


ABSTRACT
Purpose: The objective of this study was to compare clinical and radiologic parameters between minimally invasive surgery–transforaminal lumbar interbody fusion (MIS-TLIF) and open TLIF.
Methods: Data of 145 patients who underwent single- or double-level TLIF procedures with an open (n = 76) or a MIS (n = 69) technique were analyzed. Average operation time, estimated blood loss, and hospital stay were compared between open TLIF and MIS-TLIF. Improvement in clinical scores was analyzed using visual analog scale (VAS) and Oswestry Disability Index (ODI) scores in both groups and statistically compared using t tests. Radiologic parameters, such as lumbar lordosis, focal lordosis at the index level, and pelvic incidence (PI), were calculated at preoperative, postoperative, and final follow-up for comparison. The differences in improvement between open and MIS groups were analyzed using unpaired t tests.
Results: Average follow-up was 35.8 ± 15.4 months in open TLIF and 37.9 ± 14.4 months in MIS-TLIF. The average blood loss and operation times were higher and hospital stay was less in MIS-TLIF compared to open TLIF. VAS scores were improved from preoperative (8.5 ± 0.6) to postoperative (2.1 ± 0.8) and preoperative (8.4 ± 0.8) to postoperative (2.0 ± 0.7) in open TLIF and MIS-TLIF, respectively (P < .0001), and ODI scores were improved from preoperative (55.2 ± 5.2) to postoperative (22.5 ± 4.3) and preoperative (56.7 ± 4.9) to postoperative (22.0 ± 5.0) in open TLIF and MIS-TLIF, respectively (P < .0001). Similarly, there were significant improvements in lumbar lordosis and focal lordosis at the index level with a difference of 3.9° and 2.5°, respectively, in open TLIF and 4.0° and 2.9°, respectively, in MIS-TLIF. However, there were no differences in PI in both groups. There were 9 (11.8%) and 9 (13%) complications encountered in open TLIF and MIS-TLIF, respectively. Two patients from open TLIF and 5 from MIS-TLIF had to undergo revision surgeries without any statistical difference.
Conclusions: Open TLIF and MIS-TLIF are equally efficient surgical techniques with similar clinical and radiologic outcomes. MIS-TLIF is associated with less intraoperative blood loss and hospital stay; however, it increases operation time significantly.
INTRODUCTION
Lumbar interbody fusion with instrumentation is an effective surgical option to stabilize the painful motion segment and provides an indirect decompression of the neural elements, correcting lordosis and deformity.1 Five different types of lumbar interbody fusion procedures are performed by spine surgeons: posterior lumbar interbody fusion, transforaminal lumbar interbody fusion (TLIF or minimally invasive TLIF [MIS-TLIF]), oblique lumbar interbody fusion (OLIF), anterior lumbar interbody fusion, and lateral lumbar interbody fusion (LLIF/XLIF).2 However, there is no clear-cut definitive evidence for 1 approach being superior to another in terms of fusion or clinical outcomes. However, there are certainly some advantages for using 1 technique over another, and therefore specific indications for each technique have been described in the literature.2
Among them, the TLIF technique was first reported by Harms and Rolinger3 in 1982. Thereafter, TLIF has been increasingly used in a variety of lumbar diseases, including degenerative lumbar disc diseases, spondylolisthesis, degenerative scoliosis, and spinal instability.4,5 Although TLIF is an effective procedure, extensive stripping of the paravertebral muscles and prolonged retraction are required for adequate exposure of the surgical field.6,7 Iatrogenic muscle damage can lead to atrophy of the paraspinal muscles and chronic postoperative low back pain.8,9 Additionally, TLIF may not be as effective as OLIF or XLIF to correct coronal imbalance and restore lordosis.
