


ABSTRACT
Background Jefferson fractures are classically described as burst fractures of C1. Traditional surgical treatment of these unstable fractures is either occipito-cervical or posterior C1-C2 fusion, resulting in a significant loss of range of cervical neck movement. This case report discusses the fixation of a Jefferson fracture using C1 lateral mass screws to achieve surgical stabilization while preserving the range of movement. We aim to add to the body of evidence supporting this fixation method.
Methods A 39-year-old male presented to our emergency department with an unstable Jefferson fracture caused by trauma. The various treatment options, such as cervical collar, HALO immobilization, occipito-cervical fusion, and atlanto-axial fusion and direct fixation of C1, were evaluated and discussed with the patient. Informed consent was obtained from the patient prior to writing this case report.
Results At 3 months postoperation, the patient demonstrated near full range of movement in his neck. He had also resumed driving. By 6 months, the patient returned to work, and at 12 months, imaging confirmed union.
Conclusions This case report adds to the body of evidence supporting the technique of C1 lateral mass screws for direct stable fixation of Jefferson fractures. This fixation method preserves the cervical spine range of motion with minimal functional restriction.
- Jefferson fractures
- motion preserving
- lateral mass screws
- fracture fixation
- fusion alternative
- direct fixation
- nonfusion
- motion preserving
- C1 fracture
INTRODUCTION
