract
Background This study aims to evaluate patient perceptions of the outcomes following awake transforaminal endoscopic lumbar decompression surgery for treating degenerative spine diseases.
Methods Over a 1-year period from 2022 to 2023, awake transforaminal endoscopic spine surgeries were performed on 183 patients using local anesthesia and sedation, allowing patients to communicate with the surgical team throughout the procedure. A follow-up app-based survey was sent to these patients to assess their perceptions and outcomes related to the surgery.
Results Out of 183 recipients, 102 patients completed the survey. At the 1-year follow-up, 89.2% of the respondents reported better outcomes in comparison to traditional spine surgeries, and 98% expressed willingness to recommend the procedure to others with similar conditions.
Conclusions The findings demonstrate notable advancements in minimally invasive spine surgery, with awake transforaminal endoscopic decompression showing high satisfaction rates tied closely to meeting patient expectations. The study also identifies areas for improvement, particularly in managing postoperative pain and aligning patients’ expectations with clinical results.
Clinical Relevance Effective preoperative communication and consistent pain management practices are critical in enhancing patient satisfaction and postoperative recovery, along with the integration of conservative treatments such as physical therapy and acupuncture to maximize surgical outcomes.
Level of Evidence 2.
- awake transforaminal endoscopic surgery
- degenerative spine diseases
- patient perceptions
- minimally invasive spine surgery
- surgical outcomes
- patient satisfaction
- preoperative communication
- pain management
- postoperative recovery
- conservative treatments
Introduction
Spine surgery for degenerative disease has achieved remarkable advancements in recent decades. Awake transforaminal endoscopic decompression procedures represent one such advancement as an “ultra-minimally invasive” spine surgery approach designed to facilitate patients’ return to an active life without the complications associated with more invasive procedures. A critical aspect of this progress lies in the accurate reporting of patient outcomes, which is essential for evaluating the effectiveness of these procedures and informing clinical practice. Traditionally, the evaluation of outcomes in spine surgery has relied on clinical assessments of pain, function, and overall quality of life. However, contemporary trends underscore the importance of incorporating both patient-reported outcome measures and objective measures, creating a more holistic evaluation of treatment success. This multidimensional approach seeks to capture not only clinical improvements but also the patient’s subjective perspective on their health and well-being following surgery.1,2
The development of specific outcome measures for spine surgery, including the Oswestry Disability Index and visual analog scale, has improved data collection quality. These metrics are frequently complemented by imaging studies and objective clinical assessments, allowing for a nuanced evaluation of surgical success.3 Furthermore, the growing focus on integrating patient-centered outcomes into spine surgery research highlights a shift toward prioritizing functional recovery, symptom relief, and overall satisfaction rather than merely clinical indicators. Standard outcome measures, such as the visual analog scale and the Oswestry Disability Index, while valuable, have significant limitations in capturing whether patient expectations were met following surgical interventions. Various forms of bias and unmet expectations can profoundly influence a patient’s perception of surgical success, particularly regarding their ability to return to work and engage in desired activities. The ultimate definition of clinical success is multifaceted, signifying that patients no longer seek medical services for the same condition. This success is further characterized by rounding out treatment episodes without recourse to additional services such as pain management, chiropractic care, consultations with other spine surgeons, acupuncture, physical therapy, or continued pain medication following surgery.
In this context, the original definition of clinical evidence proposed by Sackett et al consists of 3 essential components: clinical studies and trials, clinical experience, and patient expectations.4 Unfortunately, there is a significant gap in understanding patients’ perceptions of surgical outcomes for many spine surgeries, including transforaminal endoscopic lumbar decompression (TELD). Patient expectations serve as a crucial element of the evidence-based medicine definition, necessitating our focus as authors on addressing this knowledge gap through a patient survey-based investigation.
Materials and Methods
Operative Procedure
For the transforaminal endoscopic (Joimax) spine procedures, the patient was positioned prone on the Jackson table with the Wilson frame. Surgeries were performed under local (1% lidocaine with epinephrine) and intravenous sedation (versed and fentanyl). Patients surveyed had single-level transforaminal decompression surgery for lumbar radiculopathy (patients included are patients with no history of spine surgery, previous laminectomy at the level treated, and previous fusion at the level treated).
Patient Survey
Over a 1-year period from 2022 to 2023, awake transforaminal endoscopic spine surgeries were performed on 183 patients with the diagnosis of lumbar radiculopathy using local anesthesia and sedation, allowing patients to communicate with the surgical team throughout the procedure. Institutional review board approval was obtained from Brown University Health (1194051–13, Outcomes in Lumbar Discectomy Patients). The authors distributed an online questionnaire via Typeform (www.typeform.com) to patients of the first author on 11 December 2024. Patients were invited to evaluate their level of agreement with a set of questions regarding their peri- and postoperative experience and perceptions of outcomes and utilization of postoperative services following a TELD procedure for sciatica-type low back or leg pain due to symptomatic herniated disc or spinal stenosis refractory to conservative care. Patient responses were graded using a Likert scale from 1 (low) to 5 (high). This survey was administered both at the beginning and the end of the webinar to monitor any shifts in the participants’ endorsements due to the information presented. Of the 183 patients, 102 voluntarily submitted completed survey responses.
