


ABSTRACT
Background: Natural history studies have reported that the progression rate of juvenile idiopathic scoliosis (JIS) curves larger than 20° is high and tends to progress. The aim of this study was to investigate the outcome of bracing on JIS and to determine the prognostic factors on the success rate of brace treatment.
Methods: From March 1985 to February 2015, the clinical data of all JIS patients with referral age from 4 to 10 years who received brace treatment were reviewed. Those patients with a prebrace Cobb angle >20° and a Risser sign of 0 to 2 were included and followed up a minimum of 2 years after discontinuation of the brace or time of spinal fusion. The Cobb angle was recorded at the time of diagnosis, before initiation of bracing, weaning time, brace discontinuation, and final follow-up.
Results: From 297 patients with JIS, a total of 75 cases (18 boys, 57 girls) with an average curve magnitude of 31.9° at the time of diagnosis met the inclusion criteria of the study. For successfully treated patients, the average best in-brace correction was 55% for Lenke I curves, 59% for Lenke II curves, 41% for Lenke III curves, and 62% for Lenke V curves. For a total of 27 patients (36%), the brace treatment failed. Of these, 21 patients (78%) reached spinal fusion, and curves of 6 patients (22%) increased to ≥50°. The progression rate was highest in patients with Lenke type III curves (67%), and also in those with a curve magnitude of ≥46° (94%).
Conclusions: Brace treatment is an effective strategy for controlling the curve progression and avoiding spinal fusion in JIS.
Level of Evidence: 4
INTRODUCTION
The unknown scoliosis that appears from 3 or 4 years to 10 years of age is called juvenile idiopathic scoliosis (JIS)1–6 and is observed in 8% to 21% of all types of idiopathic scoliosis (IS) cases.2,7,8 The male to female ratio of JIS varies across the ages of manifestation and ranges2,9 from 1:1.6 to 1:4.4. Natural history studies have reported that the progression rate of JIS is higher than that of adolescent idiopathic scoliosis.10
Observation and bracing are the most common types of nonsurgical treatment for JIS patients. Precise observation at intervals of every 4, 6, 9, and 12 months is the strategy chosen for patients with a Cobb angle of less than 20°.5 Bracing is indicated for those patients with progressive curves larger than 20°. However, the effectiveness of bracing for JIS is controversial.
Rates of success with the brace treatment for JIS were reported1–3,11–15 as 12.5% to 95%; due to the dissimilarity of the research method, follow-up duration, and heterogeneity of the patients, the results of these studies are not conclusive. Therefore, the aim of the present study was to investigate the long-term results of bracing in JIS up to 2 years after completion of brace treatment or spinal fusion. Evaluation of prognostic factors that can be involved in the effectiveness of bracing such as initial curve magnitude,16 curve type,15 best in-brace correction (BIBC),17 and brace compliance18 has been another goal of this study.
MATERIAL AND METHODS
Patients
This was a case series retrospective chart review study conducted in the senior author's (M.S.G.) spine clinic. Before initiation of the study, ethics approval was obtained from the ethics committee of Iran University of Medical Sciences. From March 1985 to February 2015, the clinical data of all patients with JIS who received brace treatment were reviewed. The inclusion criteria of the study were as follows: referral age from 4 to 10 years, prebrace Cobb angle >20°, Risser sign 0 to 2 at initiation of bracing, followed up to the end of skeletal maturity on the basis of a Risser sign >4, completion of brace treatment, no history of prior surgical treatment, a minimum of 2 years of follow-up after completion of brace treatment, and having complete x-ray data from initial visit until skeletal maturity or surgical intervention. All patients with missing records or radiographs during brace treatment and follow-up, those who discontinued brace treatment before skeletal maturity, and the patients under treatment as well as skeletally immature patients were excluded.
All radiographical parameters were measured and recorded by the senior author (M.S.G.) using 1 protractor to minimize interobserver variability.19 In addition, all clinical records were surveyed by the first author (T.B.).
The primary goals of bracing for JIS are halting the curve progression and delaying surgical intervention during the growth period of patients. Therefore, for JIS patients with a curve severity of >45°, brace treatment is often prescribed to lessen the risk of rapid curve progression and to delay spinal fusion.
Brace Treatment
During chart review the following information was recorded: (1) gender, (2) age (at baseline, before bracing, menarche, before surgery, weaning from brace, discontinuation of brace, and skeletal maturity), (3) scoliosis Cobb angle (at baseline, before bracing, best in-brace, before surgery, weaning from brace, discontinuation of brace, and final follow-up), (4) brace wearing time, (5) brace type, and (6) brace compliance. Best in-brace correction (BIBC) was determined according to the description of Jarvis et al.20 During the brace treatment and at each routine visit of the patients (at intervals of 4 to 6 months), the physician recorded the brace compliance via asking the patients and the appearance of the brace. The patients were classified into 2 groups based on compliance rate: (1) full compliance (those who had been wearing the brace for >20 hours a day) and (2) partial compliance (those who had been wearing the brace for <20 hours a day).
