


ABSTRACT
Background: Atlantoaxial dislocation usually results in sudden death. The patient had never found any axial lesion before, and the atlantoaxial joint dislocation was caused by rotation of the neck due to discomfort of the neck. The patient was given surgical treatment after the rescue of respiratory and cardiac arrest during transportation, which was extremely rare and rarely reported.
Methods: A 62-year-old male patient presented with limited cervical mobility after a violent rotation of the neck due to neck discomfort. X-ray and computed tomography (CT) scan suggested atlantoaxial dislocation. Sudden respiratory and cardiac arrest during transportation was immediately followed by continuous cranial traction and successful occipital and neck fusion operation.
Results: After the successful rescue of endotracheal intubation, the patient was given continuous cranial traction. After the completion of CT scan, the patient was given occipital neck fusion, and 6 days after the surgery, the patient wore the skull-neck-thorax brace and walked freely.
Conclusion: Continuous cranial traction and posterior occipitocervical fusion are effective methods for treating axial pathological fracture with atlantoaxial dislocation.
Level of Evidence: 5.
INTRODUCTION
Rheumatic diseases, trauma, and tumor are the common causes of atlantoaxial dislocation.1 Occipitocervical fusion is generally applicable to upper cervical fracture and dislocation where atlantoaxial fusion is not possible.2 It is also one of the effective methods to correct upper cervical instability, and effective bone grafting is also a prerequisite for occipitocervical fusion.3
CASE REPORT
The patient was a 62-year-old male patient who felt neck discomfort 3 days before admission. After being violently attacked by others, he immediately felt neck pain and discomfort with limited movement. Cervical spine computed tomography (CT) scan was performed immediately in the local hospital, indicating that cervical 2 vertebral bone destruction was diagnosed as axial vertebra lesion in the local hospital, and the local hospital suggested to transfer the patient to the hospital for treatment. The family members led the patient to the outpatient clinic of our hospital from a distance of approximately 300 km. In the outpatient examination, the neck was askew to the front and bottom of the right, and the muscle strength of the limbs was normal. American Spinal Cord Injury Association was rated as grade E. X-ray (Figure 1) and CT (Figure 2) examinations of the cervical spine were performed immediately, suggesting pathological axial fracture with atlantoaxial dislocation. The patient was admitted to the Emergency Intensive Care Unit immediately. In the process of transfer, the patient suffered sudden breathing and cardiac arrest, and was immediately given endotracheal intubation and ventilator-assisted treatment. The patient regained spontaneous heart rate and respiration, and sustained cranial traction was given after the condition was stable. Cervical spine CT scan review (Figure 3) indicated good atlantoaxial joint reduction. After the completion of the examination, the patient was given occipitocervical fusion under general anesthesia. Axial vertebral body damage was found during the operation, and local biopsy was taken for examination. Postoperative disease examination suggested that there was a little degenerated bone tissue and necrotic components. Postoperative X-ray showed good internal fixation position (Figure 4).

Preoperative anteroposterior x-ray (left) and preoperative lateral x-ray (right). Overlap of the atlas posterior arch with the axial odontoid can be seen on lateral radiographs.
