


Article Figures & Data
Figures
- Figure 1
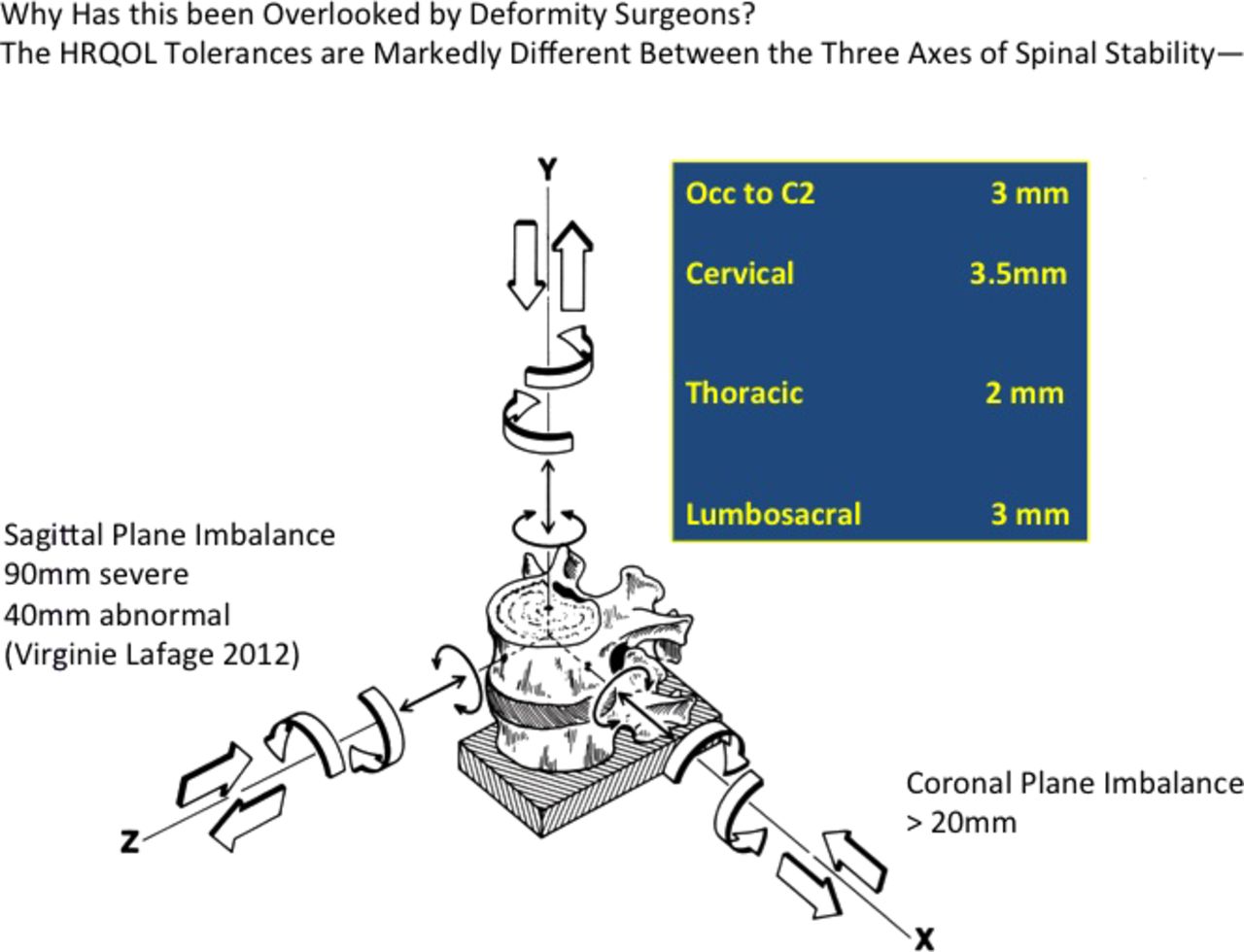
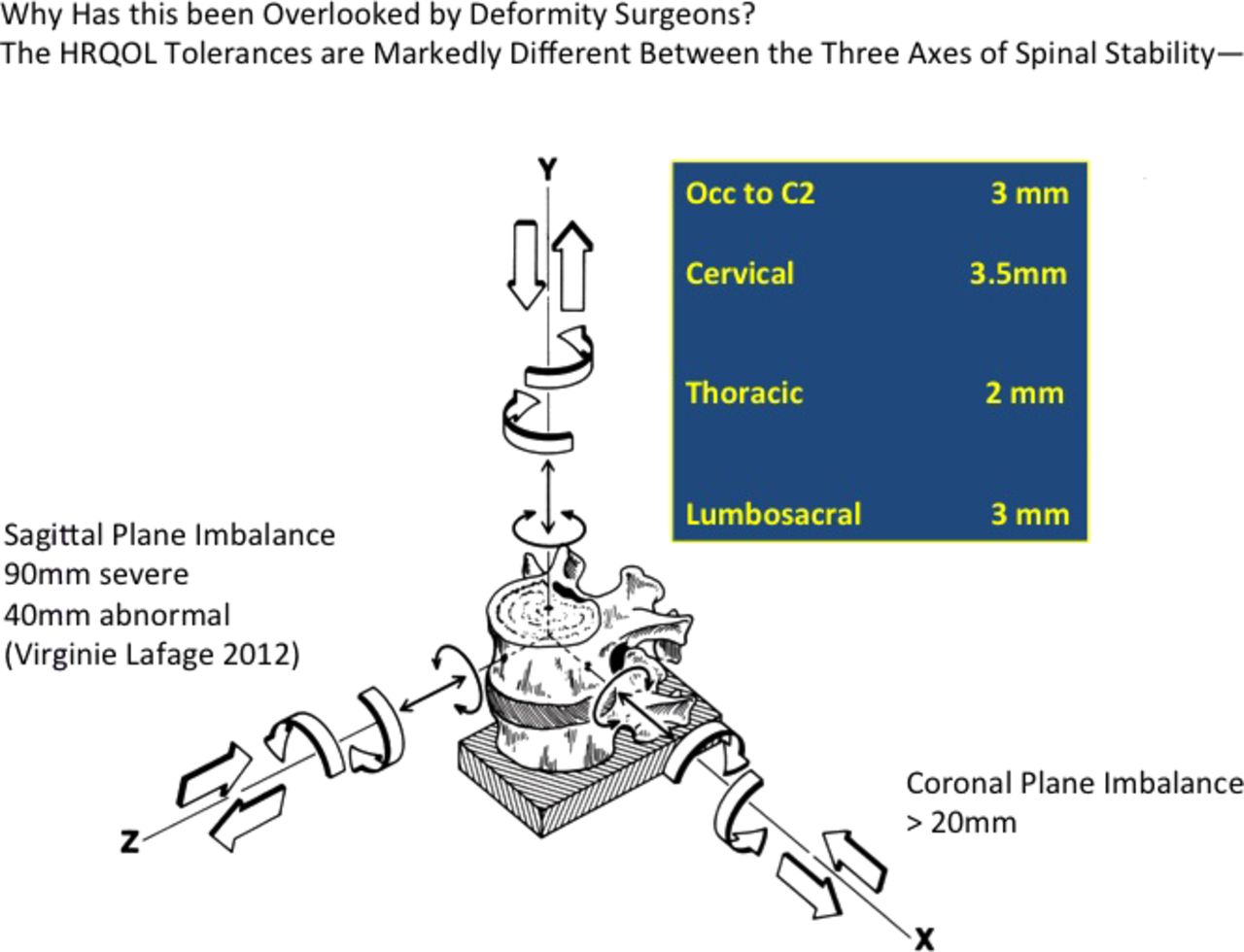
Panjabi's description of the functional spinal unit. Why has the y-axis, axial spinal height, been overlooked by deformity surgeons? (1) The axial spinal height has to be measured more accurately than sagittal or coronal balance. The Health Related Quality Of Life (HRQOL) negatively correlates with higher thresholds for sagittal balance: sagittal vertical line (SVL) is 48 mm (Lafage et al2) and coronal balance (central sacral vertical line [CSVL]) is 20 mm (Richards et al4) compared to the much smaller axial height critical numbers of 3.0 to 3.5 mm (North American Spine Society white paper10). (2) Instead of straight lines, SVL for sagittal balance (and CSVL for coronal balance), the axial height is ideally a curved line due to cervical lordosis, thoracic kyphosis, and lumbosacral lordosis. (3) Current digital planning software programs exclusively measure straight lines, plumb lines, and angles. The optimal technique quantitating axial height requires a digital software program to measure the pre-, intra-, and postoperative length of a curved line. Measurement of the middle column makes use of the redundancies of the posterior longitudinal ligament (PLL) and vertebral body malalignment; accurate measurement requires visualization of the path of the PLL.