The Lenke classification system was used to explain the type of the curve.5 Before bracing, Cobb angles were classified into 3 groups (≤29°, 30° to 45°, and ≥46°) to evaluate the outcome of bracing based on curve type and curve magnitude. In all patients, the largest curve at baseline was considered for statistical analysis. The bracing was considered successful if the curve magnitude at final follow-up measured <50°.21
To report this case series, we used preferred reporting of case series in surgery guidelines.
Statistical Methods
Statistical calculations were performed using SPSS software, version 17 (SPSS Inc, Chicago IL), and GraphPad Prism software for Windows, version 8 (GraphPad Prism Software Inc, San Diego, CA). To describe the characteristics of the patients, descriptive statistics (mean, standard deviation, and range) were used. For nominal variables, the χ2 test and for continuous statistics the independent sample t test were run. The analyses were performed between the success/stable and progression/surgery groups. A Friedman test was applied to evaluate the changes in the curve size across the different time periods of brace treatment. A P value of less than .05 was considered statistically significant.
RESULTS
Patients
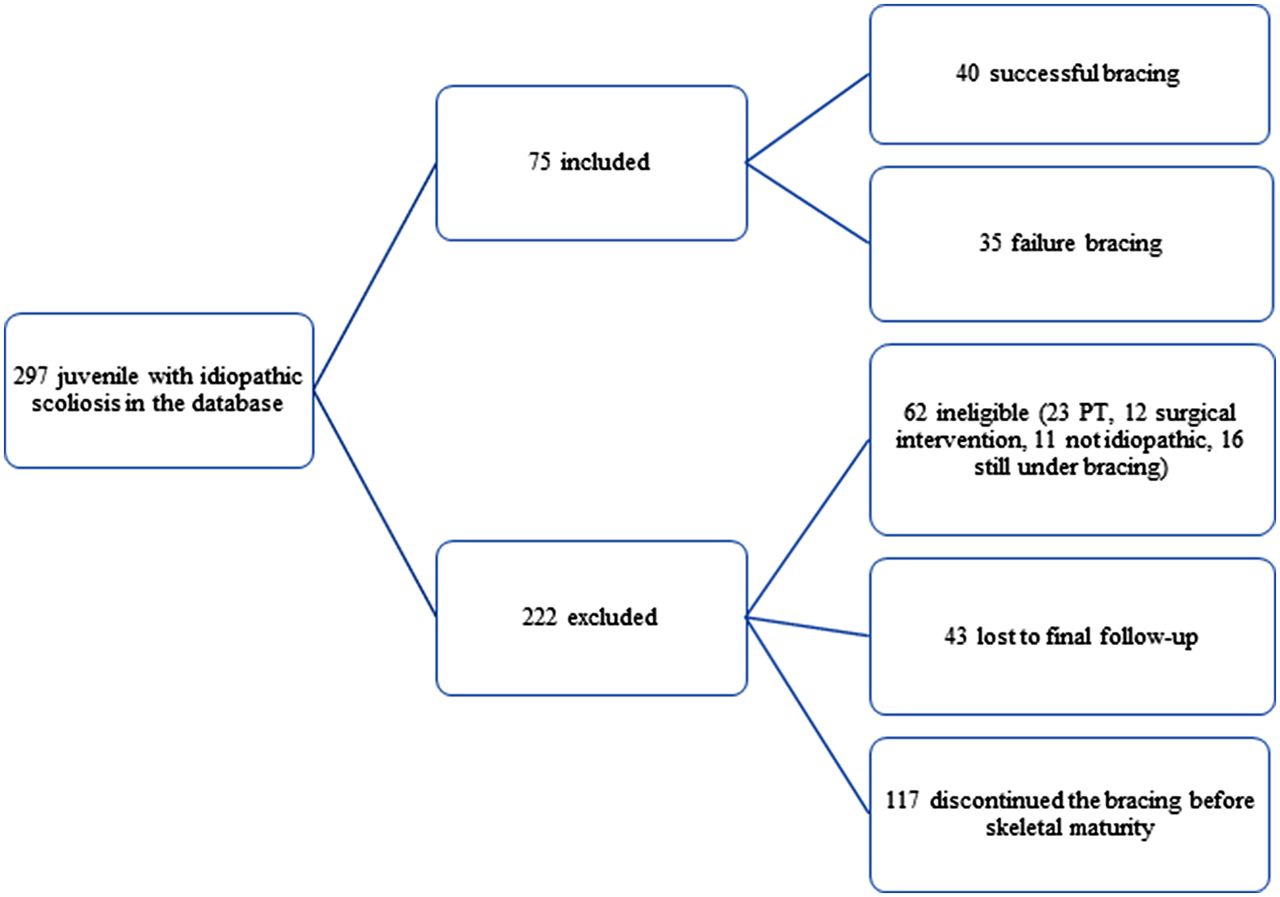
From 297 patients with JIS, 222 patients were excluded. Of these, 23 patients were treated by physical therapy, 12 patients had surgery, 11 patients did not have IS, 16 patients were still under treatment, and 43 patients were lost to final follow-up, and 117 patients discontinued the bracing before skeletal maturity (Figure 1). Finally, a total of 75 patients (18 boys, 57 girls) with a mean age of 6.94 ± 1.86 years at the time of diagnosis met the inclusion criteria of the study. Of these, 66 patients (88%) were treated with a Milwaukee brace, and the other 9 (12%) were treated with Thoracolumbosacral orthosis. The girl to boy ratio was 3.1:1. Table 1 shows the baseline and prebrace characteristics of the patients.