Statistical Methods and Rasch Analysis
The dataset was exported to Excel and processed using Jamovi (version 2.3). Descriptive statistics were employed to outline responses, computing means, ranges, SDs, and percentages. Relationships between variables were evaluated through χ 2 tests. For Rasch analysis, the item response theory module in Jamovi was utilized. Statistical significance was determined at a P value below 0.05 with a 95% confidence interval. The survey used the polytomous Rasch model, as explained by Andrich. This model proposes that an individual’s traits and the item’s characteristics together determine the likelihood of a particular outcome. It categorizes responses into levels such as “strongly agree,” “agree,” “neutral,” “disagree,” or “strongly disagree.” In this model, a score of x on an item means the respondent exceeds x thresholds but not the remaining m − x. Log odds (logit) form the mathematical basis, estimating the probability of item endorsement based on the difference between a person’s ability and item difficulty. Model fit was assessed using χ 2 statistics, as well as infit and outfit metrics. Results from the Rasch analysis are illustrated with person-item map charts.
Sample Size
For the Rasch model to provide reliable measures, there needs to be alignment between the number of items and participants. This balance is crucial in psychometrics to ensure measurement reliability. As noted by Azizan et al,5 having an equal number of items and participants, such as 30 items and 30 participants, with suitable targeting and model fit, is expected to yield stable measures. These measures should be within ±1.0 logits at a 95% confidence level. More than 50 respondents are typically considered sufficient to analyze the sufficient data fit to the Rasch model at a 99% confidence interval.
Results
Survey Patients and Demographics
The patient survey focusing on outcomes and satisfaction following endoscopic transforaminal surgery resulted in 102 completed responses, which comprised the final dataset. Respondents took an average of 8 minutes and 9 seconds to finish the survey. Participants had a mean (SD) age of 68.1 (13.0) years (range, 27.0 to 89.0 years). Among these patients, 60.8% were men and 39.2% were women. The mean duration of symptoms before surgery was around 30.0 months, although some patients experienced symptoms for 120.0 months or more. Before surgery, 59.8% of the patients (61 of 102) were employed, and a notable 78.7% of those (48 of 61) returned to work after surgery.
Surgical Outcomes and Patient Satisfaction
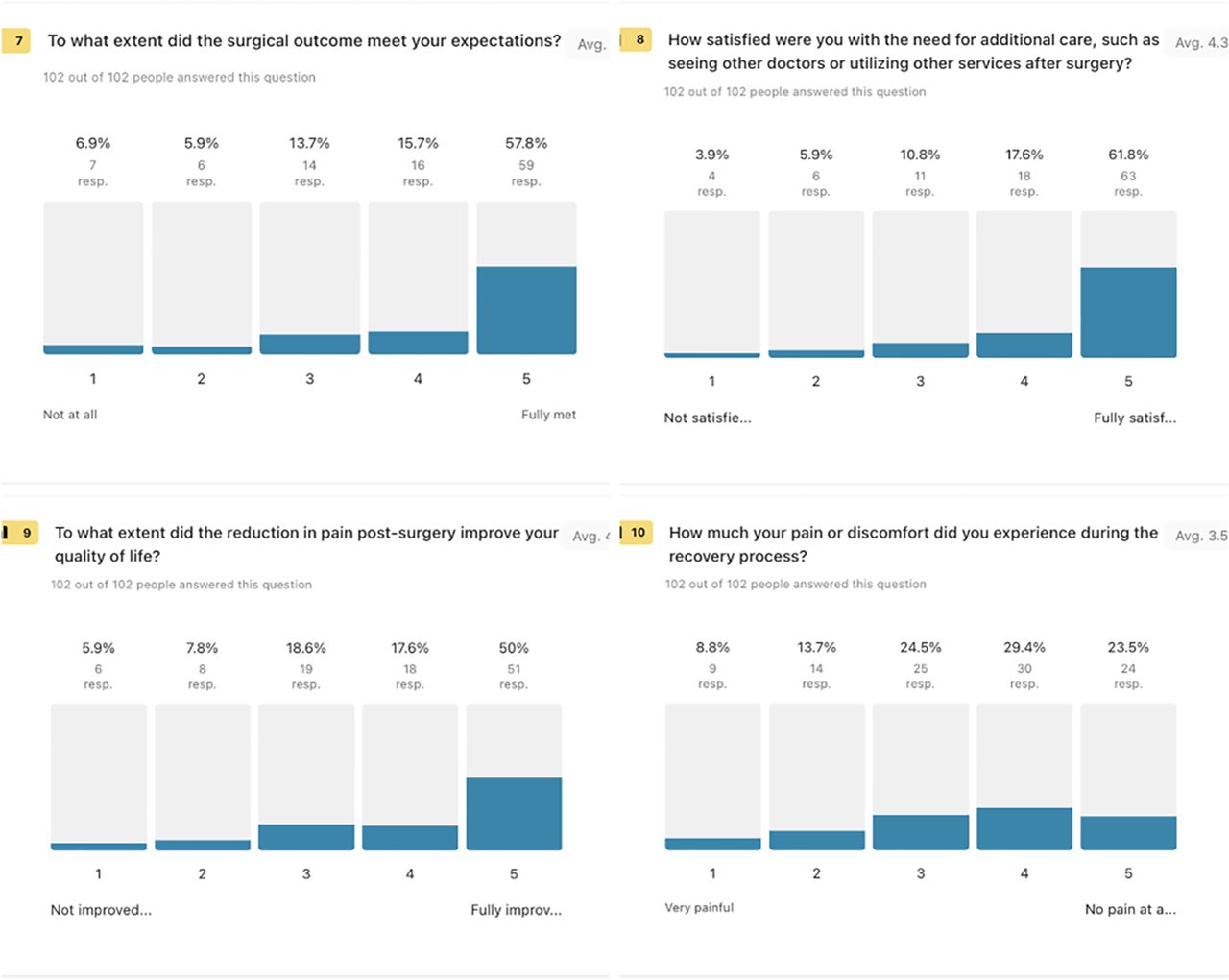
The survey results show that surgical outcomes were generally positive, with an average satisfaction rating of 4.3. Specifically, 57.8% of respondents reported that their expectations were fully met, while 15.7% rated them as a 4, 13.7% as a 3, 5.9% as a 2, and 6.9% as not met at all. Regarding the need for additional care after surgery, 61.8% of participants were fully satisfied, giving the experience an average rating of 4.3. Additionally, 17.6% rated their satisfaction as a 4, 10.8% as a 3, 5.9% as a 2, and 3.9% as not satisfied. In terms of quality-of-life improvement due to reduced postsurgical pain, 50% felt fully improved, with an average score of 4.1. The breakdown further reveals that 17.6% rated their improvement as a 4, 18.6% as a 3, 7.8% as a 2, and 5.9% as not improved. Lastly, experiences during recovery regarding pain or discomfort varied. The average discomfort rating was 3.5, with 23.5% experiencing no pain at all (5), 29.4% rating it as a 4, 24.5% as a 3, 13.7% as a 2, and 8.8% as very painful (1). These results indicate a largely favorable response to the surgical processes and subsequent recovery experiences (Figure 1).