- Figure 2
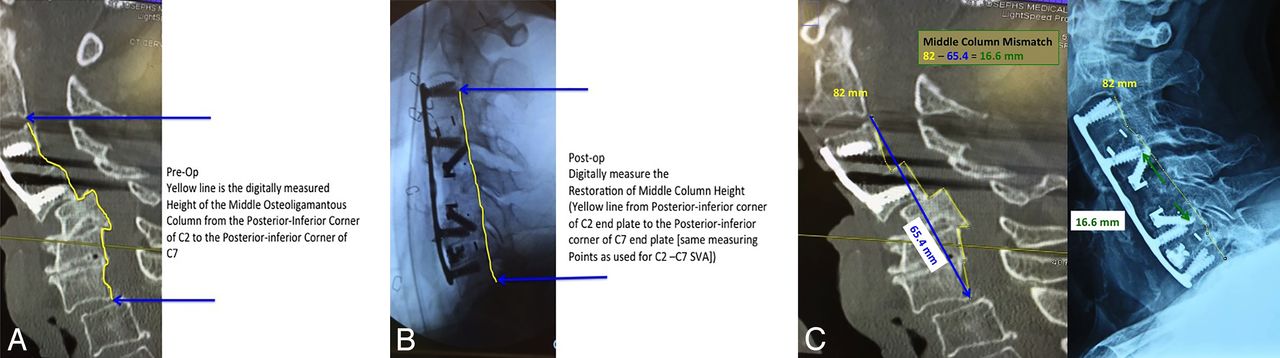
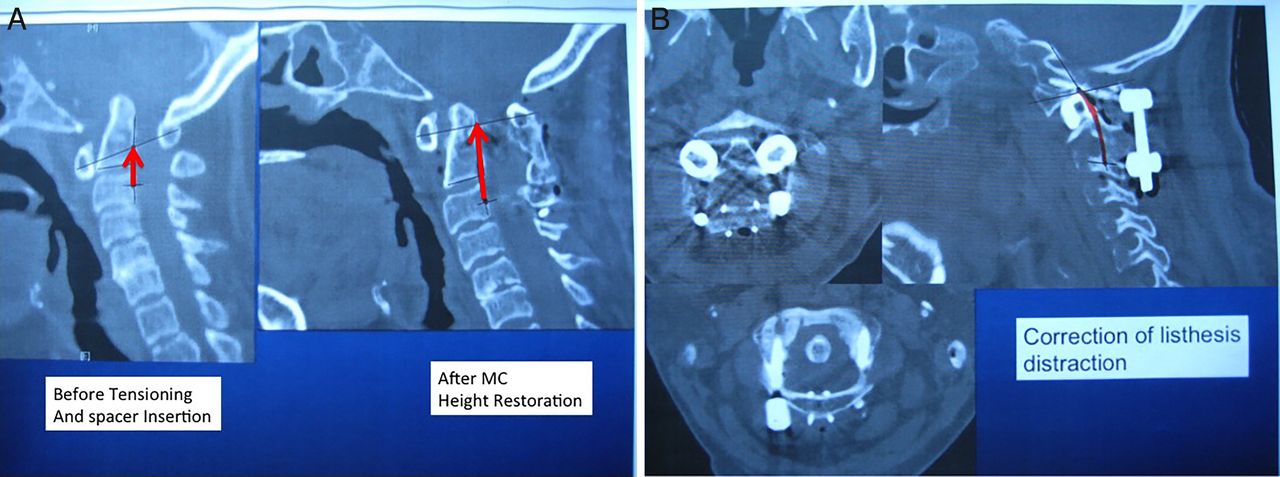
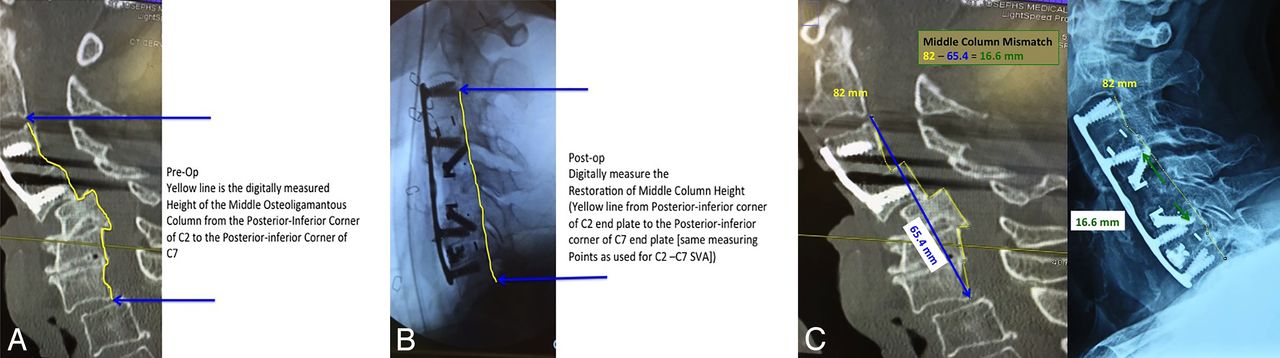
Radiographic illustrations of restoring the middle-column height in an 80-year old-woman with a complex C4-C5 and C5-C6 fracture subluxation with retropulsion of the C5 vertebral body causing Asia B paralysis. (A) Preoperative radiograph showing the measurement of the middle column illustrated as a yellow line (82 mm). (B) Postoperative radiograph after realigning the spine following C5 corpectomy, partial C6 corpectomy, and spacer insertion. The corresponding postoperative measurement of the middle column is shown as a yellow line (also 82 mm). (C) There was severe enough ligamentous disruption that the normal ligamentous tension could not be utilized to gauge correct height restoration using intraoperative distraction-type instruments (no endpoint was reached). Therefore the middle-column measurement on intraoperative radiographs was used to achieve the correct height of the reconstructed spacers. The preoperative and postoperative posterior longitudinal ligament length is shown in yellow as 82 mm. The direct straight-line measurement from the same endpoints is shown in blue as 65.4 mm. The difference between the 2, referred to as the middle-column mismatch, is shown in green: 82 mm − 65.4 mm = 16.6 mm. This means that the combined height of the middle column spacers inserted at surgery should total 16.6 mm from C2 to C7. The cervical sagittal vertical line and coronal balance was also restored.