The MIS-TLIF procedure was first described by Foley et al10 in 2003. Its popularity has been increasing since then. Favorable outcomes of MIS-TLIF have been reported for various surgical indications.11–13 The disadvantage includes exposure to ionizing radiation.14 Moreover, longer surgical time has also been reported for MIS-TLIF, at least in a few cases, and can be attributed to a narrow working channel, which could be a reflection of technical differences compared to open TLIF; however, some authors associate this with a significant learning curve.15–18 The maintenance of sagittal balance while performing the TLIF procedure has been emphasized in the literature as related to both clinical outcome and adjacent segment degeneration.19 Although several studies have compared the functional outcome between open TLIF and MIS-TLIF, only a few have compared the correction of radiologic parameters.20–23
The purpose of this study was to compare the clinical, perioperative, and radiologic outcomes between MIS-TLIF and conventional open TLIF procedures during single- or double-level (short-segment) lumbar fusion. This study also focuses on spine sagittal alignment parameters after the fusion.
MATERIALS AND METHODS
A retrospective analysis of total 145 patients who underwent single- or double-level TLIF procedures between January 2016 and December 2018 was carried out. All subjects were operated for either open TLIF (n = 76) or MIS-TLIF (n = 69) procedures with the following inclusion criteria: (1) mechanical low back pain and radicular leg symptoms, (2) lack of response to conservative therapy for at least 6 weeks, (3) age between 18 and 80 years, (4) single- or double-level (short-segment) involvement, and (5) magnetic resonance imaging (MRI) showing 1- or 2-level lumbar stenosis with facetal hypertrophy or grade 1 to 2 spondylolisthesis. Exclusion criteria included 3-level or higher surgeries, history of previous spine surgeries, revision surgeries, cauda equina syndrome, spine infection or pathology, significant lumbar deformity requiring correction, and lack of lateral lumbosacral X-ray on 3 different occasions or poor-quality X-rays. All the open TLIF and MIS-TLIF procedures were performed by a single spine surgeon in a single center. Selection of open TLIF or MIS-TLIF was decided by patients after explaining the procedures and discussing the patients' financial constraints.
Operation time in minutes, estimated blood loss (EBL), length of stay, perioperative morbidity, and complications were collected prospectively in all surgeries. All patients were followed up at 1, 3, 6, and 12 months and yearly thereafter. Clinical improvement was analyzed using visual analog scale (VAS) and Oswestry Disability Index (ODI) scores at preoperative, at 1-month postoperative, and at the final follow-up.
SURGICAL METHOD
Techniques for MIS-TLIF
In MIS-TLIF, decompression was considered on the more symptomatic side at the affected level. The level of operation was confirmed under anteroposterior and lateral views of the C-arm. A horizontal line was also drawn joining the midpoint of the right and left pedicle on each vertebra. Right and left vertical lines were drawn at the lateral part of the pedicles. These lines were used to take an entry into the pedicles with Jamshidi needles for screw insertion. An approximate 25-mm vertical incision was kept just 10 mm lateral to the vertical pedicle line at the appropriate level. Serial tubular dilators and a retractor tube were inserted to reach to the facet joint, which was fixed with a table rod-clamp. A monopolar cautery and disc forceps was used to expose the facet joint. Facetectomy was done using a high-speed burr and osteotome under a microscope. The ligamentum flavum was removed with Kerrison rongeurs to assess the dura and nerve root. Contralateral decompression was also carried out by an over-the-top technique if required. The traversing nerve and dura were retracted medially to expose the target disc, and a thorough discectomy was performed. Endplate preparation was done, and an appropriately size TLIF cage was inserted along with local bone grafts. Percutaneous pedicle screw fixation was performed under the C-arm guidance.
Techniques for Open TLIF
The level to be operated on was confirmed under anteroposterior and lateral views of the C-arm. After midline posterior incision, subperiosteal dissection was carried out to the tips of the spinous processes to expose the entry points for the pedicle screws. Insertion of pedicle screws and the rod-screw construct was performed, followed by laminectomy and facetectomy on the symptomatic side to achieve decompression at the affected level. Discectomy was done by retracting the traversing nerve root and dura medially, and the TLIF cage was inserted with local bone grafts.