Perceptions of surgical outcomes and recovery after awake transforaminal endoscopic decompression. This figure illustrates responses from 102 patients on the extent to which surgical outcomes met expectations. The mean satisfaction rating was 4.3, mean satisfaction with the need for additional postsurgical care was 4.3, mean impact of reduced pain on quality of lifewas 4.1, and mean the level of pain experienced during recovery of 3.5.
Recovery Experience and Procedure Impact Assessment
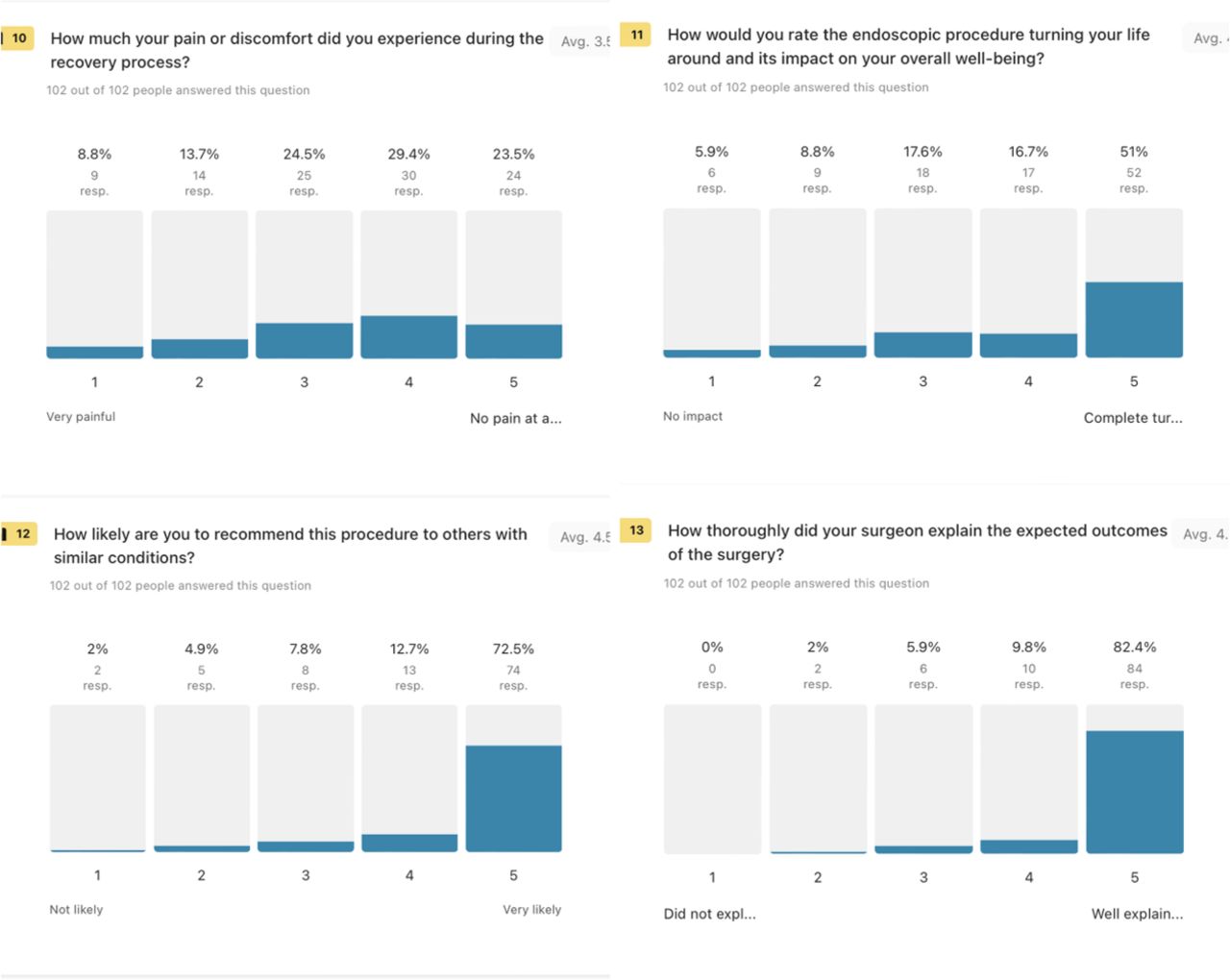
The survey results for the recovery process indicated a mean pain or discomfort rating of 3.5. Among the respondents, 23.5% reported no pain at all, while 29.4% rated their discomfort as a 4, 24.5% as a 3, 13.7% as a 2, and 8.8% as very painful. When evaluating the endoscopic procedure’s impact on overall well-being, respondents gave an average score of 4.1, with 51% indicating that it completely turned their lives around. Further breakdown shows 16.7% rated it as a 4, 17.6% as a 3, 8.8% as a 2, and 5.9% as having no impact. When asked about recommending the procedure to others with similar conditions, the mean likelihood rating was 4.5. A significant 72.5% of participants were very likely to recommend it, with 12.7% rating it as a 4, 7.8% as a 3, 4.9% as a 2, and 2% as not likely. Regarding the thoroughness of the surgeon’s explanation of expected outcomes, the average score was 4.7, with 82.4% feeling expected outcomes were well explained. In addition, 9.8% rated the explanation as a 4, 5.9% as a 3, 2% as a 2, and no respondent rated the explanations as inadequate. These responses generally reflect positive experiences and satisfaction levels with the procedure and the communication involved (Figure 2).