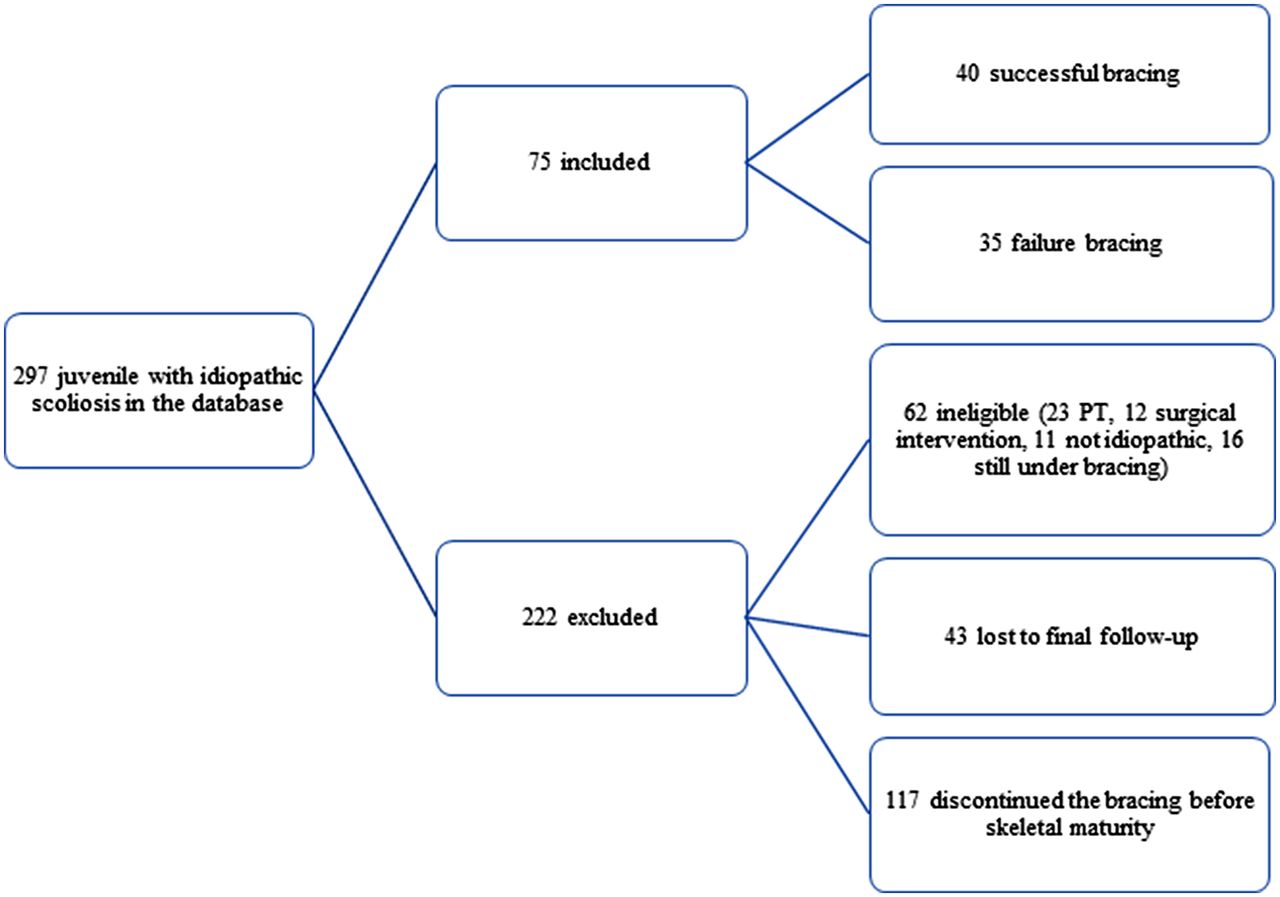
Flowchart describing the eligible and ineligible patients in the present study.
Characteristics of the entire patient sample at baseline and before initiation of bracing.
Bracing Outcome
Characteristics of the patients at different stages of brace treatment between the success/stable and progression/surgery groups are reported in Table 2. In total, bracing was successful for 48 patients (64%). Among successfully treated patients with JIS, 25 patients had been braced at their juvenile period and 23 at adolescence. The mean age, thoracic kyphosis angle between T2 and T12, scoliosis Cobb angle, Risser sign at initiation of bracing, follow-up duration, and brace wearing time of these patients are outlined in Table 3. The overall effectiveness of brace treatment was 88% (24/27) when bracing was initiated during adolescence, which significantly decreased to 54% (26/48) when bracing was initiated during the juvenile period (P = .01).