- Figure 3
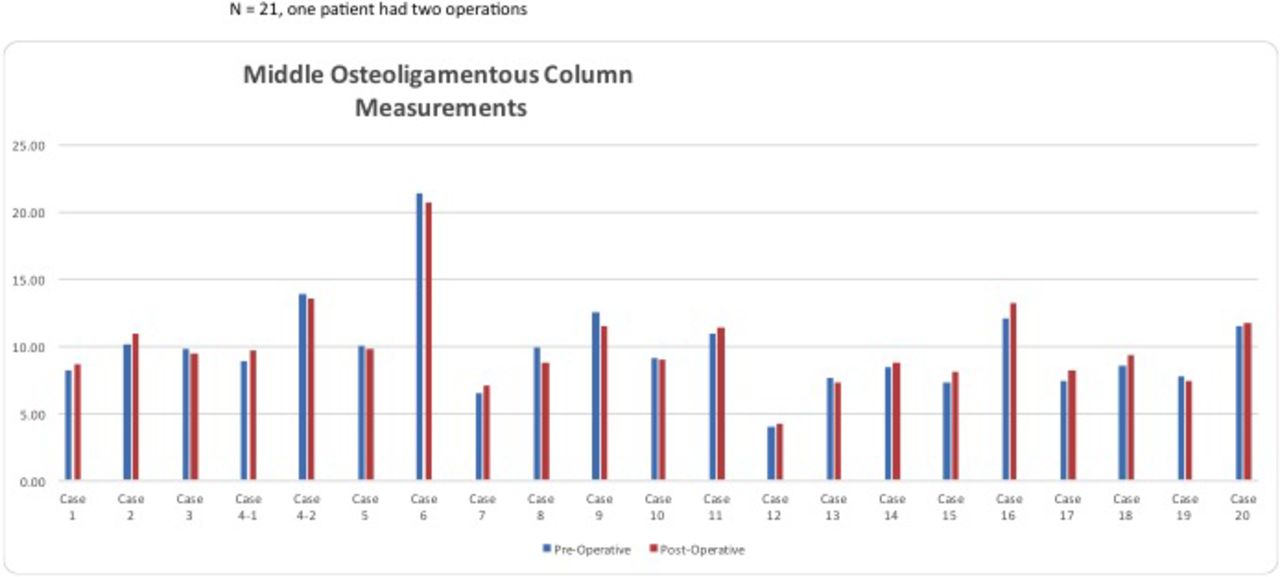
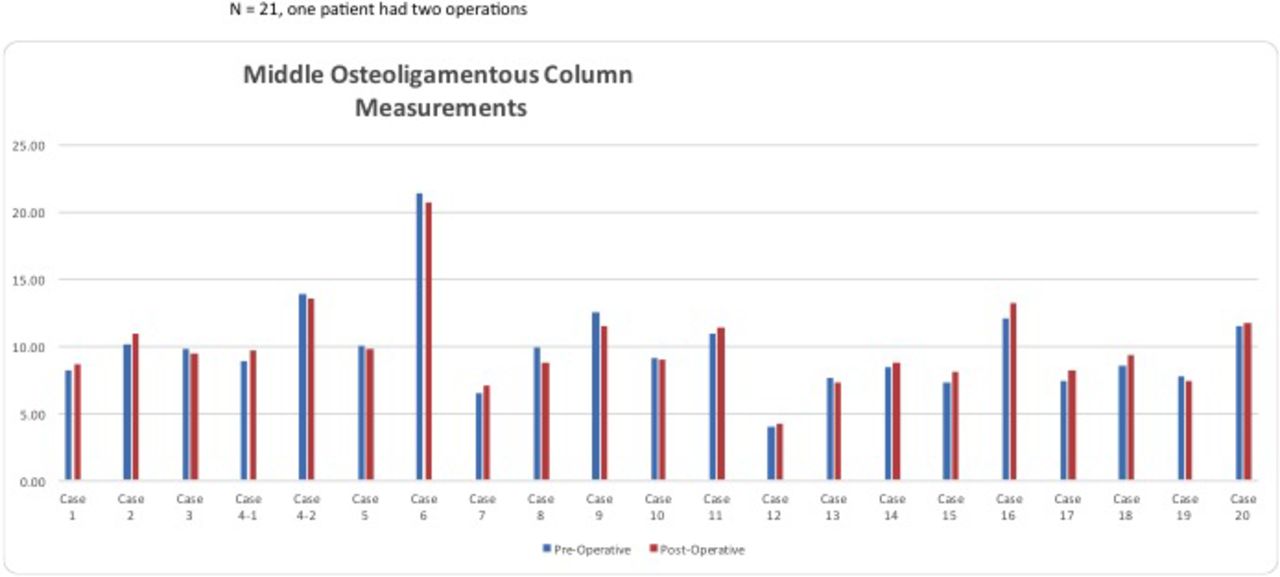
A bar graph illustrates the preoperative and postoperative measurement of the middle column using a proprietary digital mapping program capable of measuring the length of a curved line (SpineAlign). Phase 2 measurement testing of 21 consecutive patients (case 4: 2 measurements, n = 22) undergoing surgery with multilevel deformities for cervical, thoracic, and lumbar procedures had middle-column gap balancing height pre- and postoperatively measured by 3 blinded observers.
- Figure 4
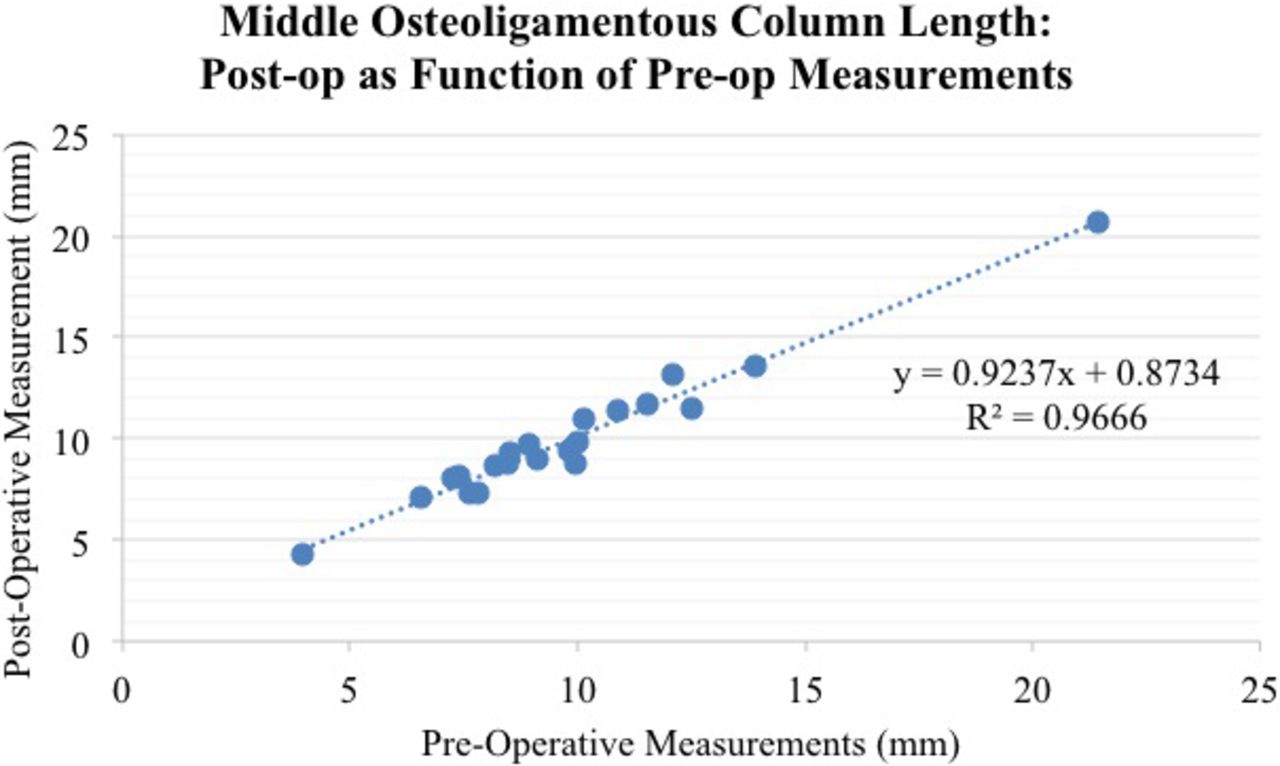
A Pearson product-moment correlation was run between each individual's preoperative and postoperative middle osteoligamentous column measurements. In total this was a consecutive series of 21 patients (case 4: 2 measurements, , n = 22) presenting with spinal deformities. There was a strong, positive correlation between preoperative and postoperative measurements, which was statistically significant (r = 0.983, n = 21, P < .01) (R2 = 0.9666).