Jefferson fractures are burst fractures of C1 involving bilateral anterior and posterior arches, and they result from axial compression and hyperextension. They make up 2% to 13% of all cervical spine fractures.1 Stable fractures are often treated with a hard collar or HALO immobilization for 6 to 12 weeks. Surgical treatment of unstable fractures is, however, more controversial. Occipito-cervical or posterior atlanto-axial (C1-C2) fusion is often the surgery of choice. Unfortunately, fusion will result in significant loss of cervical spine range of movement. The following case report details an alternate surgical technique to treat unstable Jefferson fractures by means of direct fixation of C1 fracture with C1 lateral mass screws, aimed at preserving range of motion. Although described before,2,3 we hope that this case report adds to the body of evidence supporting it.
CASE REPORT
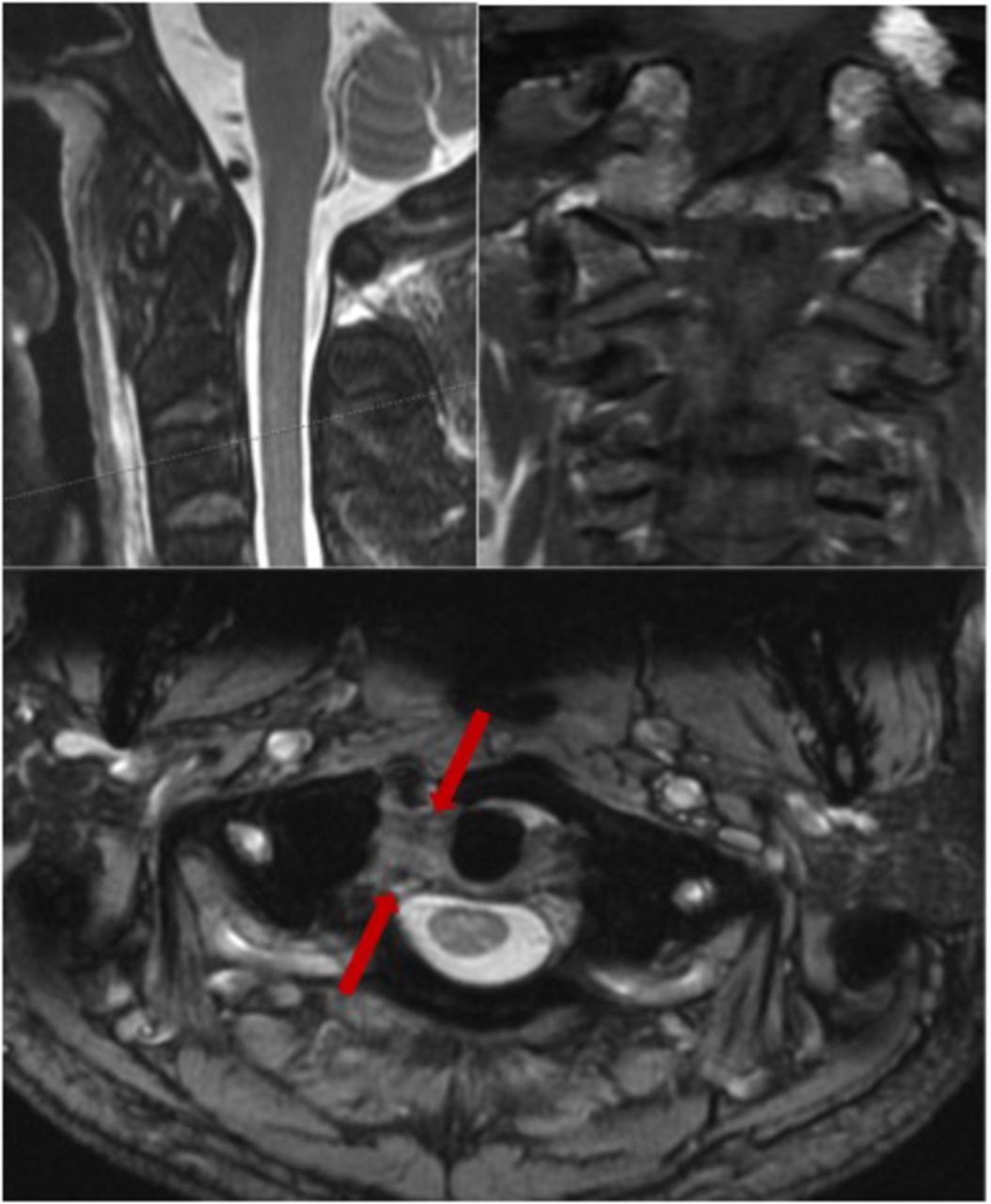
A 39-year-old male, with no medical comorbidities, presented to our emergency department complaining of neck pain for a week following a diving accident when on vacation overseas. He recounted impacting his head against the swimming pool floor. Initial radiographs taken in the emergency department overseas failed to diagnose the C1 fracture. He had no neurological deficits at any point. Further radiographs and computed tomographic (CT) scan revealed fractured anterior and posterior arches of C1 with centrifugal displacement of lateral masses (Figure 1). Carotid and vertebral artery CT angiograms were not indicated due to the subacute presentation and the absence of any clinical manifestations of vascular injury. A magnetic resonance scan later confirmed an intrasubstance tear of the transverse ligament (Figure 2). Treatment options discussed with him included HALO immobilization, occipito-cervical fusion, C1-C2 fusion, or direct fixation with lateral mass screws. After careful consideration, the patient opted for direct fixation.