The mean age, Risser sign, and scoliosis Cobb angles at different stages of brace treatment between the success/stable and progression/surgery groups (n = 75).
Results of the patients with stable/improved curve (n = 48).
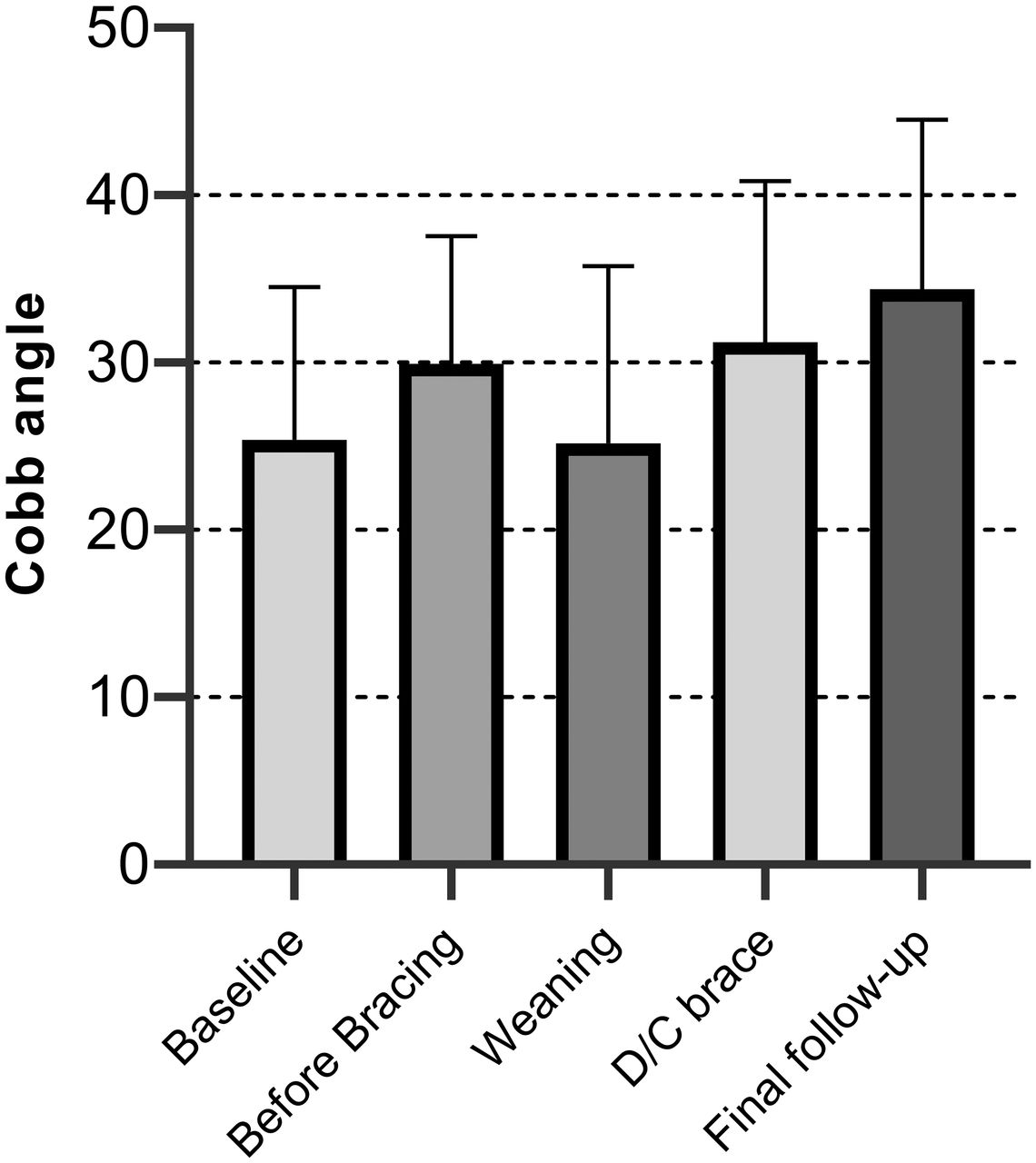
Figure 2 summarizes the Cobb angle values across 5 time periods (baseline, before bracing, weaning, brace discontinuation, and final follow-up). The results of the Friedman test showed that there was a significant difference in Cobb angle values across these 5 time periods (χ2 = 57.59, P <.001). Survey of the median values indicated a decrease in Cobb angle values from initiation of bracing (median = 28°) to weaning (median = 25°). However, the Cobb angle values increased from weaning to discontinuation of bracing (median = 30°) and showed a further increase at final follow-up (median = 35°).