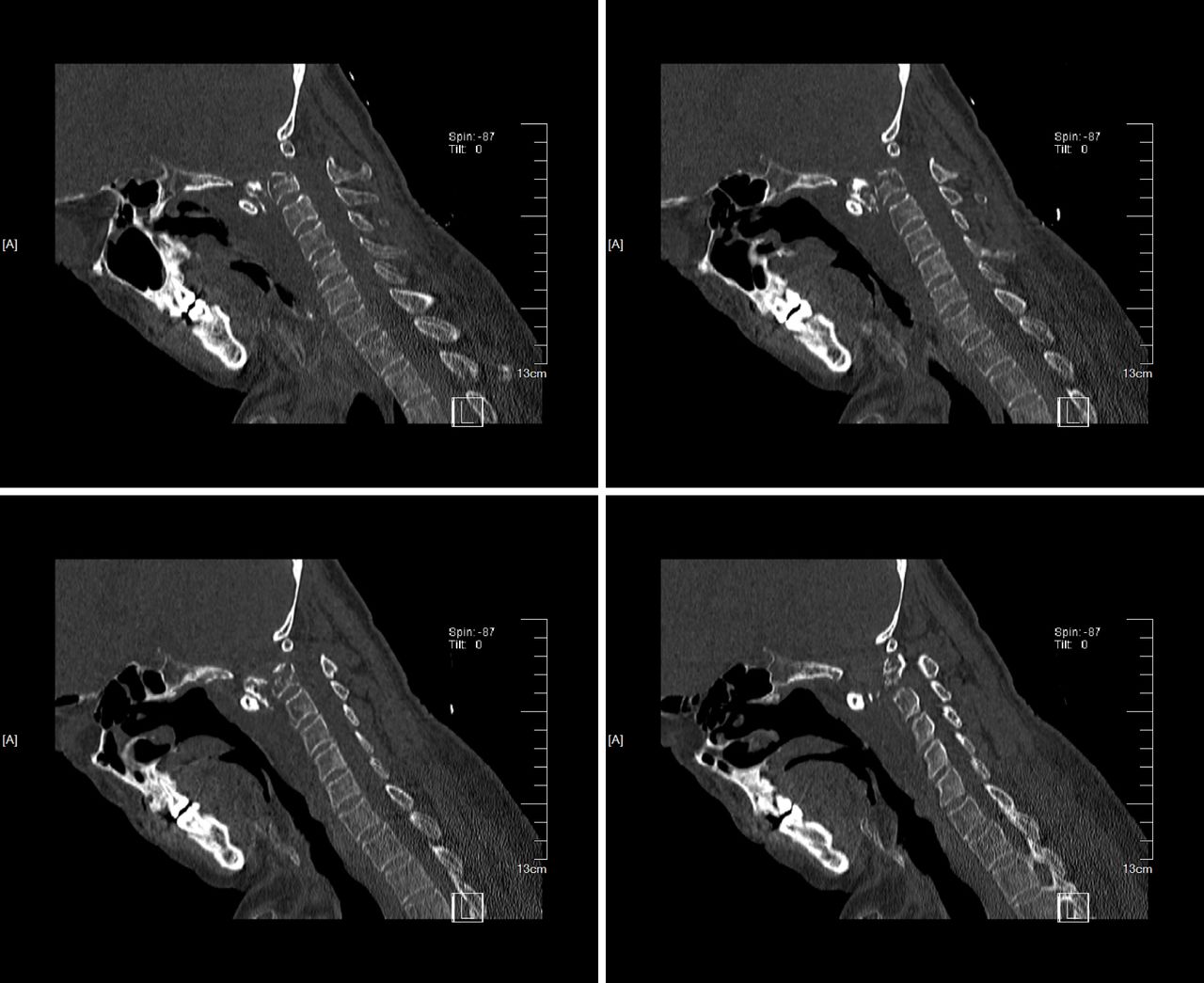
Preoperative computed tomography scan sagittal view showed axial odontoid fracture. The fracture end is located in front of the axial body.