Preoperative computed tomographic scan showing the displaced fracture of the C1 vertebra with increased C1 lateral mass overhang over C2.
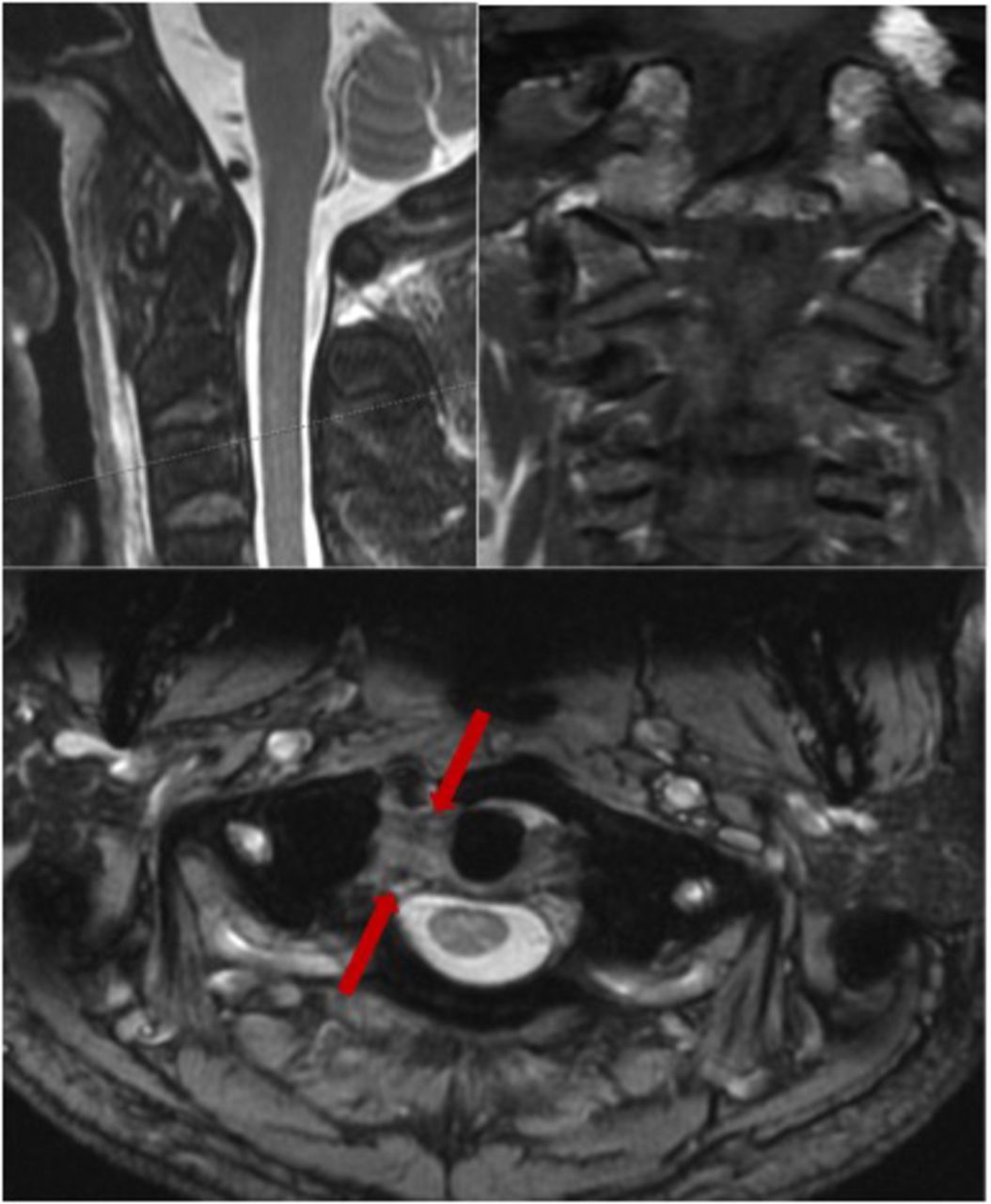
Preoperative magnetic resonance image (sagittal, coronal, and axial) showing an intrasubstance tear in the transverse ligament on the right side (between the red arrows).
The surgery was performed in the prone position on a Jackson table with the head stabilized in a Mayfield headholder. Manual reduction was achieved by traction applied through the Mayfield clamp under fluoroscopic guidance. This was judged by the reduction of the overhang of C1 lateral masses. A midline incision was then made, and the paravertebral muscles were retracted to expose the C1 posterior arch. C2 nerve roots and vertebral arteries were identified and protected throughout to avoid iatrogenic injuries caused by misplacement or migration of instrumentation. The C1 lateral masses were meticulously exposed. The lower borders of overhanging C1 posterior arches were identified as entry points for lateral mass screws and burred to establish smooth entry points. Drilling through the lateral masses was done under II guidance. Partially threaded 34-mm lateral mass screws were inserted bilaterally. The posterior arch fracture was reduced under direct vision by approximating the lateral mass screw heads. A rod was then cut to measure, contoured, and fitted to the screws, achieving further reduction of the anterior arch. End caps were then tightened to achieve compression across the fracture (Figures 3 and 4). The wound was finally washed with saline and a radivac drain inserted before executing a layered closure. An Aspen collar was applied postprocedure.