- Figure 5
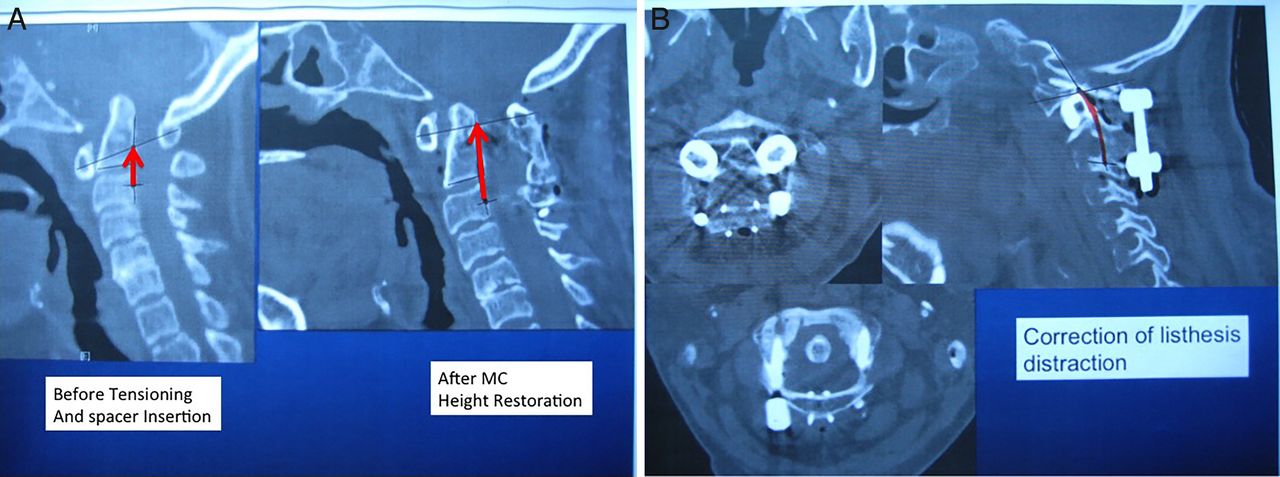
Basilar invagination from rheumatoid arthritis. (A) Ranawat's line if measured along the posterior longitudinal ligament instead of from the C2 pedicle is actually a measure of middle-column length. The red lines on the pre- and postreduction images are the length of the middle column. For consistency the distances are measured form the midportion of the C3 pedicle to the longest anteroposterior diameter of C1. Ranawat's line is the same vertical measurement, just starting from the middle of the C2 pedicle—the problem being that this is a negative number preoperatively. Our proposed site of measurement is shown before and after skeletal tong traction and reduction of 7 mm. The starting point is actually not important as long as it is consistently measured along the middle column. The starting point was determined by overlying the midportion of the C3 pedicle from the computed tomography axial image. (B) This corresponds to 7 mm of bilateral spacer reconstruction as titanium spacers were placed between the C1 and C2 lateral masses with restoration of ambulation and neurologic function.
- Figure 6
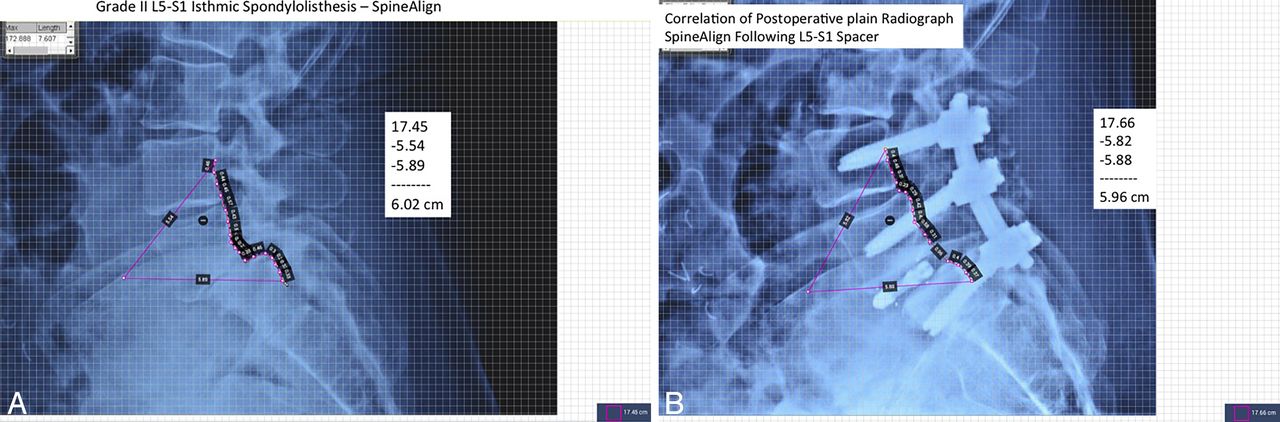
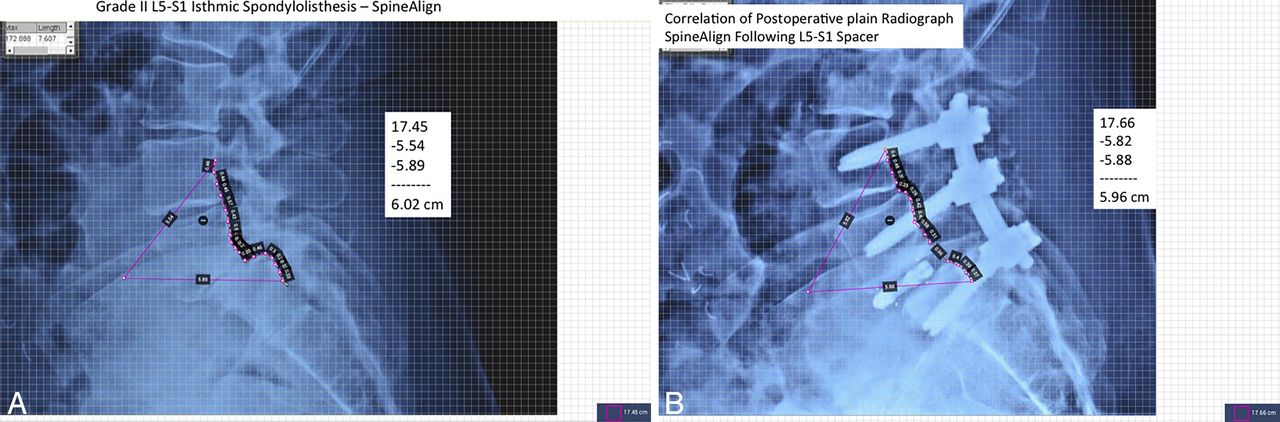
Grade II L5-S1 isthmic spondylolisthesis. (A) The preoperative height of the ligamentous portion of the middle column (posterior longitudinal ligament) was measured utilizing Spine Align, a digital software program capable of measuring a curved perimeter. The 2 extraneous portions of the closed perimeter were subtracted leaving a preoperative middle column length of 60.2 mm, measured from midpedicle of L4 to the midpedicle of S1. (B) Following posterior decompression, pedicle screw L4 to S1 instrumentation and adjustable expandable L5-S1 spacer, the middle-column height was restored to 59.6 mm, or within our acceptable target of 0.6 mm. So, postoperatively using a closed perimeter measurement, the perimeter was 17.66 cm. Therefore, if the extraneous 2 legs of the perimeter measuring 5.82 and 5.88 cm respectively are subtracted out, the curved line of the middle column is 17.66 cm − 5.82 cm − 5.88 cm = 5.96 cm. In summary, by using a spacer at L5-S1 and reducing the L5-S1 spondylolisthesis the surgery has not overstretched the middle column: preoperative measurement = 6.02 cm and postoperatively the middle column was 5.96 cm. It is hoped that even more exacting postoperative height restoration is possible with precise intraoperative digital measuring techniques.