Assessment of recovery and procedural impact after awake transforaminal endoscopic decompression. This figure presents data from 102 respondents regarding pain and discomfort during recovery, with a mean score of 3.5. The impact of the endoscopic procedure on overall well-being had a mean rating of 4.1. The mean likelihood of recommending the procedure to others was 4.5, and the thoroughness of the surgeon’s explanation of expected outcomes was rated highly at 4.7.
Patient Perspectives on Surgical Outcomes and Symptom Management
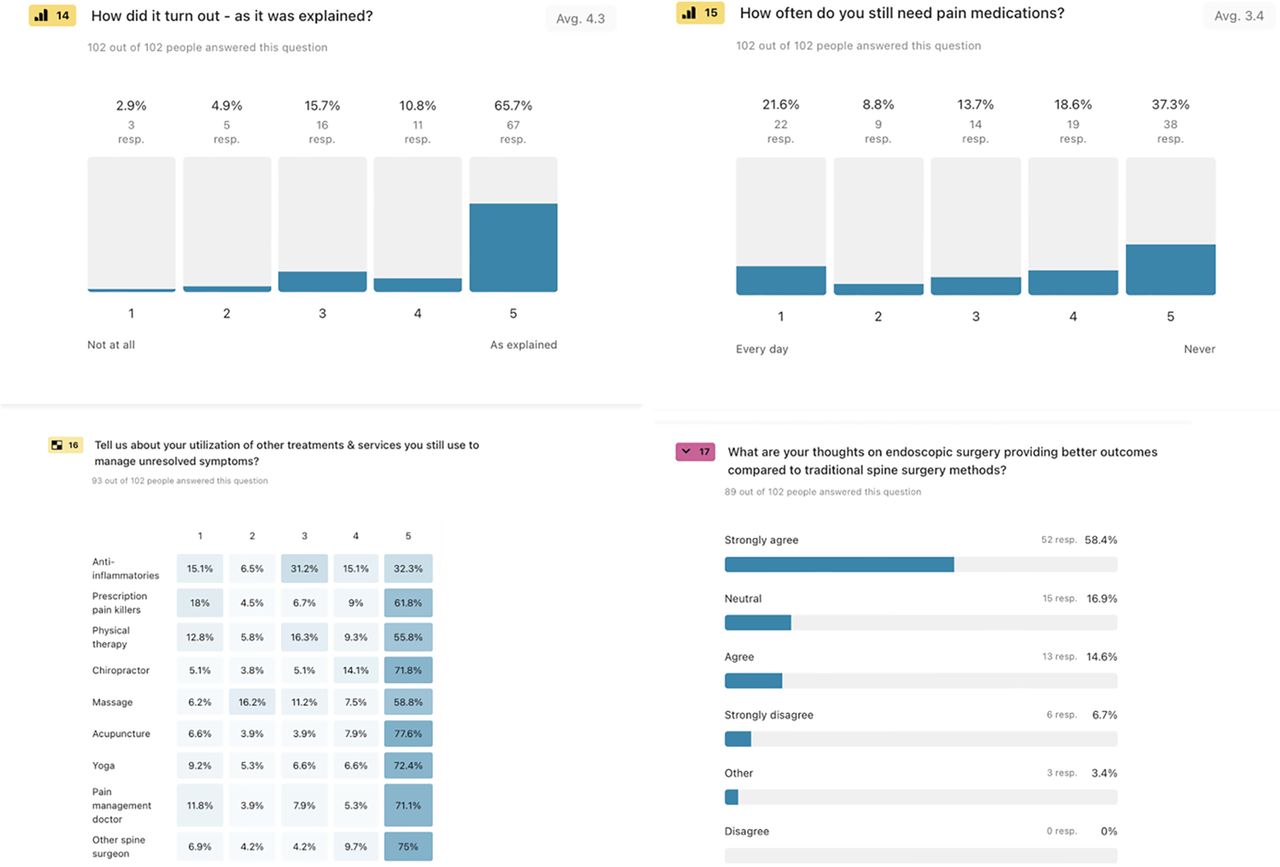
The survey responses also offered a comprehensive view of the participants’ experiences regarding how surgical outcomes matched with preoperative explanations: 65.7% (67 individuals) felt they were as explained, with a mean rating of 4.3. Pain medication usage varied, with 37.3% (38 respondents) never needing it, averaging a score of 3.4. Meanwhile, 21.6% (22 respondents) required it daily. To manage unresolved symptoms, 32.3% (30 out of 93) frequently used anti-inflammatories and 61.8% (58) relied on prescription painkillers. Physical therapy and chiropractic care were reported by 55.8% (52) and 71.8% (67) respectively, while acupuncture and yoga saw engagement from 77.6% (72) and 72.4% (69). When comparing endoscopic surgery to traditional methods, 58.4% (52 out of 89) strongly agreed that it offers better outcomes, with 14.6% (13) agreeing and 16.9% (15) neutral. Only 6.7% (6) strongly disagree, and 3.4% (3) expressed other views, with none disagreeing outright, highlighting significant confidence in endoscopic procedures (Figure 3).