Radiologic Measurements
Pelvic incidence (PI) angle was measured between 2 lines: 1 from the midpoint of the upper sacral endplate to the hip axis and 1 perpendicular to the upper sacral endplate. Focal lordosis is the angle between upper and lower endplates, composed of the disc space. Focal lordosis of the disc space was measured where the TLIF cage was inserted. Similarly, the lumbar lordosis angle is defined as the angle between the upper endplate of the L1 vertebra and upper endplate of the sacrum. In our study, perpendicular lines were drawn from these lines in Microsoft PowerPoint, and the angle was measured manually between 2 perpendicular lines. The measurement of parameters of sagittal balance was done by a single observer from the lumbosacral radiographs of 3 different occasions: preoperative, immediately postoperative, and final follow-up. Measurement of angles was recorded 3 times at an interval of at least 1 week between 2 measurements, and average values were calculated.
Statistical Analysis
Statistical analysis for clinical and radiologic parameters was performed using SPSS software (version 17, SPSS, Chicago, Illinois) with t tests and χ2 tests.
RESULTS
Of 145 patients, 76 and 69 were in the open TLIF group and MIS-TLIF group, respectively. The average age of patients in the open TLIF and MIS-TLIF groups was 51.5 ± 14.0 years and 51.2 ± 12.2 years, respectively. The average follow-up was 35.8 ± 15.4 months in the open TLIF group and 37.9 ± 14.4 months in the MIS-TLIF group. There were 35 males and 41 females in the open TLIF group and 31 males and 38 females in the MIS-TLIF group, suggesting no difference in both groups (P = .891, χ2 test) regarding sex distribution. There were 34 single-level and 42 double-level surgeries in the open TLIF group and 45 single-level and 24 double-level surgeries in the MIS-TLIF group, suggesting that the open TLIF group had significantly higher double-level surgeries (P = .013, χ2 test). Involvement of levels and demographics are shown in Table 1.
Number of patients in each group with single- or double-level disc herniation.
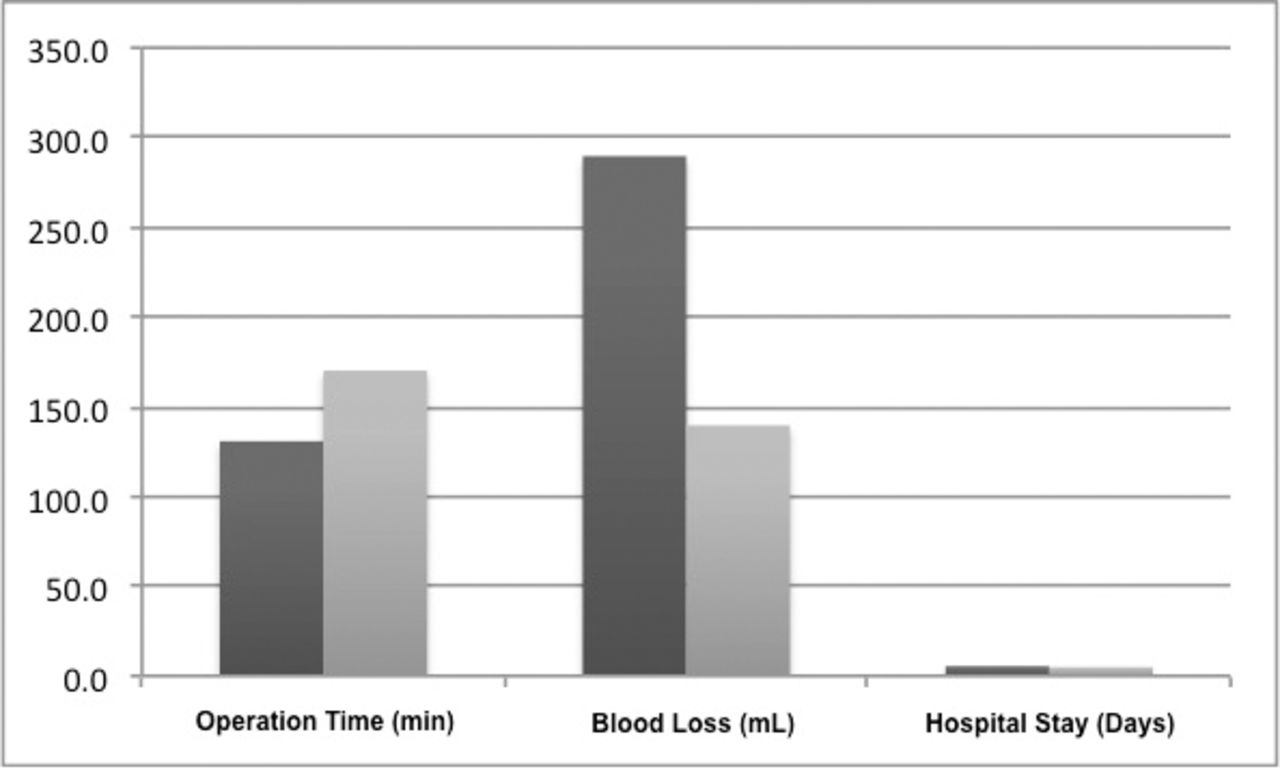
Average operation time, EBL, and hospital stay were 130.8 ± 15.2 minutes, 289.7 ± 58.5 mL, and 5.5 ± 1.3 days, respectively, in the open TLIF group and 170.1 ± 18.8 minutes, 139.6 ± 42.2 mL, and 4.9 ± 0.8 days, respectively, in the MIS-TLIF group (Figure 1). There was significantly longer operation time (P < .0001, unpaired t test) and significantly less EBL (P < .0001, unpaired t test) in the MIS-TLIF group compared to the open-TLIF group. Average hospital stay was also longer in the open-TLIF group than the MIS-TLIF group (P = .002, unpaired t test) (Table 2).