- Figure 7
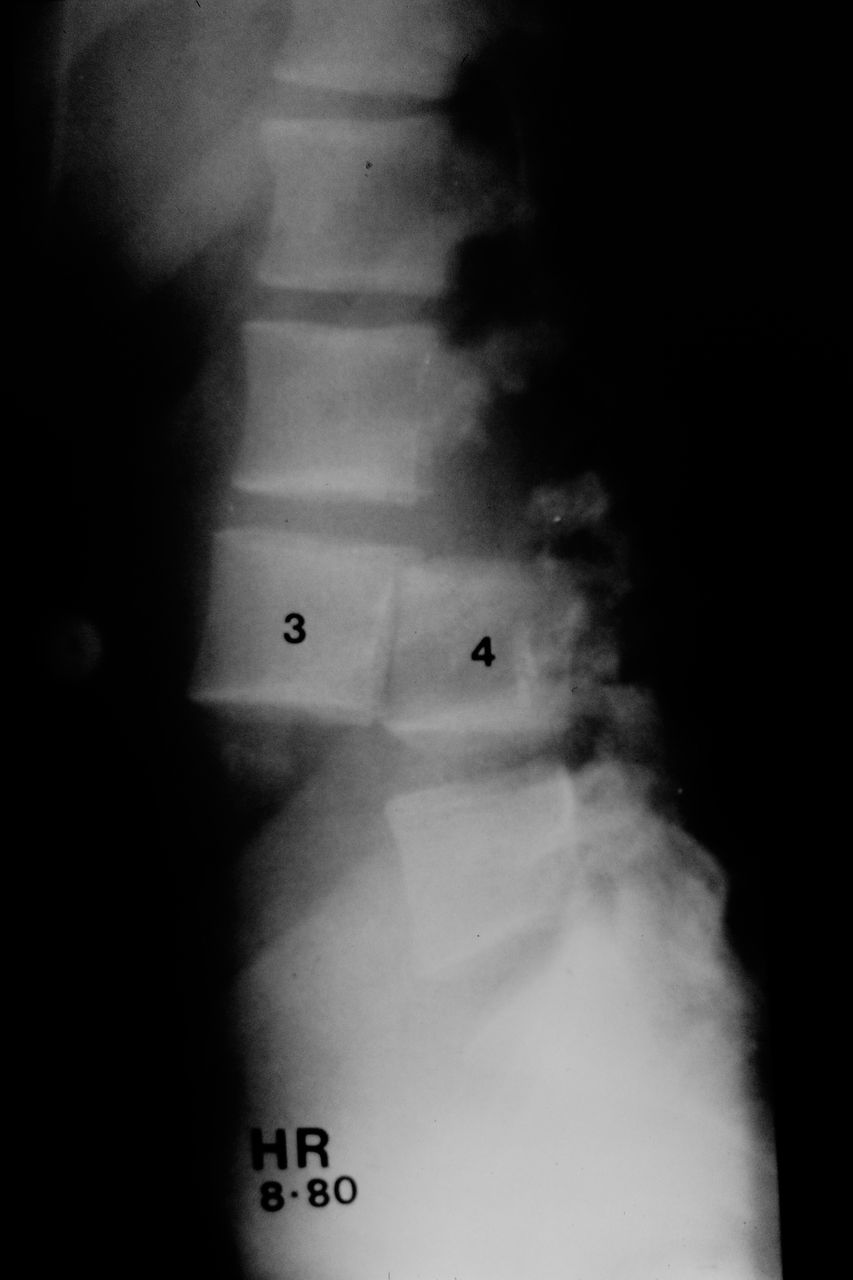
An extreme case of spinal shortening and the importance of maintenance of preservation of middle column height is shown in this 38-year-old man with a traumatic L3-L4 fracture-dislocation.
- Figure 8
The opposite extreme of axial spinal height is shown with another patient with iatrogenic overdistraction at L1 to L2 due to insertion of nonsegmental spinal instrumentation. The measurement of axial height (y-axis) correlates well with the neurologic level of function but it requires more precise measurement (an order of magnitude) compared to imbalances in the coronal and sagittal planes. This is due to the close proximity of the middle column to the neuroforamen (directly adjacent).
- Figure 9
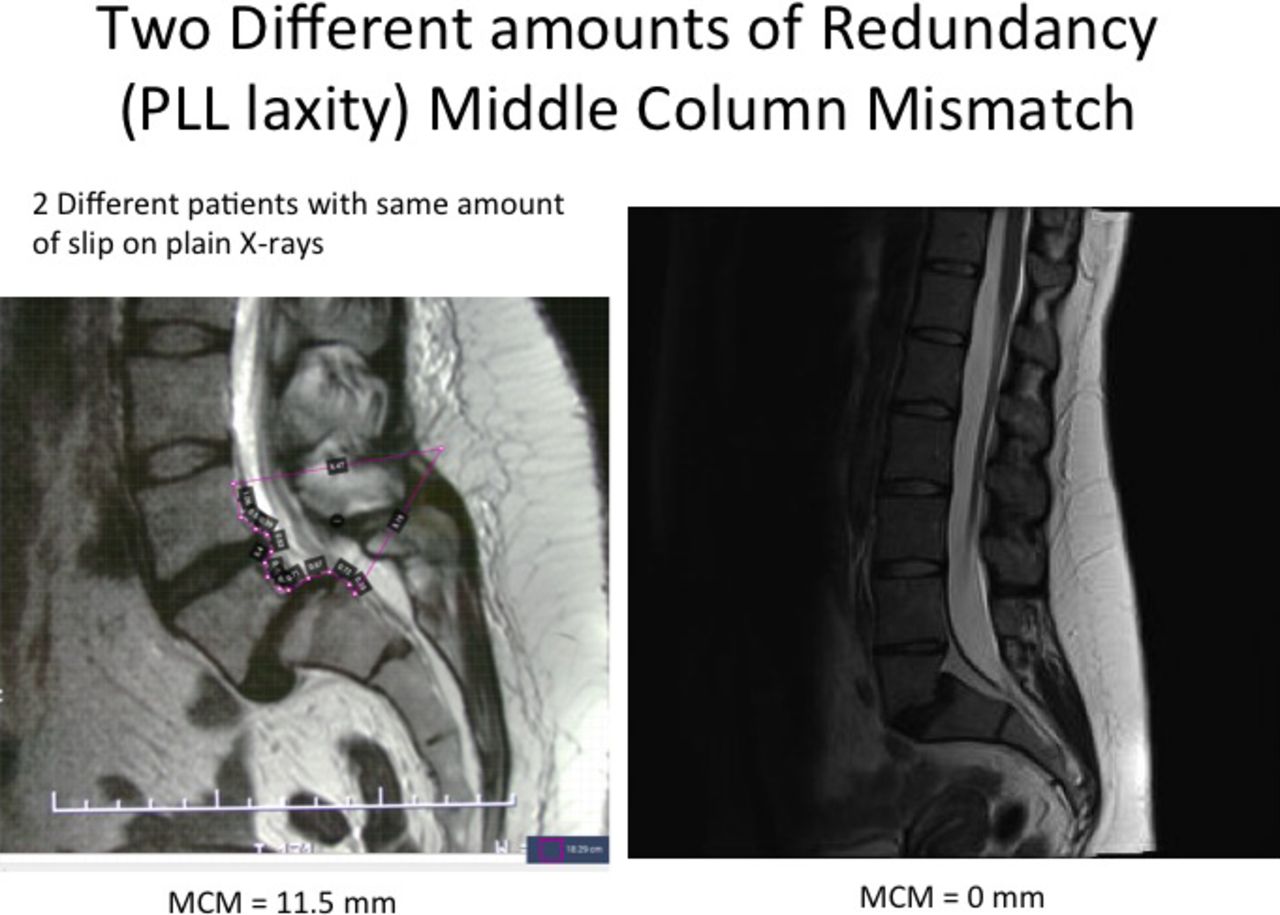
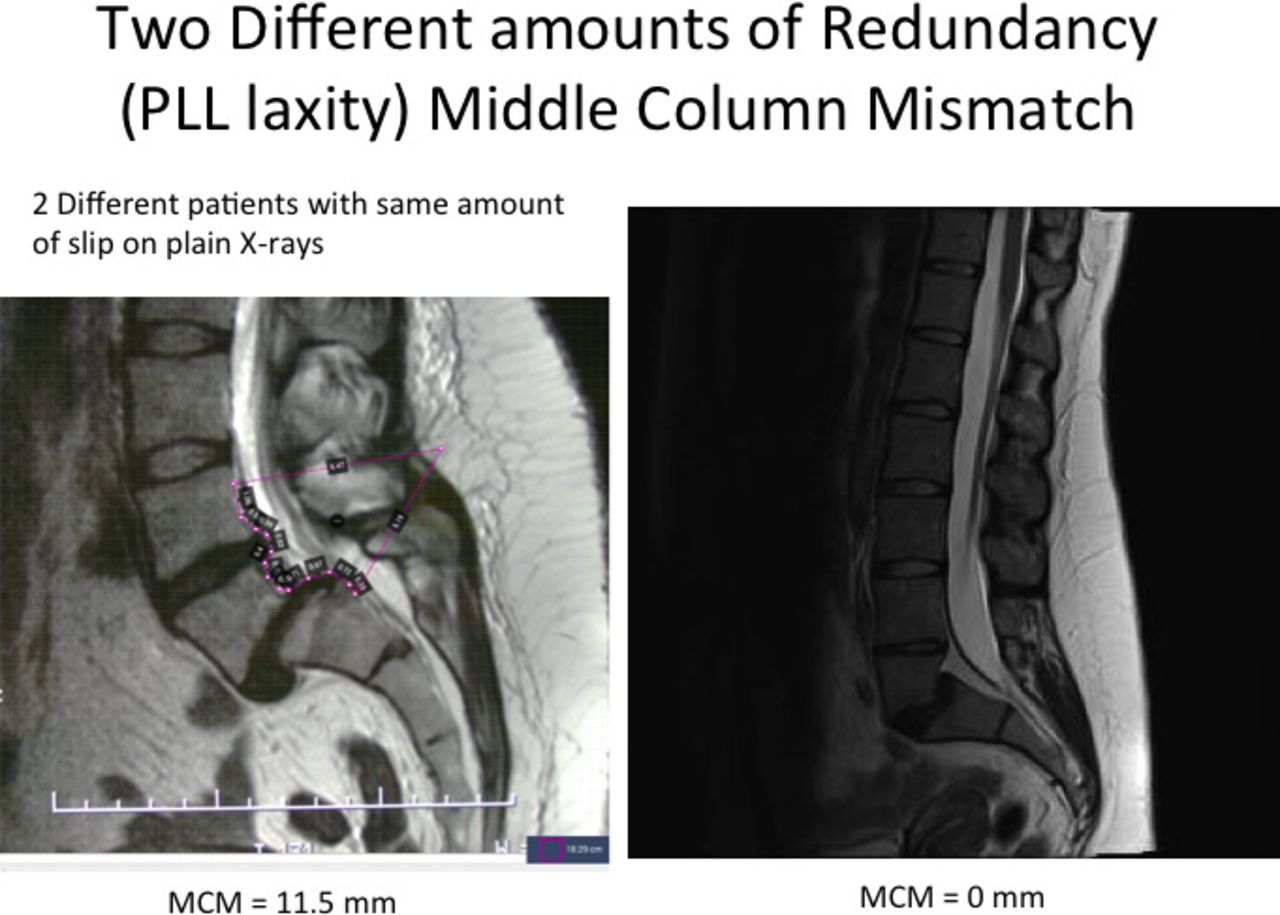
The sagittal magnetic resonance images are shown from 2 different patients, each with approximately the same degree of slippage or L5-S1 translation from spondylolisthesis apparent on their respective plain radiographs. The amount of middle-column mismatch (MCM) was calculated for each: the patient on the left had an isthmic spondylolisthesis (MCM = 11.5 mm), whereas the patient on the right had a dysplastic