Evaluations of surgical outcomes and symptom management after awake transforaminal endoscopic decompression. This figure presents data from 102 respondents, showing how surgical results aligned with explanations (mean rating of 4.3) and pain medication usage frequencies (mean rating of 3.4). It also details the utilization of various treatments like anti-inflammatories, prescription painkillers, physical therapy, and chiropractic care among 93 respondents. Additionally, it reflects opinions on endoscopic vs traditional spine surgery from 89 respondents, with a majority strongly agreeing on better outcomes with endoscopic methods.
Unsolicited Patient Comments
The feedback on endoscopic spine surgery highlights a range of experiences from patients. Many appreciated the quicker recovery and reduced pain compared with traditional surgeries. Several described significant relief and satisfaction, with some noting immediate improvement and others finding the procedure life changing. The primary surgeon received frequent praise for his expertise and compassion, with patients expressing gratitude for his minimally invasive approach. However, some reported ongoing pain, complications, or less effective results, necessitating further treatment. Despite these issues, many patients would recommend the procedure and the surgeon, noting improvements in mobility and daily life. While some faced challenges like nerve damage and unexpected outcomes, the overall sentiment was positive, with many considering the procedure a valuable alternative to more invasive surgeries. The following list provides some examples of patient feedback on endoscopic surgery:
Recovery was significantly quicker, and pain was much lower compared with traditional surgery.
“The surgeon was very kind and helpful. It is still a work in progress.”
Immediate results with recovery time in days, not months.
“I feel another trial with this procedure would be helpful.”
“The surgery worked exactly as promised, allowing me to resume normal activities.”
Ongoing pain led to further surgery but praised the initial procedure’s quality.
“Feeling awesome and very satisfied with the outcome.”
Some pain returned weeks later but markedly less than before surgery.
Gratitude was expressed toward Dr. Telfeian for his care and expertise.
“The endoscopic surgery was life changing, allowing me to enjoy life again.”
Rasch Analysis
The Rasch analysis provides insights into the fit and effectiveness of a series of survey items. The model fit reveals a person reliability of 0.739, indicating moderate consistency in responses, while the MADaQ3 value of 0.170 and a significant P value (<0.001) suggest a good fit to the Rasch model. Comparing models, the partial credit model (PCM) has a log-likelihood of −671 and deviance of 1342, with an Akaike information criterion of 1400 and a Bayesian information criterion of 1476, across 29 parameters for 102 respondents. The rating scale model is slightly simpler with 11 parameters, showing a log-likelihood of −683 and deviance of 1366. While PCM offers a marginally better fit due to its complexity, both models adequately describe the data. The Q3 Correlation Matrix highlights correlations among items, with notable positive correlations such as 0.517 between “To what extent did the surgical outcome meet your expectations?” (A) and “To what extent did the reduction in pain postsurgery improve your quality of life?” (C), indicating that expectations and quality of life improvements are related. Conversely, “How much pain or discomfort did you experience during the recovery process?” (D) shows negative correlations with several items, such as −0.499 with “To what extent did the surgical outcome meet your expectations?” (A), suggesting that individual experiences of pain during recovery were impacted by other aspects. The Q3 Correlation Matrix shows several negative correlations, indicating inverse relationships between items. These included the item “How satisfied were you with the need for additional care, such as seeing other doctors or utilizing other services after surgery?” (B) and “To what extent did the reduction in pain postsurgery improve your quality of life?” (C): −0.103; or “To what extent did the reduction in pain postsurgery improve your quality of life?” (C): −0.527; and “How would you rate the endoscopic procedure turning your life around and its impact on your overall well-being?” (E); and other items such as “How much pain or discomfort did you experience during the recovery process?” (D): −0.235. These negative correlations suggest that as the experience of positive outcomes or satisfaction increases, the perceived need for additional care or reported discomfort decreases.
Item statistics demonstrated varied difficulty levels and fit statistics. “To what extent did the surgical outcome meet your expectations?” (A) and “To what extent did the reduction in pain postsurgery improve your quality of life?” (C) have low outfit values, suggesting good response predictability, while “How satisfied were you with the need for additional care, such as seeing other doctors or utilizing other services after surgery?” (B), “How much pain or discomfort did you experience during the recovery process?” (D), and “How thoroughly did your surgeon explain the expected outcomes of the surgery?” (G) displayed higher outfit values, indicating unexpected responses from some individuals. In delta-tau parameterization, “How thoroughly did your surgeon explain the expected outcomes of the surgery?” (G) exhibits extreme values, implying issues with respondent differentiation. This aligns with its Thurstone thresholds, which show a wide range from −12.00 to −2.034, indicating divergence in perceived difficulty. The analysis suggests a generally good fit for the model, with some items not meeting patients’ expectations. Table 1 summarizes the survey items with their respective measures, fit statistics, and patient agreement strength, which prioritizes the survey items from the strongest to the weakest patient agreement.
Patient responses by level of agreement on surgical experience.