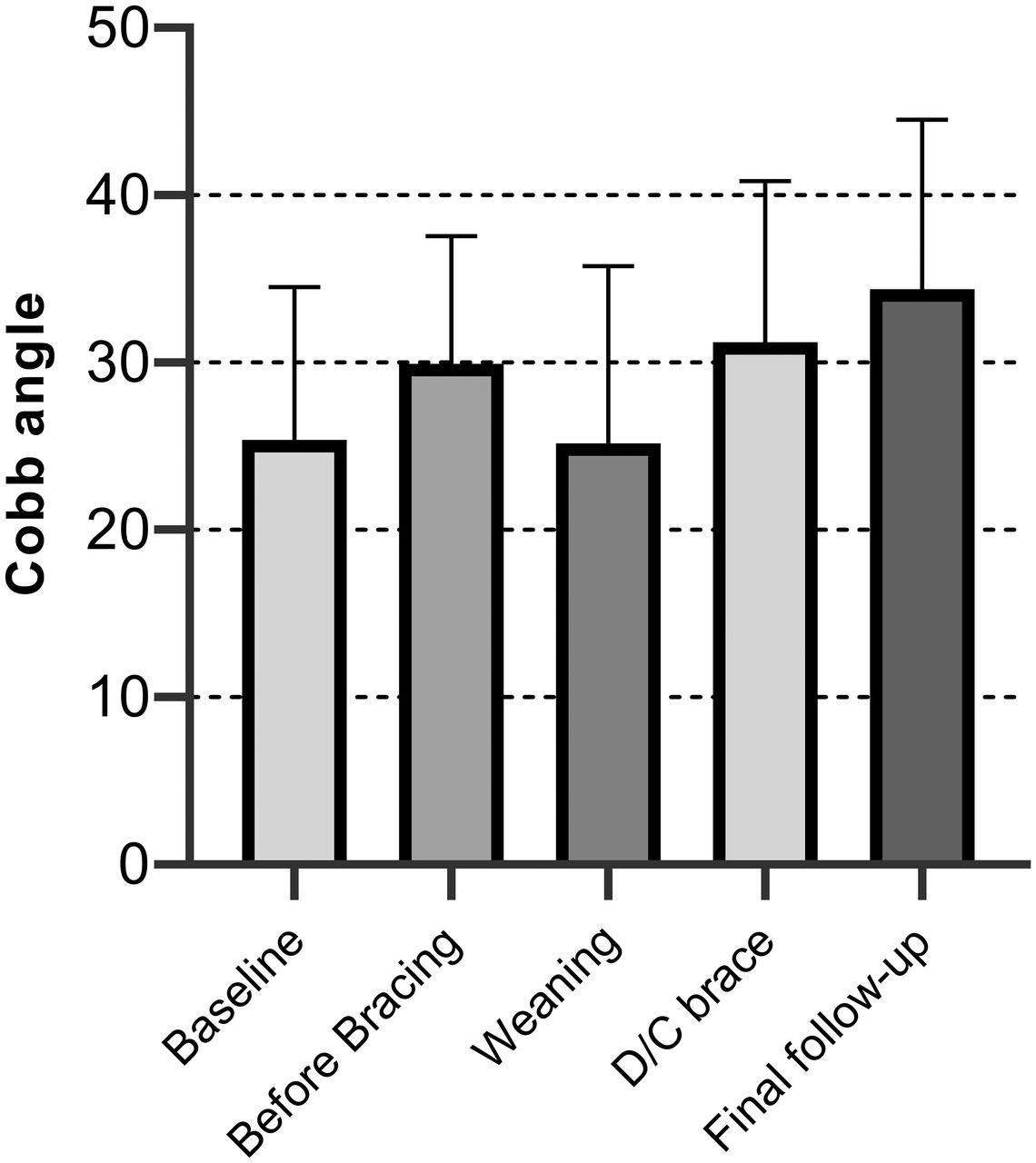
The Cobb angle values across 5 time periods of brace treatment (baseline, before bracing, weaning, brace discontinuation, and final follow-up).