spondylolisthesis (MCM = 0). However, the spinal reconstruction for the patient on the left should incorporate a spacer measuring 11.5 mm in height. In contrast, the patient with dysplastic spondylolisthesis and a MCM = 0 is tethered by the nerve roots, filum terminale, and posterior longitudinal ligament. Any increase in spinal height could lead to axial stretching as there is no redundancy in the spine. Correction of the spondylolisthesis in this case should incorporate a neutral height cage equal to the amount of middle column resection in the decompressive part of the operation.
- Figure 10
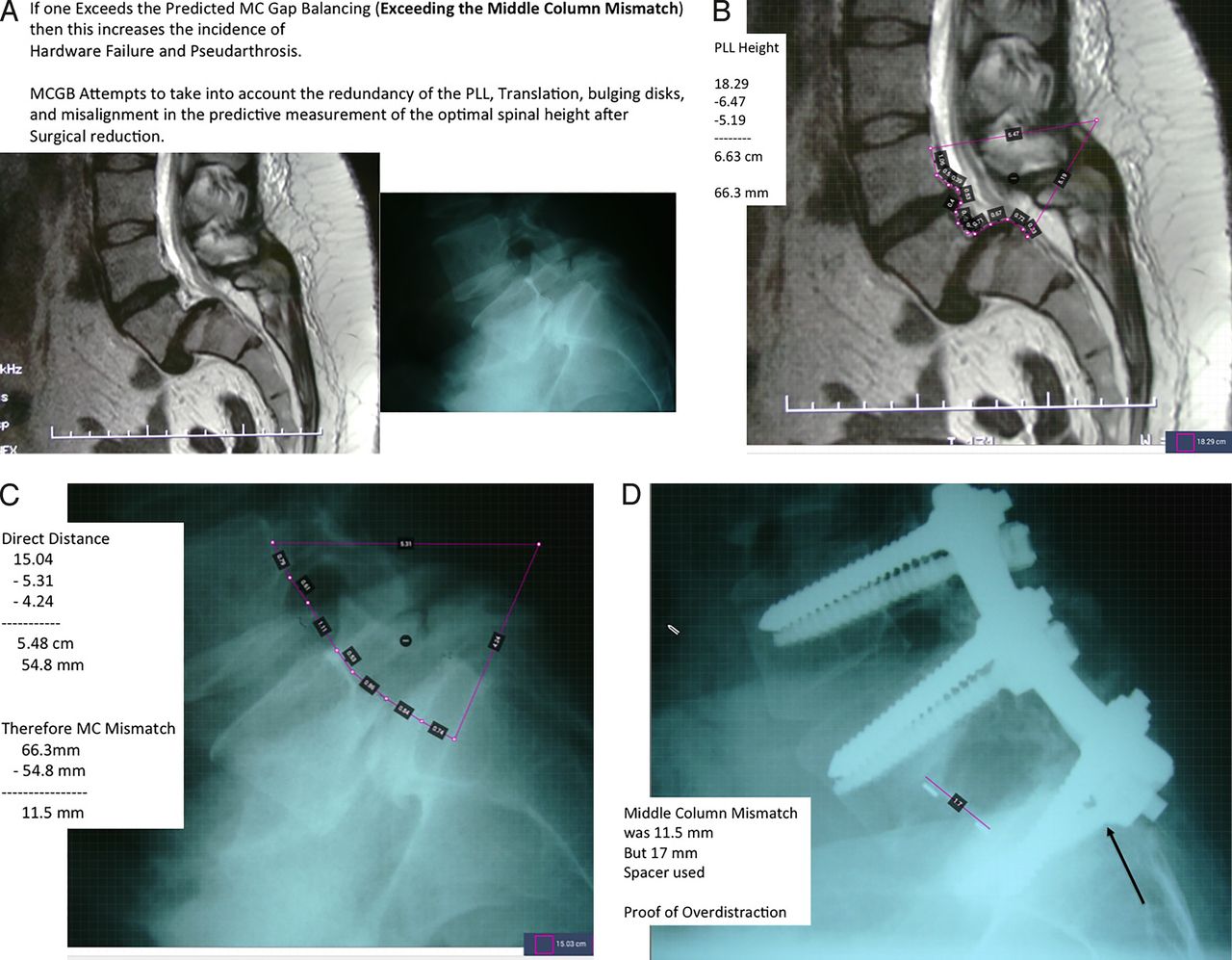
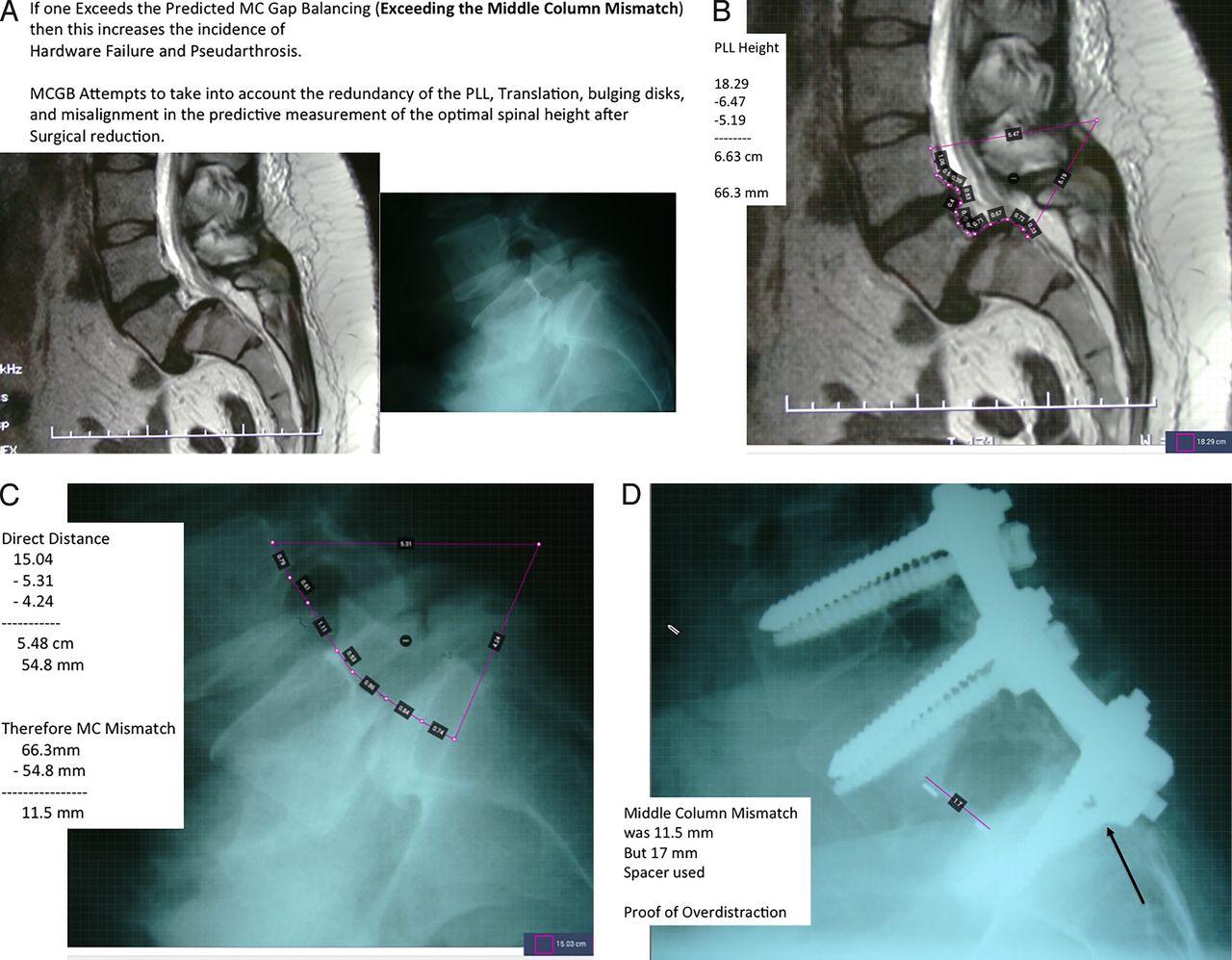
Overdistraction of the middle column. This is a patient from Elsewhere General not included in this deformity series but she presented during the time course of this study. (A) This 40-year-old woman presented with neurogenic claudication from a grade II L5-S1 isthmic spondyloisthesis. (B) The preoperative magnetic resonance image shows the length of the posterior longitudinal ligament from the midpedicle of L4 to the midpedicle of S1 = 66.3 mm. (C) The bony load-bearing components of the middle column measures 54.8 mm utilizing the same endpoints. Therefore