Bar diagram of average operation time (minutes), intraoperative blood loss (mL) and hospital stay (days) for open TLIF and MIS-TLIF group (dark area is for open TLIF, and lighter area is for MIS-TLIF). TLIF indicates transforaminal lumbar interbody fusion; MIS-TLIF, minimally invasive surgery–transforaminal lumbar interbody fusion.
Average operation time, blood loss, and hospital stay in both groups and according to single- or double-level involvement.
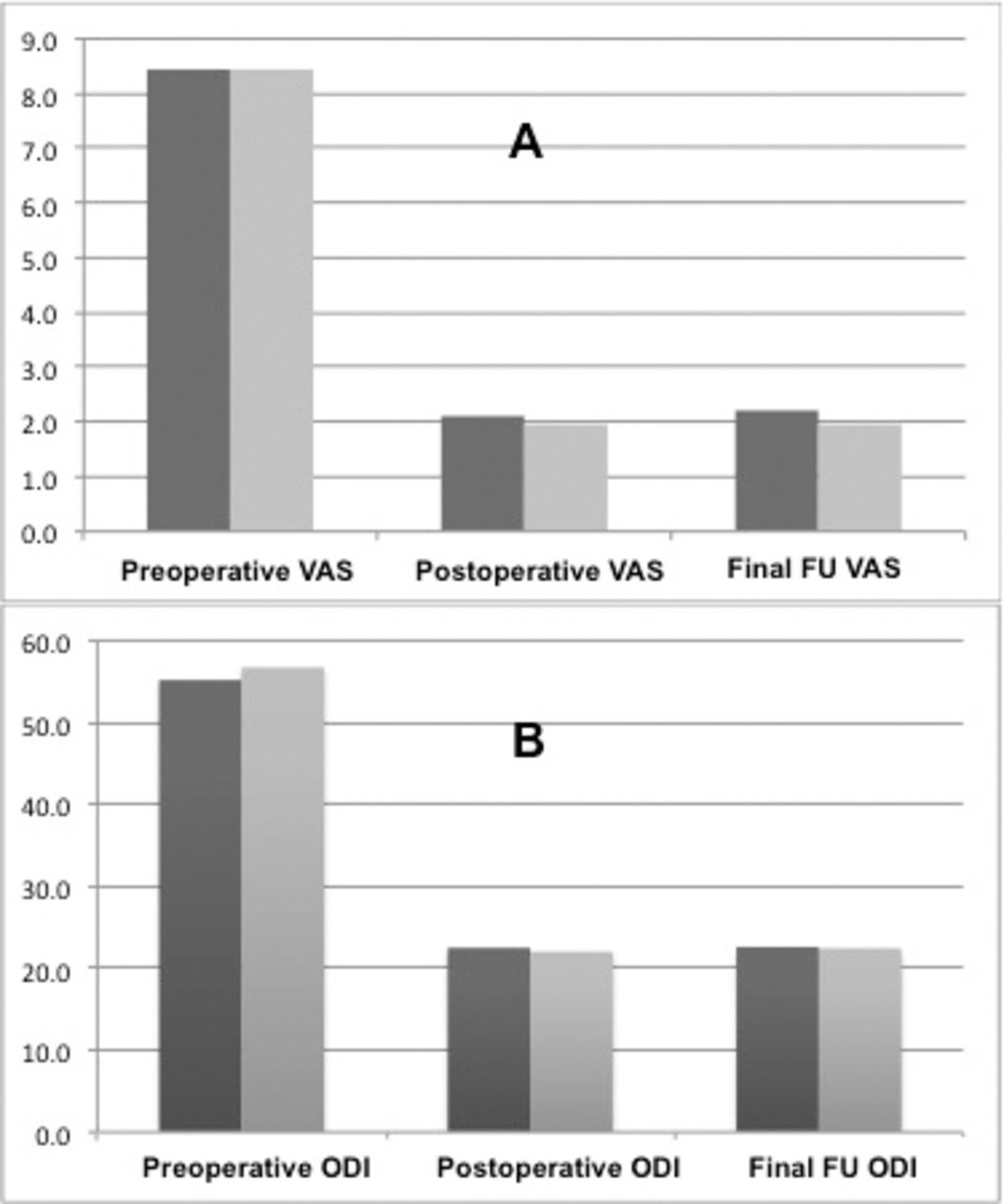
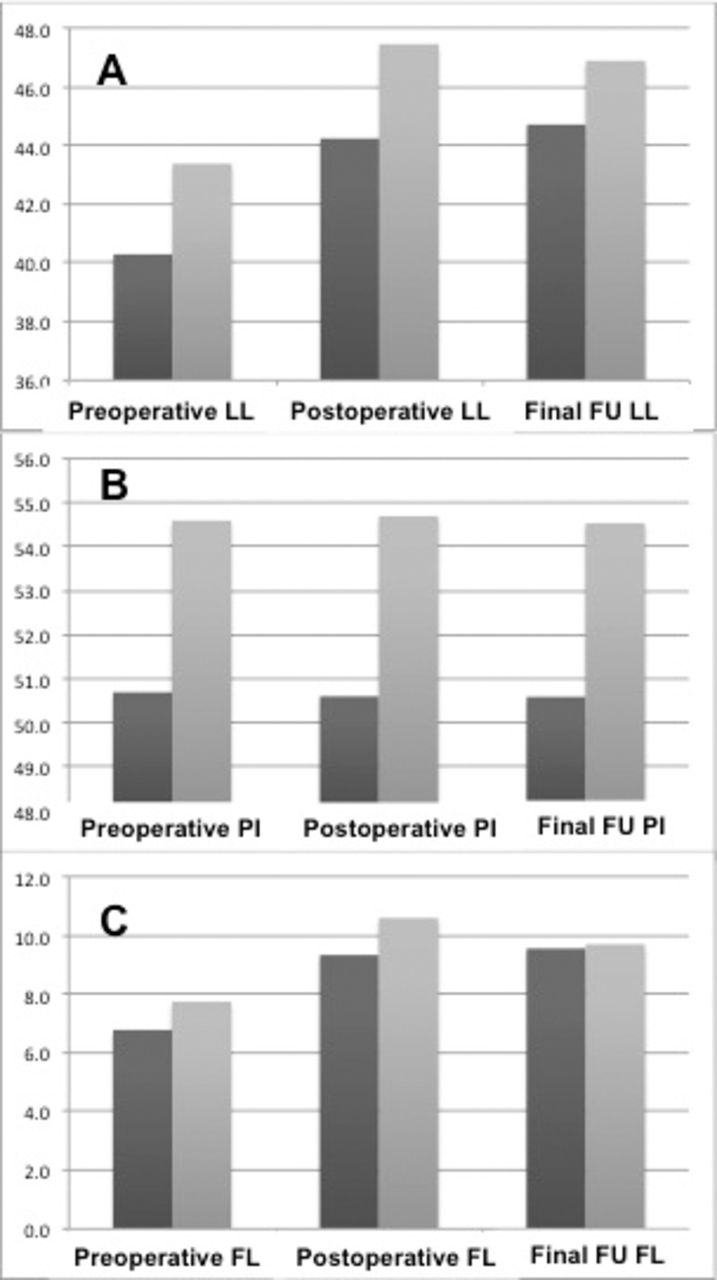
Clinically average preoperative, postoperative, and final follow-up VAS scores were 8.5 ± 0.6, 2.1 ± 0.8, and 2.2 ± 0.7, respectively, in the open TLIF group and 8.4 ± 0.8, 2.0 ± 0.7, and 2.0 ± 0.8, respectively, in the MIS-TLIF group. Similarly, average preoperative, postoperative, and final follow-up ODI scores were 55.2 ± 5.2, 22.5 ± 4.3, and 22.6 ± 4.4, respectively, in the open TLIF group and 56.7 ± 4.9, 22.0 ± 5.0, and 22.4 ± 4.7, respectively, in the MIS-TLIF group (Table 3). There was significant clinical improvement in VAS and ODI scores postoperatively in both groups (P < .0001, paired t test), and all changes were maintained at the final follow-up (Figure 2). However, there was statistically no difference in improvement in both groups (P = .0612 for VAS and P = .820 for ODI). In the open TLIF group, average preoperative, postoperative, and