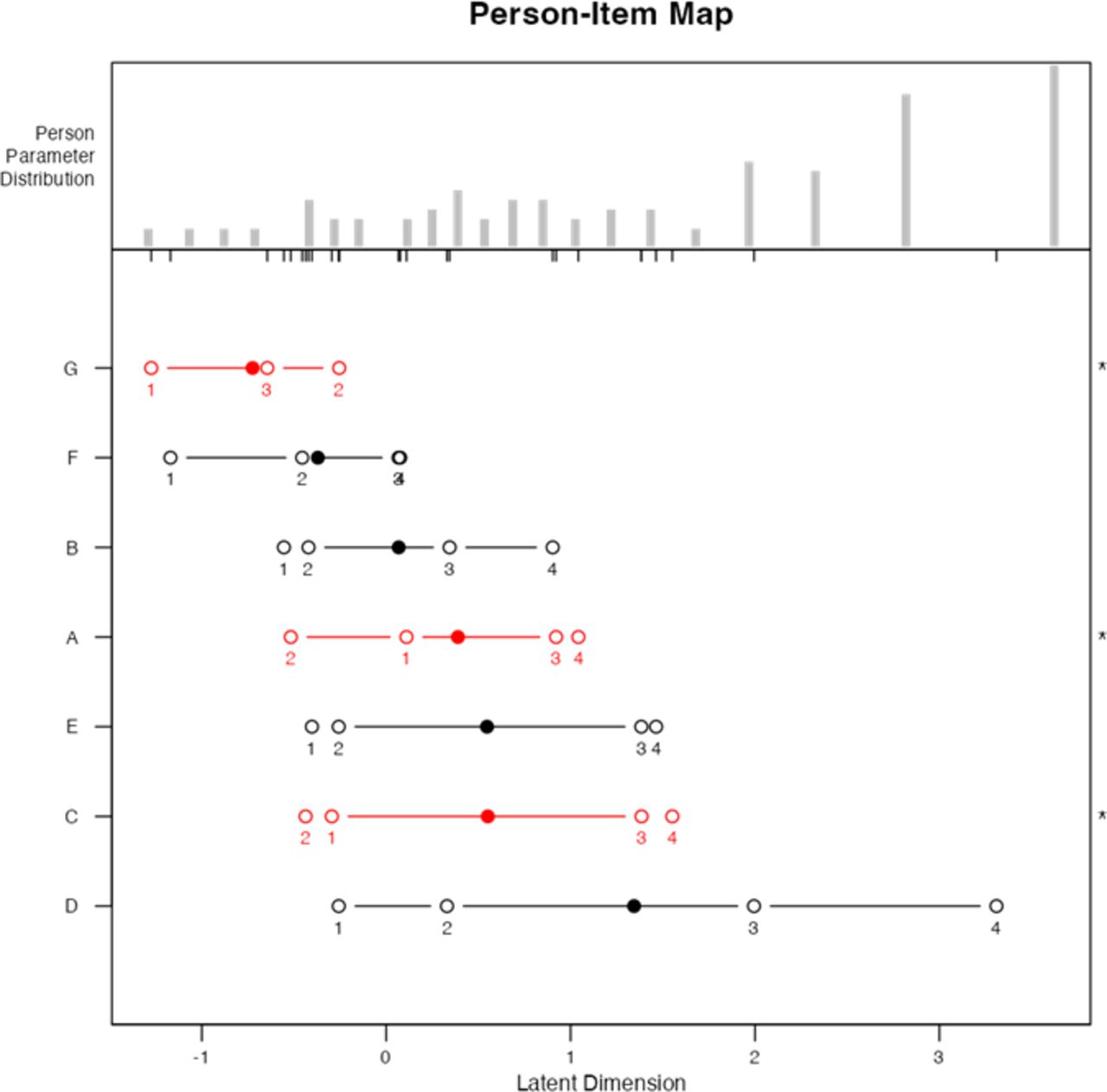
These findings are graphically depicted in the person-item map, which provides a comprehensive view of patients’ perceptions and the level of agreement (item difficulties), reflecting the findings from the previous analyses (Figure 4). The distribution of respondents’ partial agreement is clustered toward the middle, suggesting most participants have moderate agreement levels regarding their experiences and expectations related to the surgery. The item thresholds reveal different difficulty levels for each survey item. “To what extent did the surgical outcome meet your expectations?” (A) shows moderate difficulty, aligning with the general notion that expectations were largely met. Items such as “How satisfied were you with the need for additional care?” (B) and “How much pain or discomfort did you experience during the recovery process?” (D) vary more significantly, reflecting diverse experiences as supported by the higher outfit statistics and noted negative correlations.

The person-item map illustrates the distribution of patients’ abilities and unmet expectations regarding their surgical experience. The middle clustering highlights moderate abilities across patients. The logical progression of the logits from 1 to 4 for items F, B, E, and D, shown as black lines, represents the increasing levels of agreement or response categories for these items. The location of the mean logit (black solid dot) indicates the average level of challenge or ease with which patients agreed with each survey question. Item (F) “How likely are you to recommend this procedure to others with similar conditions?”: The placement of its mean logit suggests that most patients found it easy to agree, aligning with the “very high” agreement level. Item (B) “How satisfied were you with the need for additional care?” and item (E) “How would you rate the endoscopic procedure’s impact on your overall well-being?”: Their mean logits indicate moderate ease of agreement, reflecting the mixed levels of satisfaction and perceived impact. Item (D) “How much pain or discomfort did you experience during the recovery process?”: The mean logit’s position shows variable responses, suggesting that pain during recovery was more challenging to evaluate consistently among patients. Item thresholds indicate varied expectations, with “To what extent did the surgical outcome meet your expectations?” (A) showing moderate unmet expectations. Items such as “How satisfied were you with the need for additional care?” (C) indicating high satisfaction and recommendation likelihood. Communication effectiveness is noted through (G) “How thoroughly did your surgeon explain the expected outcomes?”, where variability suggests areas for improvement.
The Rasch analysis of the remaining survey questions regarding patients’ perceptions about their experience when going through the process of a TELD procedure and their experiences in the postoperative recovery process provided additional insights that are relevant in defining clinical outcomes with the procedure. Analysis of the model’s fit and effectiveness indicated less consistency among patient responses for the second set of survey questions, with a person reliability of 0.603. With an MADaQ3 of 0.228 and a significant P value (<0.001), the data suggest a reasonable fit to the Rasch model. Comparing models, the PCM exhibits a log-likelihood of −705 and deviance of 1410, with an Akaike information criterion of 1500 and a Bayesian information criterion of 1599 across 45 parameters for 67 patients. The rating scale model, slightly simpler with 15 parameters, presents a log-likelihood of −734, indicating a slightly poorer fit than PCM.