the middle-column mismatch (MCM) = 66.3 mm − 54.8mm = 11.5 mm. (D) Unfortunately, an interbody spacer and reduction had been done elsewhere. In retrospect the spine had been overdistracted with a 17-mm-high spacer exceeding the optimal 11.5 mm MCM. She presented to us with persistent L5 radiculopathy and a broken S1 screw due to overdistraction at the time of the original surgery. A higher incidence of radiculopathy, neuropraxia, pseudarthrosis, and instrumentation failure would be expected if the optimal predictions of MCM are exceeded.
- Figure 11
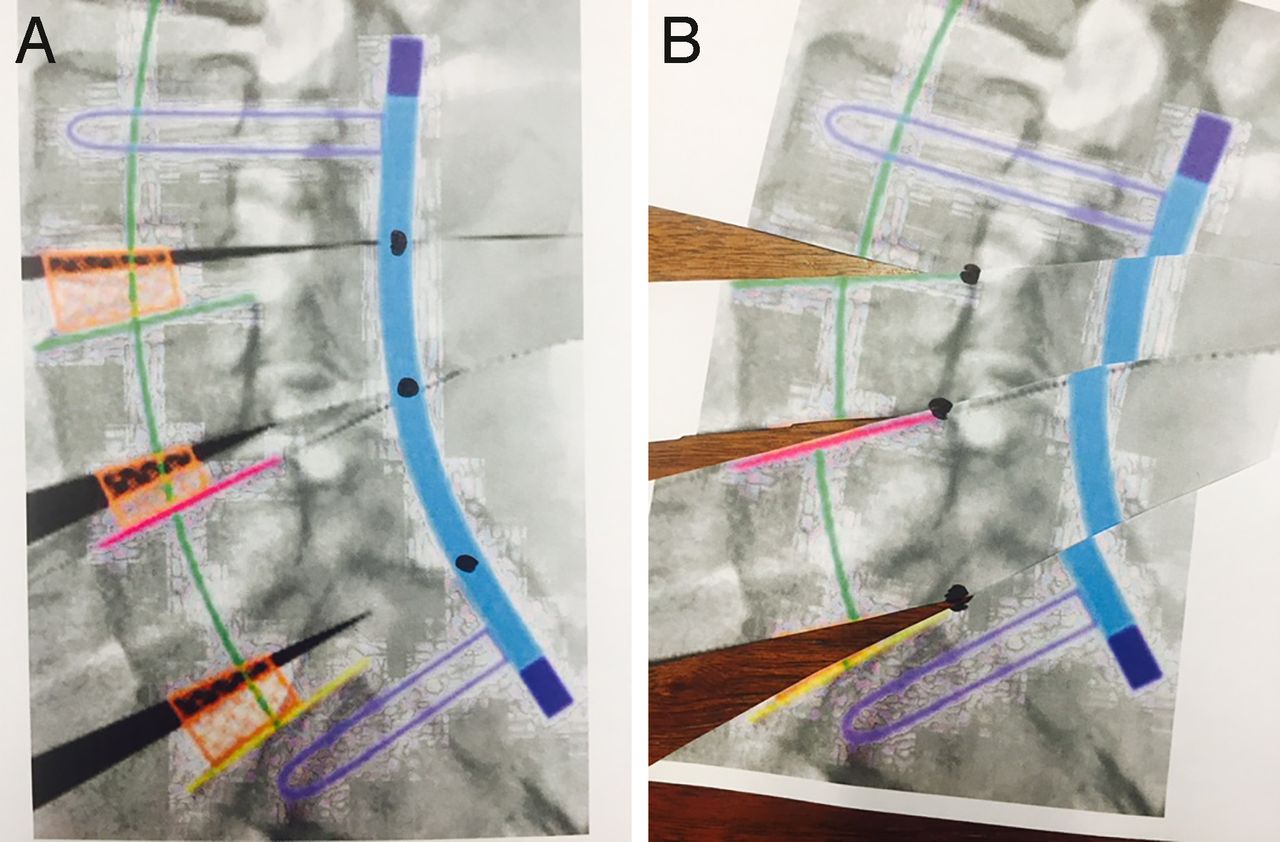
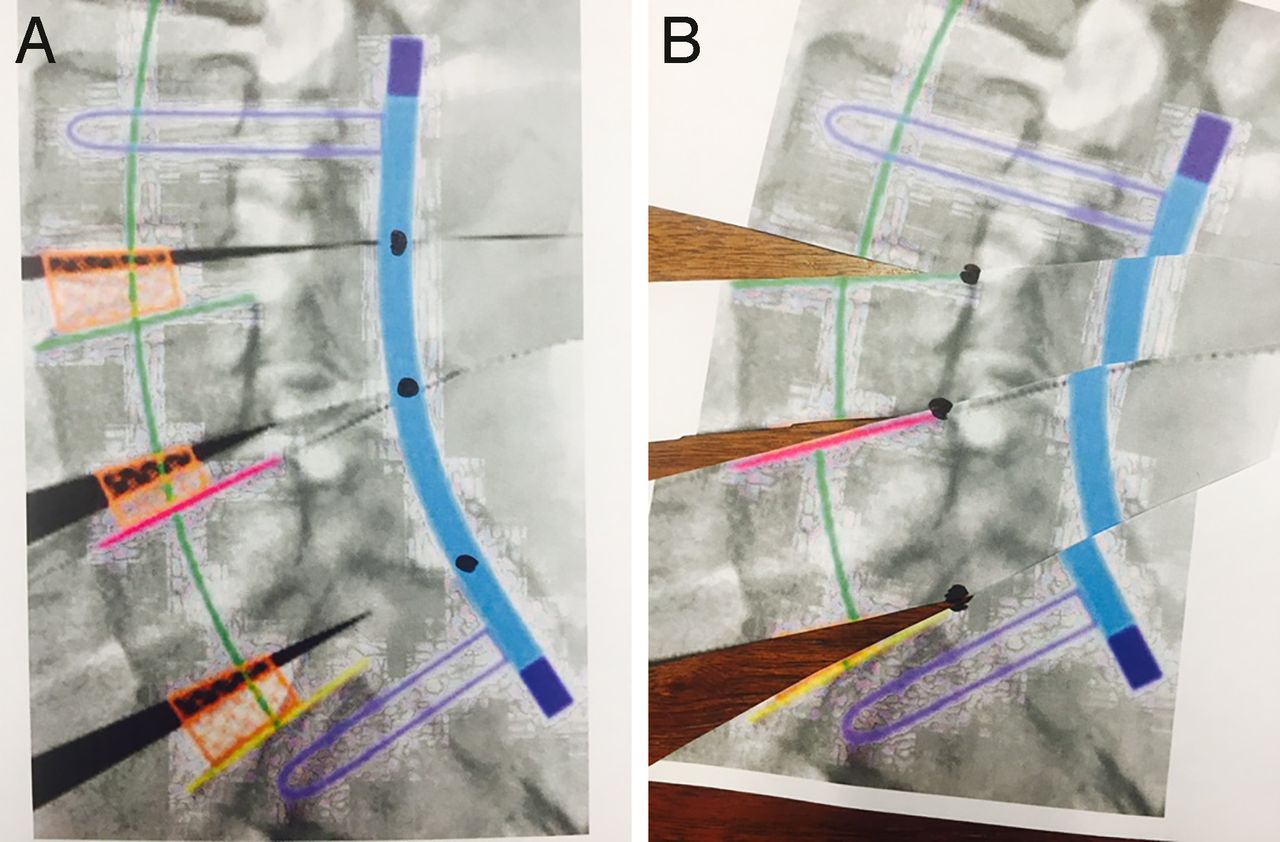
2 different preoperative planning models are illustrated in commercially available software programs utilizing DICOM images. (A) The default programs essentially cut up a JPEG in horizontal strips and rotate them along a pivot point overlying the eventual position of the posterior spinal rod. The priority of uniformly all current commercially available programs is to correct sagittal imbalance. (B) If the pivot points are moved to an alternate location, such as the middle column, the effect of inadvertent and unanticipated distortion of spinal soft tissue can be appreciated. The information