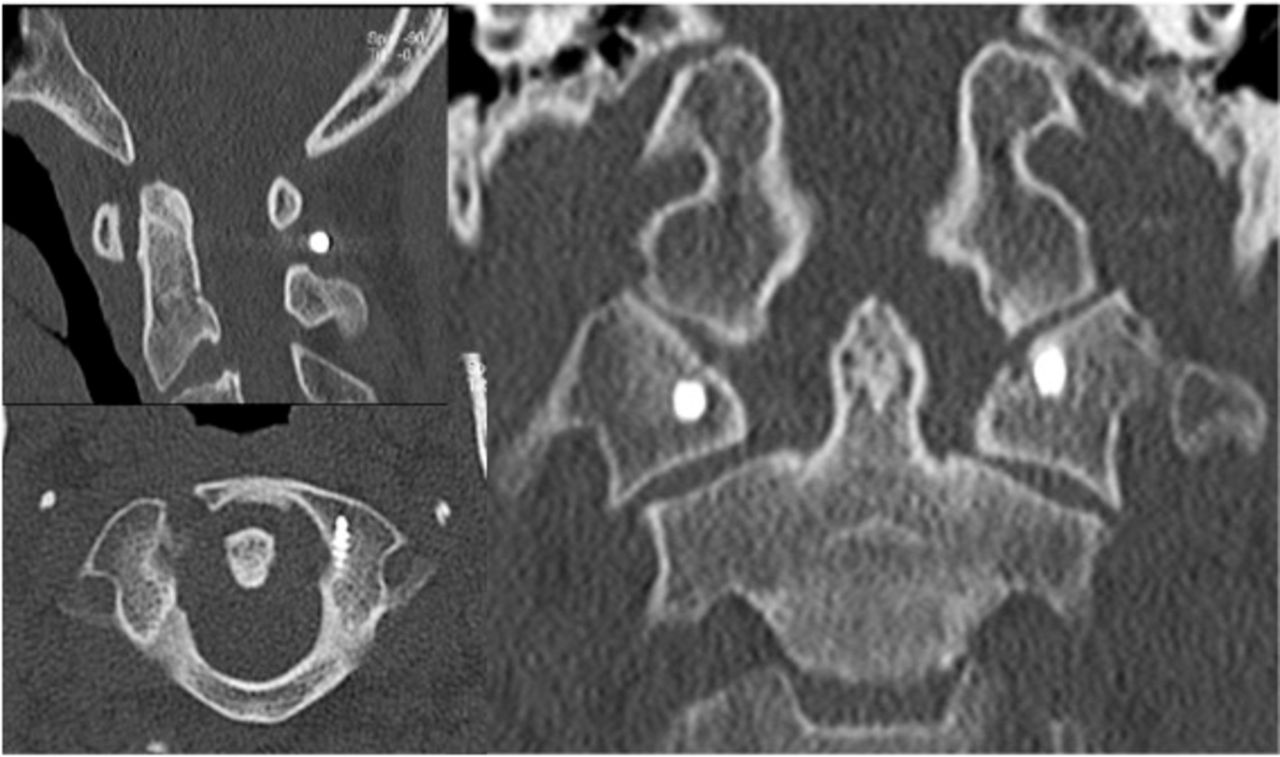
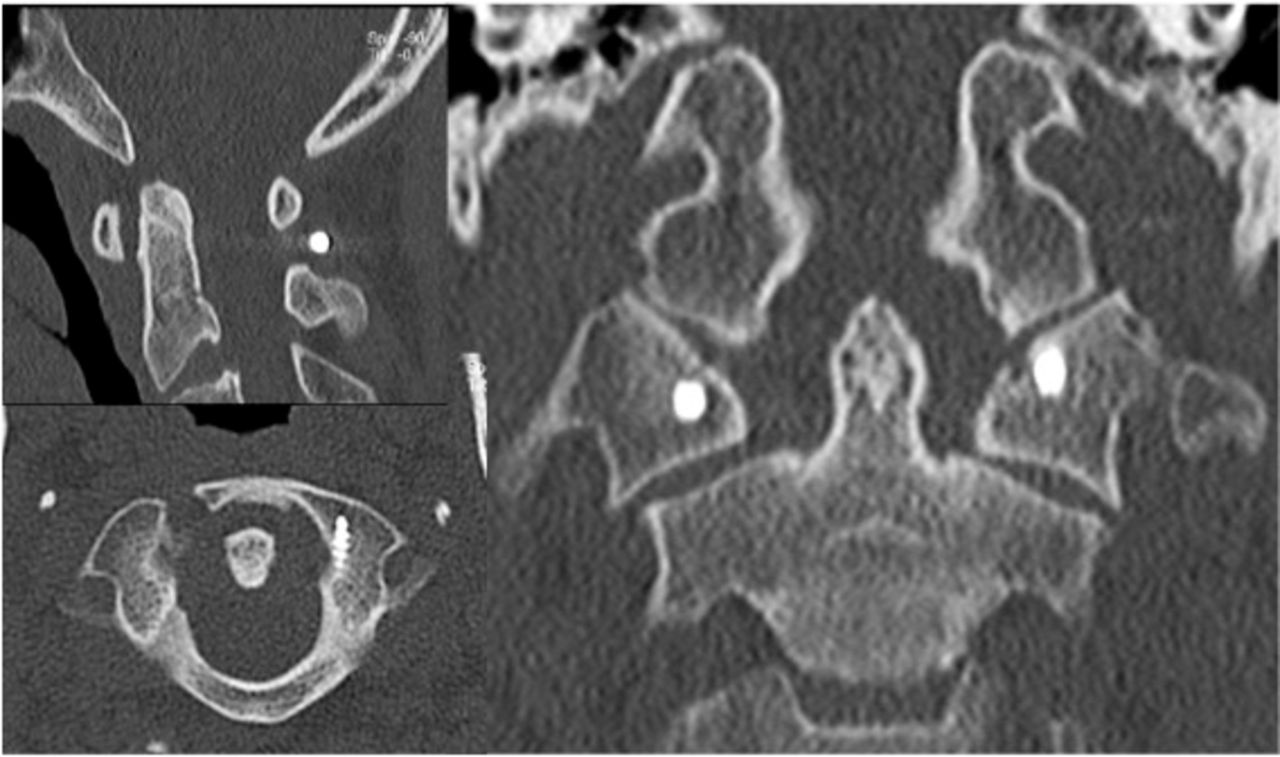
Postoperative computed tomographic scan showing the reduction of the posterior C1 ring and correction of the C1 lateral mass overhang.

Postoperative radiographs demonstrating the stability of the construct.
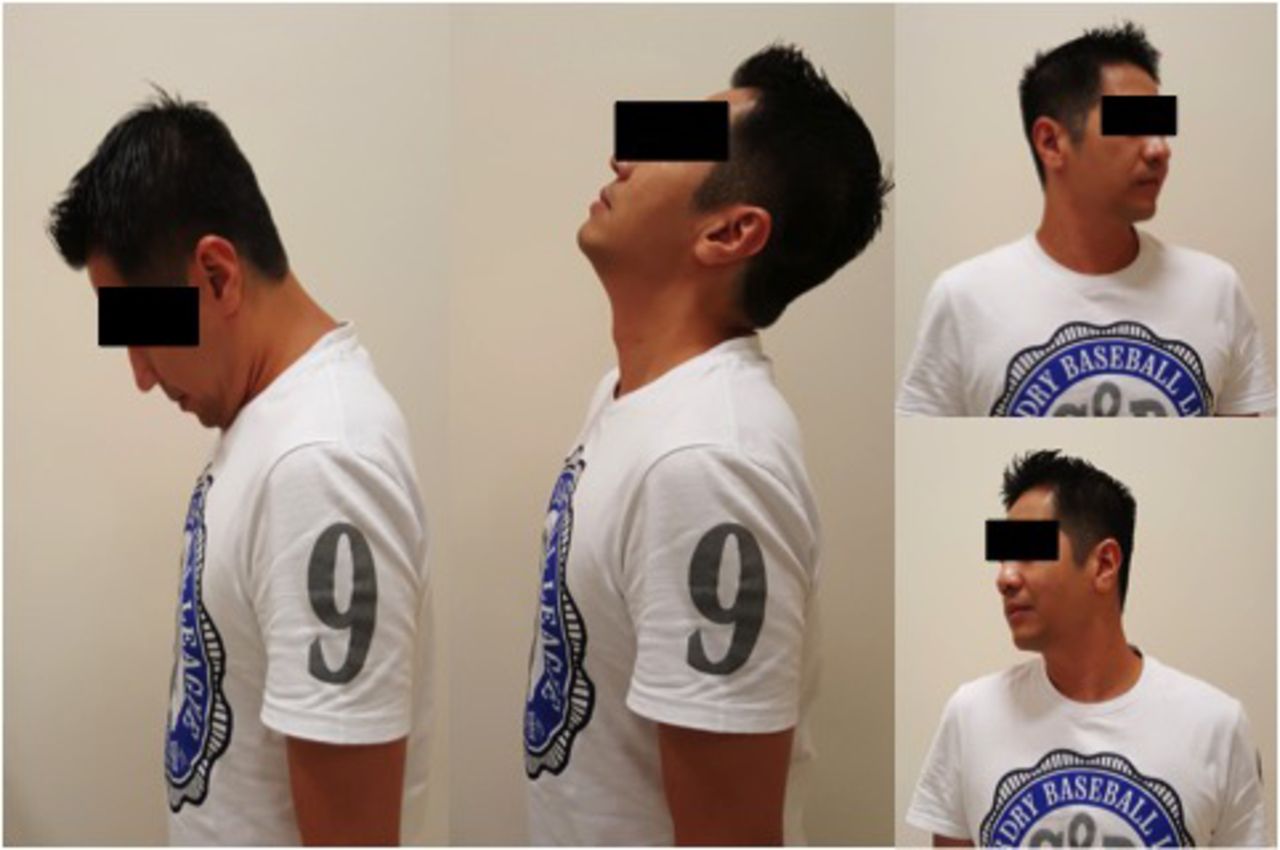