The Q3 Correlation Matrix reveals positive correlations among items “How did it turn out—as it was explained?” (H), “How often do you still need pain medications?” (I), and “anti-inflammatories” (J), indicating aligned patient responses, while negative correlations, especially with “chiropractor” (M), suggest differing perceptions or experiences as to the usefulness of continued chiropractic care after transforaminal endoscopic decompression surgery. Examining item statistics, items “physical therapy” (L) and “pain management doctor” (Q) show lower outfit values, suggesting predictable responses, whereas “How often do you still need pain medications?” (I) and “anti-inflammatories” (J) present higher outfit values, indicating some unexpected responses. Most items have infit values near 1, reflecting decent predictability. In the delta-tau parameterization, the measure of each item varies. “How did it turn out—as it was explained?” (H) displays varied parameters, whereas “How often do you still need pain medications?” (I) and “anti-inflammatories” (J) indicate closer clustering, suggesting more consistent experiences. Overall, the analysis reflects a moderate fit for the model, with some items such as “chiropractor” (M) showing variation, highlighting areas for further evaluation to ensure they align with patient experiences. The respective fit statistics are listed in Table 2, which prioritizes the survey items from strongest to weakest patient agreement.
Patient responses by level of agreement on postoperative aftercare.
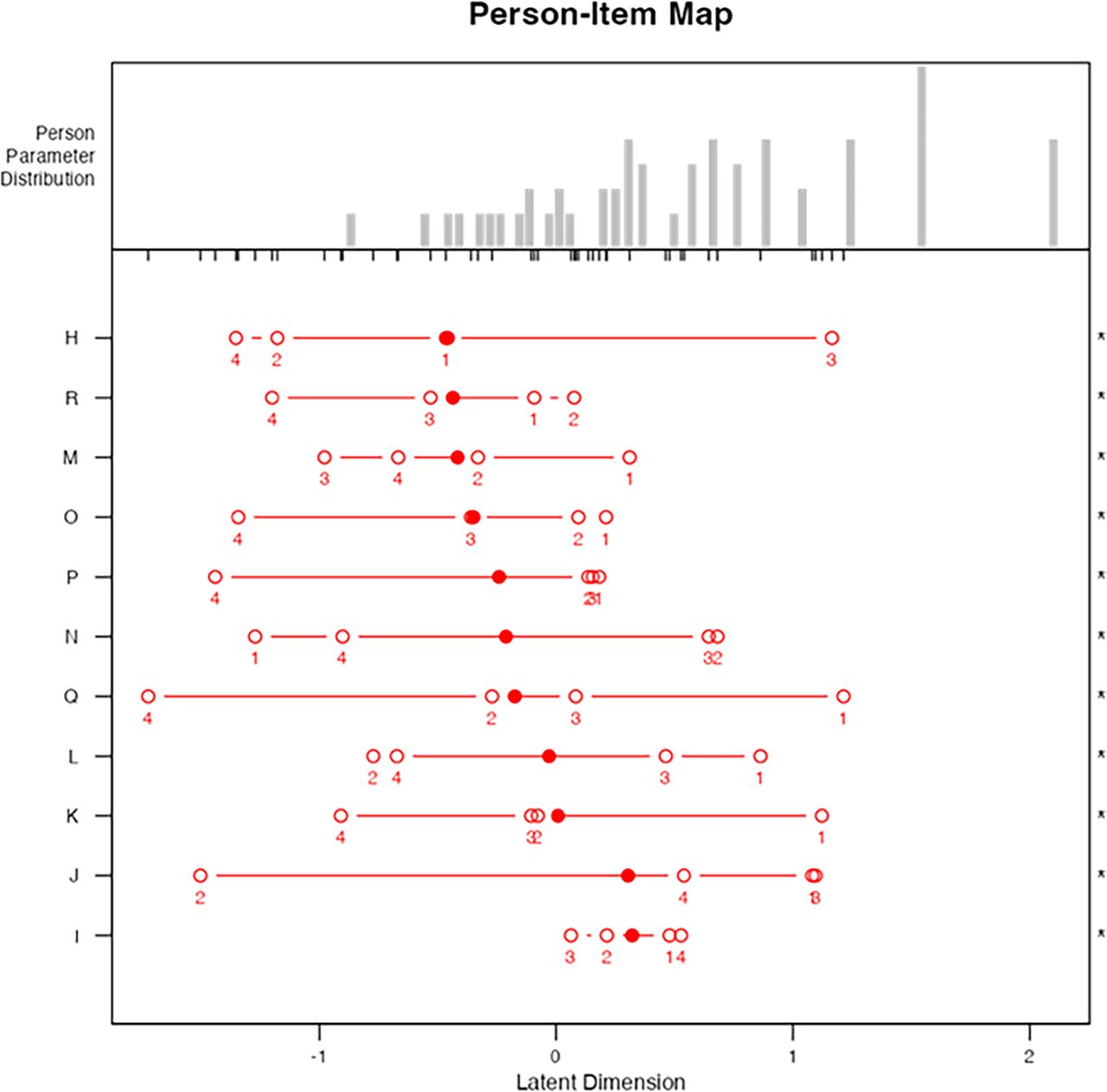
The corresponding person-item map (Figure 5) provides additional insights into patients’ perceptions and the level of agreement (item difficulties) on questions regarding their postoperative recovery, postoperative pain management, other treatments, interventions, and consultations. The gray bars show the distribution of patient abilities, with most clustered in the middle, indicating moderate levels of agreement or perception of outcomes. The red lines and dots display expectation levels across survey questions. Close-spaced thresholds imply consistent patient responses, reflecting similar perceptions, while wider spacing suggests more variability. “How did it turn out—as it was explained?” (H) is positioned where patients generally agree, indicating expectations were mostly met. However, “How often do you still need pain medications?” (I) and “anti-inflammatories” (J) show variability, reflecting diverse experiences in medication needs. Treatments such as “physical therapy” (L) and “chiropractor” (M) indicate high agreement, suggesting they were well received. Similarly, “acupuncture” (O) and “pain management doctor” (Q) align with high patient satisfaction. In contrast, “prescription pain killers” (K), “massage” (N), “yoga” (P), and “other spine surgeon” (R) reflect moderate to variable responses, highlighting areas of low perceived additional benefits with mixed patient experiences. The lack of logical progression of the logits suggests that certain items do not align well across response categories, indicating inconsistencies in how patients perceive or respond to these aspects of care.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The person-item map illustrates patient abilities and expectations regarding survey questions related to postoperative care and treatments. The gray bars represent the distribution of patient abilities, predominantly centered, indicating moderate agreement levels. Red lines and dots depict expectation thresholds across items, revealing consistent responses where thresholds are closely spaced and variability where they are wider. Items such as “physical therapy” (L) and “chiropractor” (M) show high agreement, while “How often do you still need pain medications?” (I) and “anti-inflammatories” (J) indicate more variability, reflecting diverse patient experiences. The map identifies areas of consistent satisfaction and opportunities for improvement, indicated by the lack of logical progression in some logits.
Discussion
Patient perspectives on awake transforaminal endoscopic decompression surgery outcomes have shown promising results, with many patients reporting high satisfaction due to the minimally invasive nature of the procedure and reduced recovery times. Studies highlight that patients appreciate the ability to communicate during surgery, which enhances their sense of control and safety.6 Furthermore, outcomes such as lower postoperative pain levels, reduced opioid use, and shorter hospital stays have been frequently cited.7 However, patient experiences can vary depending on factors like preoperative expectations, underlying health conditions, and surgeon expertise. Despite these variables, the majority of patients indicate that the benefits, including quicker return to daily activities and improved quality of life, outweigh the discomfort associated with the awake procedure.8 Continued exploration of patient-reported outcomes will be essential to refining techniques and optimizing the overall surgical experience.