on magnetic resonance imaging, computed tomography, or flexion-extension radiographs are not currently integrated into these measurements. Correct determination of cage or middle-column reconstruction requires consideration of soft tissue tension; the tension of the posterior longitudinal ligament should be considered in order to optimize neuroforaminal height postoperatively. Notice the distortion of the blue rod, which reflects the translation that must also be present in the neural canal to some extent.
- Figure 12
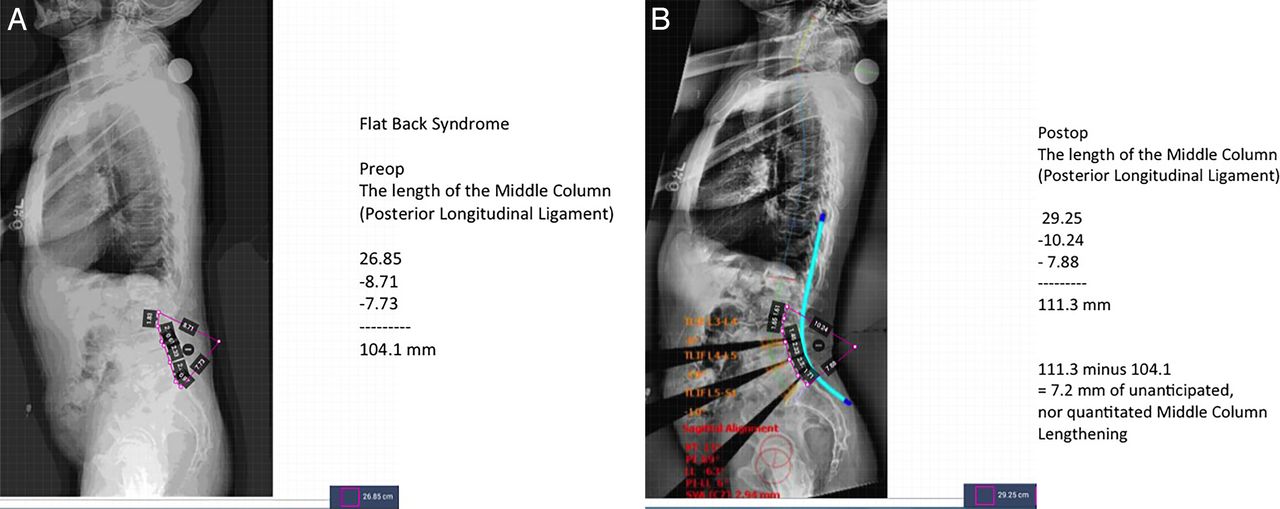
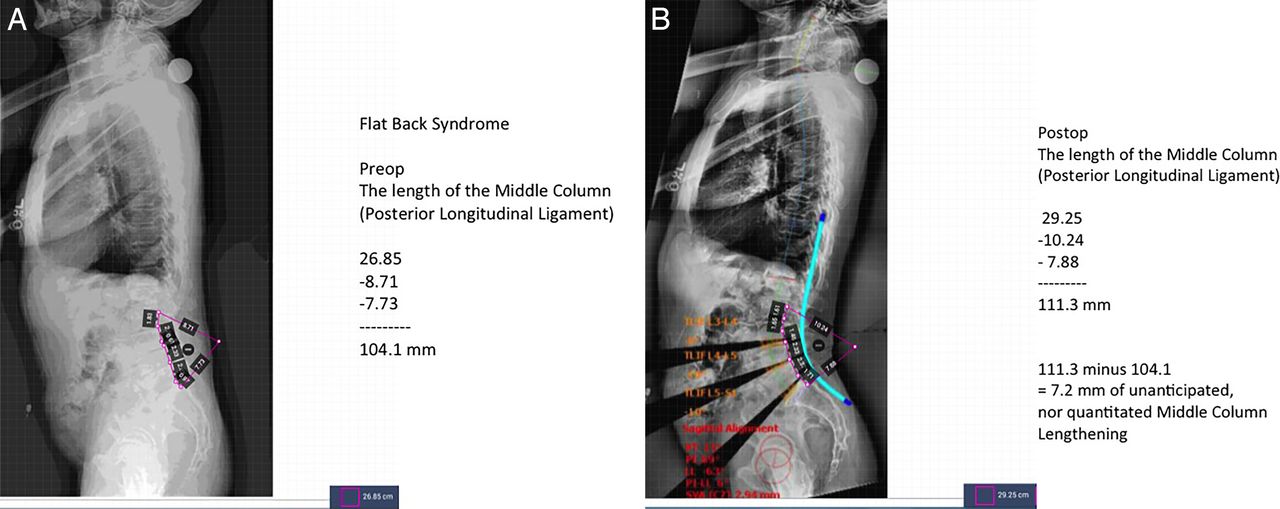
Flat back syndrome. (A) The preoperative middle-column height is 104.1 mm. (B) The postoperative middle-column height utilizing a commercially available digital mapping program measuring the same endpoints is 111.3 mm, indicating 7.2 mm of overdistraction. This may or may not create symptoms but the stretching and alteration of soft tissues, especially neural elements, needs to be appreciated—they are not integrated into the programs. The 3 triangular wedges of missing radiographic data on the lower left half of the image represent unanticipated lengthening of soft tissues.


In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.