The patient made an uneventful recovery and was discharged 2 days later. The collar was worn for 6 weeks before weaning off over the subsequent 6 weeks. Follow-up radiographs were performed at 1 and 3 months along with CT scan at 3 months. At 3 months, he demonstrated near full range of motion of the cervical spine, was pain free, and had resumed driving (Figure 5). At 6 months, he returned to work as an airline steward. At 12 months, CT scan confirmed union (Figure 6). Clinically, the patient experienced slight discomfort after prolonged sitting or standing but remained painless through a full range of movement.
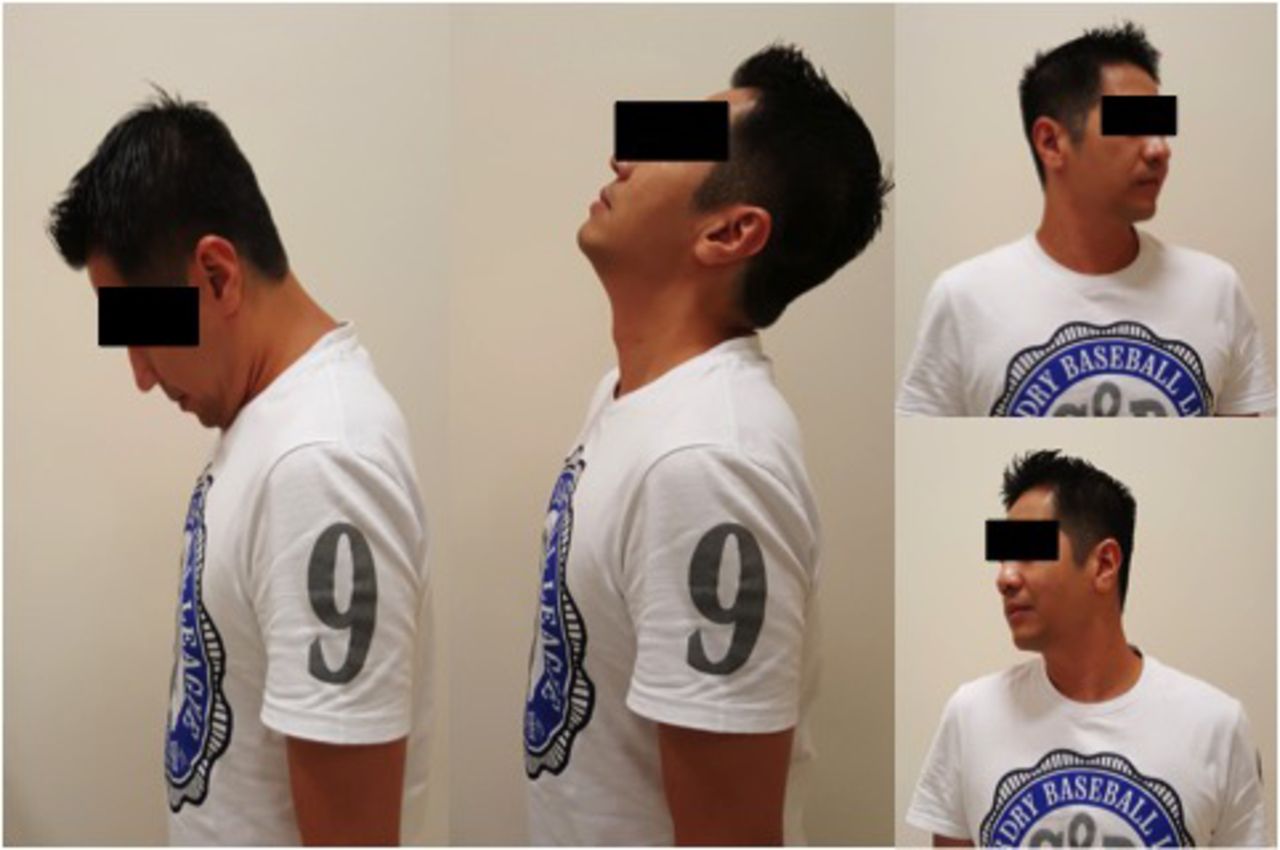
Patient showing near normal range of flexion, extension, and rotation of the cervical spine at 3 months postsurgery.