The relationship between patient expectations and surgical outcomes in the present study revealed several positive correlations that significantly influenced patient satisfaction and perceived quality of life. Patients’ overall satisfaction was enhanced when there was an alignment between patient expectations and actual surgical outcomes. As illustrated in Table 1, patients whose expectations were met often report improved quality of life, which boosted their confidence in the procedure and aligned with a high degree of agreement on outcome satisfaction survey questions. Additionally, satisfaction with surgical results correlated positively with the likelihood of recommending the procedure to others. Patients who experienced successful outcomes were more inclined to endorse the surgery, creating a reinforcing cycle of trust and perceived efficacy. Thorough and comprehensive explanations of potential outcomes also play a crucial role; patients who received clear information reported higher satisfaction, positively influencing their perception of the procedure’s success and enriching their overall experience. The analysis further suggests that consistency in pain management practices is beneficial. Positive correlations between postoperative medication and conservative treatments, such as physical therapy or acupuncture, indicate that adhering to a cohesive pain management plan may yield better outcomes. Regular engagement in these alternative therapies could provide synergistic effects, reducing pain and promoting recovery. Moreover, patients who utilized complementary treatments like massage, yoga, and acupuncture alongside pain medications reported similar levels of satisfaction and relief. This trend points to the advantages of a holistic approach to recovery, where a combination of pharmacological and nonpharmacological treatments reinforce pain reduction and healing.
Conversely, negative correlations in our patient outcome data highlight areas requiring attention. Discrepancies in perceptions regarding additional care may indicate that unmet expectations can detract from overall satisfaction. Patients who experience more postoperative pain often report lower satisfaction, underscoring the need for improved pain management and recovery support resources. Furthermore, how effectively patients feel their expectations were managed can negatively correlate with satisfaction. If communication regarding the procedure is unclear or outcomes do not align with what was initially promised, dissatisfaction can arise, even in the presence of clinical improvements.
Conclusion
This study highlights the significant advancements and patient-centered outcomes associated with awake transforaminal endoscopic decompression procedures for treating degenerative spine diseases. The findings underscore the importance of aligning surgical outcomes with patient expectations, which directly influences overall satisfaction and the perceived quality of life following surgery. A majority of respondents reported that their expectations were met, leading to high satisfaction ratings and a strong willingness to recommend the procedure to others. Clear communication from health care providers regarding the surgical process and expected outcomes plays a crucial role in enhancing patient experiences. Thorough preoperative counseling fosters trust, mitigates discrepancies in care perception, and optimizes postoperative recovery. Moreover, adherence to consistent pain management strategies—including the integration of conservative treatments such as physical therapy, acupuncture, and lifestyle adjustments—contributes to improved recovery outcomes and reinforces the effectiveness of the surgical intervention. Conversely, the study identifies gaps in understanding patient perceptions, particularly concerning pain management and additional postoperative services. Higher rates of postoperative pain and unmet expectations seem to correlate with lower satisfaction levels, pointing to the critical need for ongoing support and effective pain management strategies postsurgery. This highlights the necessity for continual refinement of patient education and support systems to ensure comprehensive care.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
IRB Approval Brown University Health (1194051-13) Outcomes in Lumbar Discectomy Patients.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.