Brace Compliance
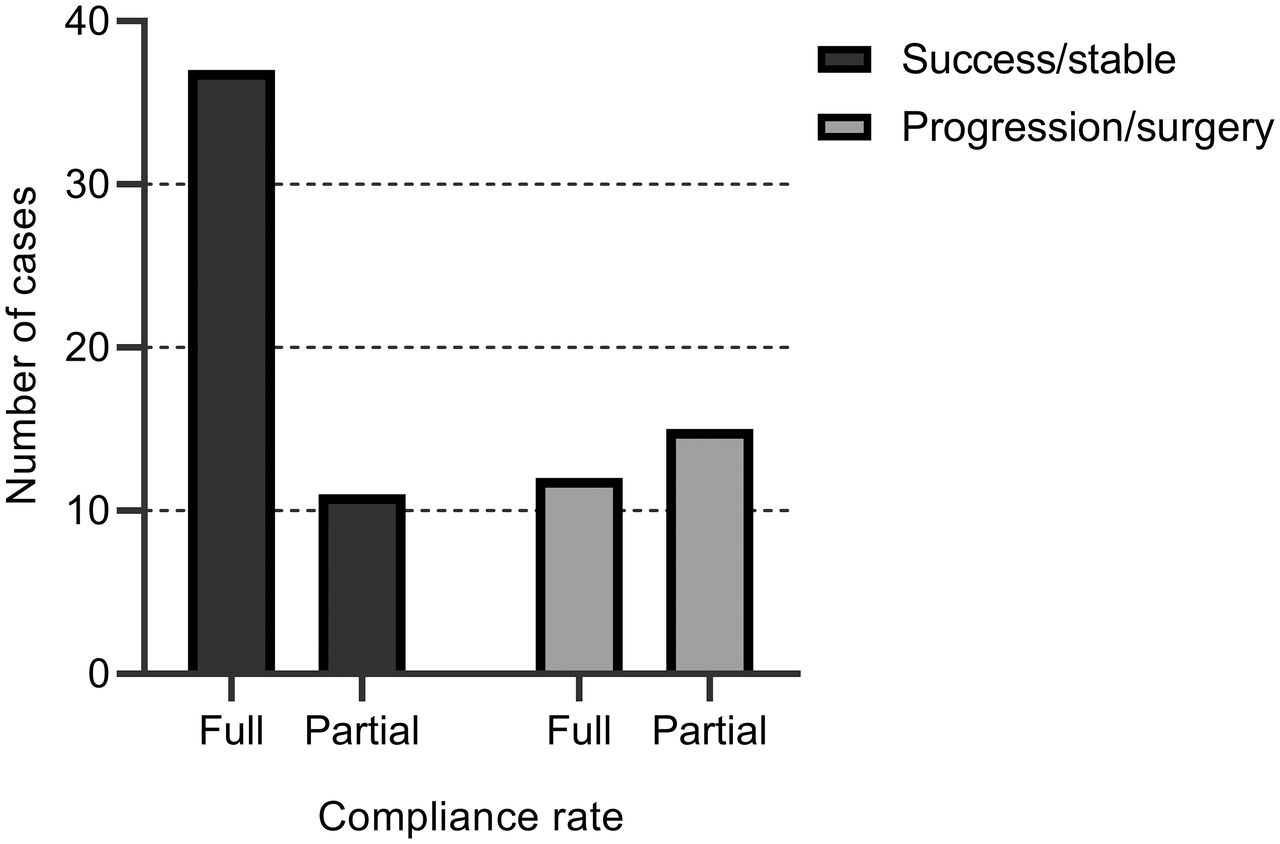
There was a significant difference in terms of adherence to the brace between the success/stable and progression/surgery groups (P = .008) (Figure 3). In the successfully treated group, 37 patients (77%) had full compliance and 11 had partial compliance (23%). On the other hand, in the progression/surgery group, 12 patients (44%) had full compliance and 15 had partial compliance (56%).
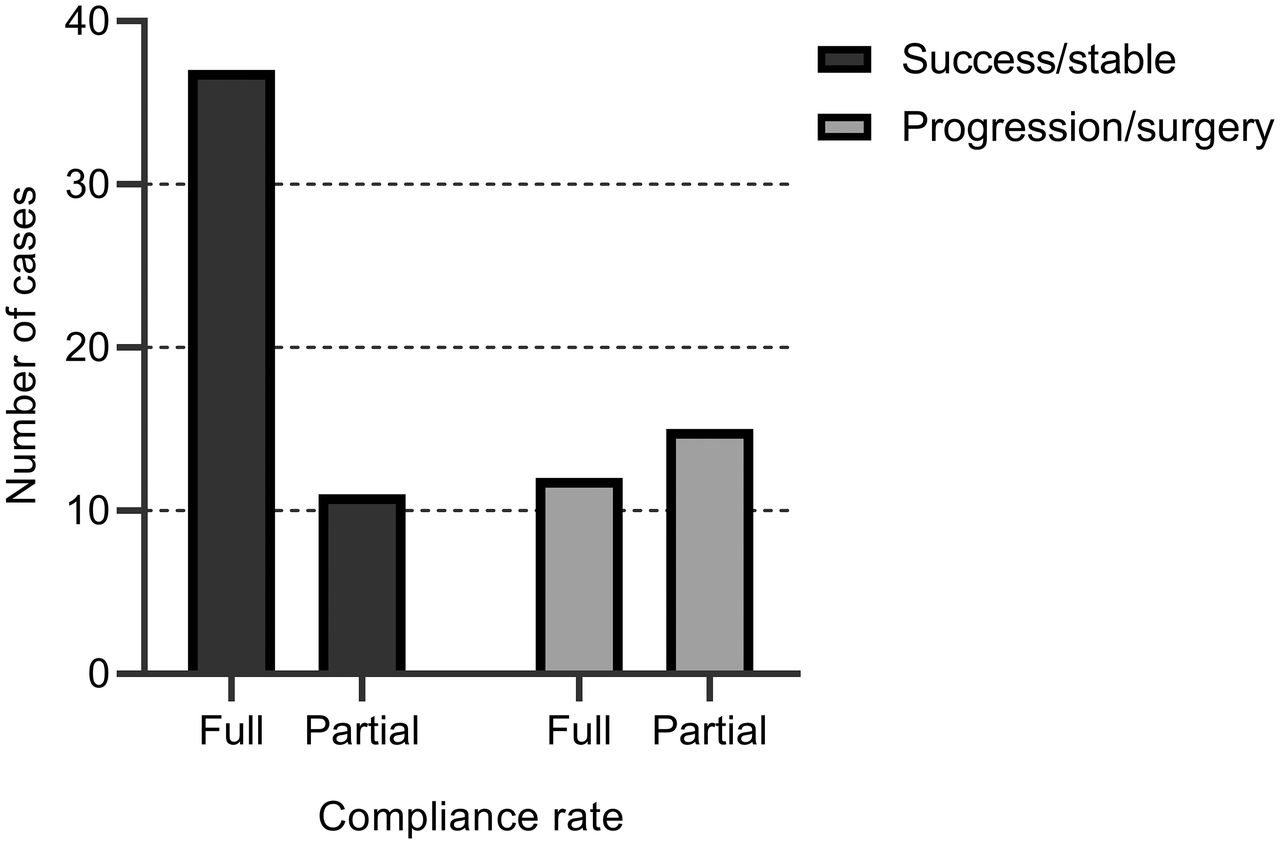
Brace compliance between the success/stable and progression/surgery groups.