Computed tomographic scan at 1 year postoperation showing maintenance of reduction, bony union of the posterior arch, and fibrous union of the anterior arch of C1.
DISCUSSION
Neck pain is the most common presentation of Jefferson fractures. Neurological injuries are uncommon since the large diameter of the spinal canal is further widened by centrifugal displacement of fragments.4 Standard radiographs of occipito-cervical junction are often inadequate and overlook these fractures. Hence, a high index of suspicion must be maintained in patients with neck pain who have sustained axial compression injuries.
The integrity of the transverse ligament determines the stability of Jefferson fractures.1 Transverse ligament injuries are classified into intrasubstance tears (type I) or bony avulsion fractures of the ligament from C1 lateral mass (type II). Type II injuries show a promising 74% healing rate with conservative management, while type I injuries exhibit poor healing rates that warrant surgical intervention.5 An atlanto-dens interval > 3 mm or cumulative lateral mass displacement > 8.1 mm on open mouth odontoid view radiographs imply rupture of the transverse ligament and hence fracture instability6 (Figure 1).
Our case is an unstable type III atlas fracture involving both anterior and posterior arches with associated intrasubstance transverse ligament injury. It is cited to have a 33.3% prevalence of nonunion across both operative and nonoperative management.7 Other atlas fracture types and their associated nonunion prevalence are detailed in Table 1. The management of unstable Jefferson fractures is controversial. HALO immobilization is a viable option with acceptable radiographic results and low rates of nonunion or instability.8 However, the patient rejected it because of the perceived practical difficulties and inconvenience of managing it for a period of potentially up to 3 months. The 1-week delay in presentation was also taken into consideration as a risk factor for nonunion with conservative measures, thus further justifying the use of direct operative fixation.8
Types of Jefferson burst fractures.
Unstable Jefferson fractures are traditionally treated with fusion. Occipito-cervical fusion is helpful when purchase of C1 is inadequate. Unfortunately, fusions cause significant loss of range of motion, up to 52° in the flexion-extension plane and 38.9° in rotation,9 making it particularly disabling for younger patients. C1-C2 posterior fusion, though less extensive, can be challenging if the C1-C2 joint is not reduced. McGuire and Harkey10 proposed executing it with transfacet C1-C2 screw fixation to preserve motion at the occipital cervical level, but this sacrifices C1-C2 movement.
The technique employed here was direct fixation of C1 with a posterior approach. Although described before by Li et al3 and Bransford et al2 to have positive functional outcomes, it is still not widely practiced. This approach affords better exposure and provides the option of stabilizing adjacent vertebrae if necessary. The idea is to obtain stable fixation that enables the transverse ligament to heal and achieve stable fibrous union while preserving cervical spine range of motion. While no major complications have yet to be reported, the advent of surgical navigation would further minimize the risk of injuring surrounding structures with a more precise placement of screw and a less invasive approach.11
While this technique has been described before, it is still rarely utilized outside major institutions, and we hope to raise awareness of this simple technique that allows for earlier return to work and social life. We believe that using monoaxial screws along with contoured rods would allow us to reduce the anterior arch fracture more effectively, but these screws are currently not available to us.
Footnotes
Disclosures and COI: This is to declare that there are no conflicts of interest and source of funding in the writing of this case report.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2019 ISASS.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.