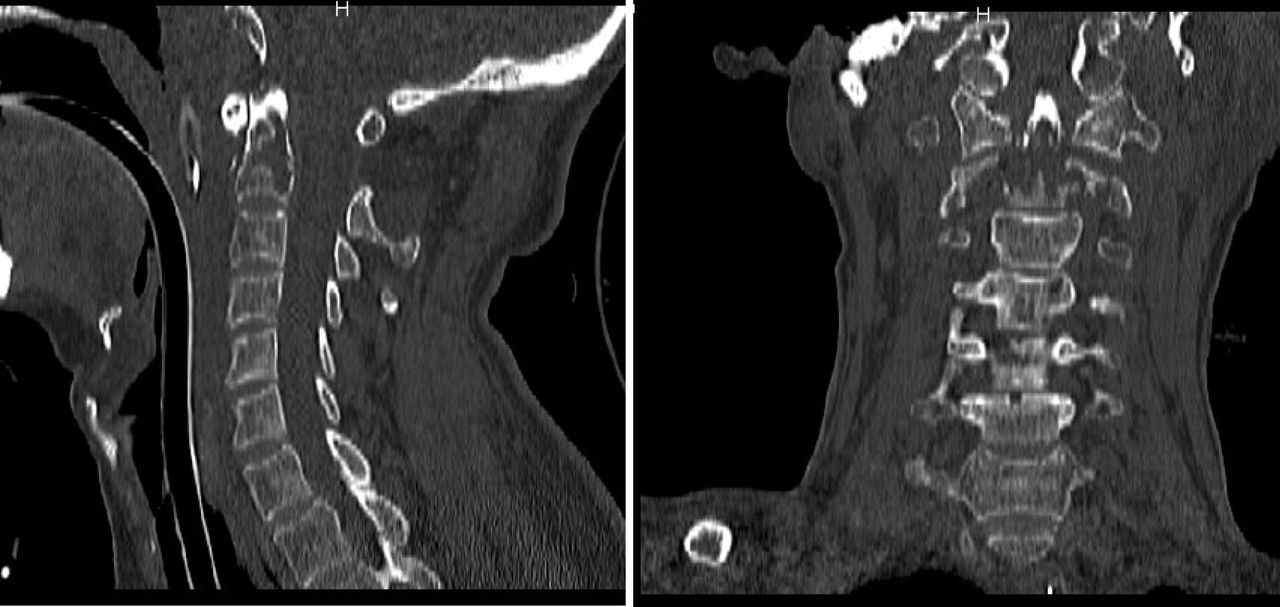
Complete reduction was seen in the sagittal and coronal positions after cranial traction.

Postoperation anteroposterior x-ray (left) and postoperation lateral x-ray (right).
DISCUSSION
Atlantoaxial dislocation can be divided into partial and complete dislocation. Most patients with complete dislocation die on the spot, although it is rare for the patient to travel to many places without death. The reason may be that dislocation accompanied by local bone destruction leads to slight expansion of spinal canal volume, and no respiratory or cardiac arrest occurs in the mobile position. Tuberculosis of the cervical spine is more rarely reported, accounting for 0.3%–1% of systemic tuberculosis.4,5 Cervical tuberculosis may not be detected at the early stage. Because the patient has no clinical symptoms, the present onset is neck discomfort and posttraumatic atlantoaxial dislocation. Moreover, the role of polymerase chain reaction in the diagnosis of bone tuberculosis is not clear6,7 because it can be rapidly excluded but cannot be diagnosed,8 as shown in this case.
Atlantoaxial tuberculosis often leads to bone destruction of atlantooccipital joint, and local ligament relaxation leads to atlanto-occipital joint instability, so it is particularly important to clear the lesion and reconstruct the stability of upper cervical vertebra.9 Although anterior surgery can achieve the purpose of clearing lesions and decompression of spinal canal, anterior surgery is difficult to reconstruct the stability of atlas and occipital region, and posterior surgery can achieve the purpose of bone grafting and fusion internal fixation,10 but posterior surgery alone is difficult to completely remove lesions, so the selection of surgical methods is particularly important.11 In this case, no local pharyngeal wall abscess was found to form before surgery, so posterior surgery was performed directly after skull traction. However, for other patients with tuberculosis with abscess formation, anterior decompression and posterior fixation and fusion surgery were required, so as to better restore the stability of upper cervical vertebra.
The choice of autologous bone graft or allograft fusion in occipitocervical fusion has always been controversial. Godzik et al12 believed that the success rate of allograft fusion was relatively high, and the occurrence of complications related to body bone was avoided. The thickest part of the occipital region is mostly located in the external carinal process.13 It is still controversial to fix the occipitocervical fusion vertebra to C2 or C3. Pan et al14 found no statistical difference in the rate of fixed C2 or C3 fusion, but there were more complications in the treatment group than in C2. In this case, due to the obvious axial vertebra destruction, we adopted cervical 3 in the operation, and the postoperative effect was good.
CONCLUSIONS
Continuous cranial traction and posterior occipitocervical fusion are effective methods for treating axial pathological fracture with atlantoaxial dislocation.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.