Effect of Curve Type and Curve Magnitude
Impact of prebrace curve type and curve magnitude on the outcome of bracing is presented in Table 4. As expected, the progression rate was highest in patients with Lenke type III and lowest in Lenke type V. Before initiation of bracing, 28 patients had a Cobb angle of 29° or less (24.28° ± 2.60°), 31 patients had a Cobb angle of 30° to 45° (35.67° ± 5.00°), and the other 16 patients showed a large Cobb angle of >46° or more (54.62° ± 6.27°; P < .001). The progression rate was very high in patients with a curve magnitude of ≥46° (94%).
Impact of prebrace curve type and curve magnitude on effectiveness of bracing.
The average BIBC was 57% (6%–100%). However, patients with different curve type revealed a different BIBC. The average BIBC was 55% (6%–100%) for Lenke type I curves, 59% (26%–100%) for Lenke type II curves, 41% (14%–67%) for Lenke type III curves, and 62% (25%–100%) for Lenke type V curves. The results indicated that the Lenke type III curve is a prognostic factor for curve progression and spinal fusion.
Surgery
For a total of 27 patients (36%) the brace treatment failed. Of these, 21 patients (78%) underwent spinal fusion and the curves of 6 patients (22%) increased to ≥50°. Considering the clinical characteristics of JIS patients such as age, skeletal maturity, functional status, spinal height, and patients' and parents' preferences, the decision for surgical procedure may be difficult and complex. Nevertheless, the routine suggestion15 for spinal fusion in JIS patients is presence of a curve size >50°. At initiation of bracing, the average Cobb angle of the these patients was 46.90° ± 12.00° (25°–70°). Before surgery, the average age was 13.42 ± 1.39 years (10–15 years), with an average Cobb angle of 66.52° ± 13.57° (45°–95°). Finally, the rate of surgery was 48% (10 patients) in Lenke type III curves, 28.5% (6 patients) in Lenke type I curves, 14% (3 patients) in Lenke type V curves, and 9.5% (2 patients) in Lenke type II curves.
DISCUSSION
In JIS patients, the risk of curve progression is greater than in adolescent idiopathic scoliosis because the time span between initiation of deformity and skeletal maturity is very long. Therefore, for patients with progressive curves, consideration of brace management at manifestation of the deformity may significantly affect the final results. The present study was conducted with the aim of investigating the outcome of bracing in JIS patients and determining the influential factors on the success rate of brace treatment. The results showed that the success rate of bracing was 64%.
To the best of our knowledge, in the literature overall, 12 English language studies exist that have reported the results of brace treatment for JIS.1–3,9,11–15,20,22,23 Of these, only 5 studies had sample sizes of larger than 50 patients.2,11,12,15,24 The lowest success rate of bracing in JIS patients was reported in the Robinson and McMaster case series,2 where in spite of early diagnosis of deformity, brace treatment was initiated only for those with a curve magnitude higher than 30° (88 cases). In this study, the success rate was reported as 12.5% and the patients were followed up until skeletal maturity or spinal fusion. On the other hand, the highest success rate of bracing in JIS (94%) was reported by Aulisa et al,11 who conducted their study on 113 patients. In the study of Khoshbin et al,15 of the 88 cases with JIS, the overall success rate with bracing was 28%. Of the 125 patients in Harshavardhana and Lonstein's study,24 the reported success rate was 41%. Furthermore, in 5 studies, the follow-up duration was short, and not all patients were examined until skeletal maturity.3,9,13,14,22 In the study by Coillard et al,12 of 150 JIS patients undergoing the SpineCor brace treatment, only 67 patients were followed up until the end of skeletal maturity. Tolo et al3 conducted a study on 42 JIS patients, reporting the success rate of bracing as 81%. However, in this study, the follow-up duration was short, and only 4 patients were followed up until the end of skeletal maturity. The studies25 on patients with adolescent idiopathic scoliosis showed that after discontinuation of the brace treatment, nearly one third of the curves increased to higher than 5°. In the successfully treated patients of the present study, from initiation of weaning time to final follow-up, 63% of the curves had progressed to >5°.
In the present study we identified the prognostic factors in effectiveness of bracing such as BIBC, brace compliance, curve size, and curve type at initiation of bracing. The results indicated that the surgical rate in the patients with a prebrace Cobb angle <29° was very low (11%). However, for patients with a curve magnitude >46°, the rate of curve progression reached 94%. Therefore, bracing has a limited capacity to control the curve progression for JIS patients with Cobb angles >46°. The curve magnitude at initiation of bracing and surgical rate in patients who had braced during adolescents was significantly lower as compared with those who were braced during the juvenile period. These results are in line with the findings of Khoshbin et al15 and Harshavardhana and Lonstein.24
The mean BIBC in the present study was 57%; the maximum value was associated with patients with Lenke type V curve, and the minimum was associated with patients with Lenke type III curve. Thus, Lenke type III curve is a prognostic risk factor for progression of the curve and spinal fusion.15,26 In the present study, of 18 patients with Lenke type III curve, 10 patients had partial compliance and 8 had full compliance. However, there was no statistically significant difference in their compliance rate. Therefore, the lower success rate of bracing in patients with Lenke type III curve might be associated with the rigidity of the curve or the brace fitting. Previous studies have suggested that an increase in flexibility across the scoliosis curve and adjustment of the pressure pads of the brace at shorter intervals will decrease the risk of curve progression in patients with adolescent idiopathic scoliosis.27–29 Further research is required to evaluate these factors on JIS patients.
In the present study, brace compliance was assessed subjectively (reported by patients) and through appearance of the brace. The results showed that the compliance rate is associated with the outcome of brace treatment. In the success/stable group, compliance rate was significantly higher than in the progression/surgery group. These findings are consistent with the results of previous studies on JIS patients.15,18 Today, to measure the compliance objectively, reliable temperature or pressure data loggers are used, which offer researchers more accurate information on adherence of patients to the brace.30,31
There are no standardized criteria for evaluating the brace effectiveness on JIS. Recently, Harshavardhana and Lonstein24 published the results of their series on 125 juveniles with idiopathic scoliosis who were followed up until the end of skeletal maturity. In this study, the success rate of brace treatment according to inclusion criteria of the Scoliosis Research Society (SRS) Committee was reported as 41%. In the present study, the success of brace treatment based on the criteria of the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST) was 64%. However, if the success rate had been considered on the basis of SRS,32 it would have been 54%. The next step for SRS is establishing uniform criteria for subsequent studies on the effectiveness of bracing in JIS patients.
The present study had some limitations, however. First, because 54% of patients in our database were excluded from the study due to having been lost to final follow-up and discontinuation of bracing before skeletal maturity, the results may suffer lack of generalizability. Nevertheless, this exclusion of patients is expected in a retrospective study covering a 30-year period. Second, given the retrospective nature of the study, our data were limited to the information available in the clinical records of the patients. Nevertheless, assessment and recording of the data of all patients were performed by 1 surgeon and based on a constant method. Also, all of the required information was extracted from the clinical files of patients by 1 author. Third, most of the patients were treated by the Milwaukee brace. However, it was not possible to compare the results of treatment based on the type of brace. Fourth, this was a single-center case series performed in the senior author's spine clinic, which may reduce the generalizability of the findings. However, this center is one of the largest spine clinics in Iran, where scoliosis patients were referred to from all cities and provinces. Fifth, due to the retrospective nature of the present study, evaluating patient records from 1986 to 2013, measuring the brace wear compliance objectively was not feasible. Lavelle33 first introduced the use of a data logger to objectively measure brace compliance in 1996. However, at each follow-up during brace treatment, the treating physician recorded the average hours of brace wearing by evaluating the appearance of the brace and asking the patients and parents. Sixth, the Cobb angle measurements were performed based on applying the classical Cobb method on total-spine posteroanterior x-ray films. Reports showed that some fault may have occurred as a result of measurement error and insufficient clarity of radiographs.34 However, measurement error can be reduced when all Cobb angles are recorded by 1 observer and using 1 protractor.19 Finally, due to absence of any control group, it was not possible to compare the results of bracing with the natural history of JIS.
CONCLUSIONS
Brace treatment is an effective strategy for controlling the curve progression and avoiding spinal fusion in JIS if the curves are spotted early. The initial curve magnitude, type of the curve, and degrees of in-brace correction are prognostic risk factors for progression of the curve and spinal fusion in JIS.
Footnotes
Disclosures and COI: This research was supported by grant No. 32-33718 from the Rehabilitation Research Center of Iran University of Medical Sciences. The authors report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.