final lumbar lordosis were 40.3° ± 10.9°, 44.2° ± 11.1°, and 44.7° ± 11.2°, respectively; PI was 50.7° ± 10.8°, 50.6° ± 10.8°, and 50.6° ± 10.8°, respectively; and, similarly, focal lordosis at the index level was 6.8° ± 5.8°, 9.3° ± 5.9°, and 9.6° ± 5.7°, respectively (Figure 3). There was significant improvement in lumbar lordosis (P < .0001, paired t test) and focal lordosis at the index level (P < .0001, paired t test) postoperatively; however, there was no significant difference in PI (P = 0.584, paired t test). In the MIS-TLIF group, average preoperative, postoperative, and final lumbar lordosis were 43.4° ± 11.5°, 47.4° ± 12.1°, and 46.9° ± 12.1°, respectively; PI was 54.6° ± 10.4°, 54.7° ± 10.0°, and 54.5° ± 10.1°, respectively; and, similarly, focal lordosis at the index level was 7.7° ± 5.1°, 10.6° ± 5.1°, and 9.7° ± 4.8°, respectively. There was significant improvement in lumbar lordosis (P < .0001, paired t test) and focal lordosis at the index level (P < .0001, paired t test) postoperatively; however, there was statistically no difference in PI (P = 0.472, paired t test) (Table 3).
Preoperative, postoperative, and final follow-up clinical visual analog scale (VAS) and Oswestry Disability Index (ODI) scores and radiologic parameters using lumbar lordosis (LL), pelvic incidence (PI), and focal lordosis at the index level (FL) in both groups.
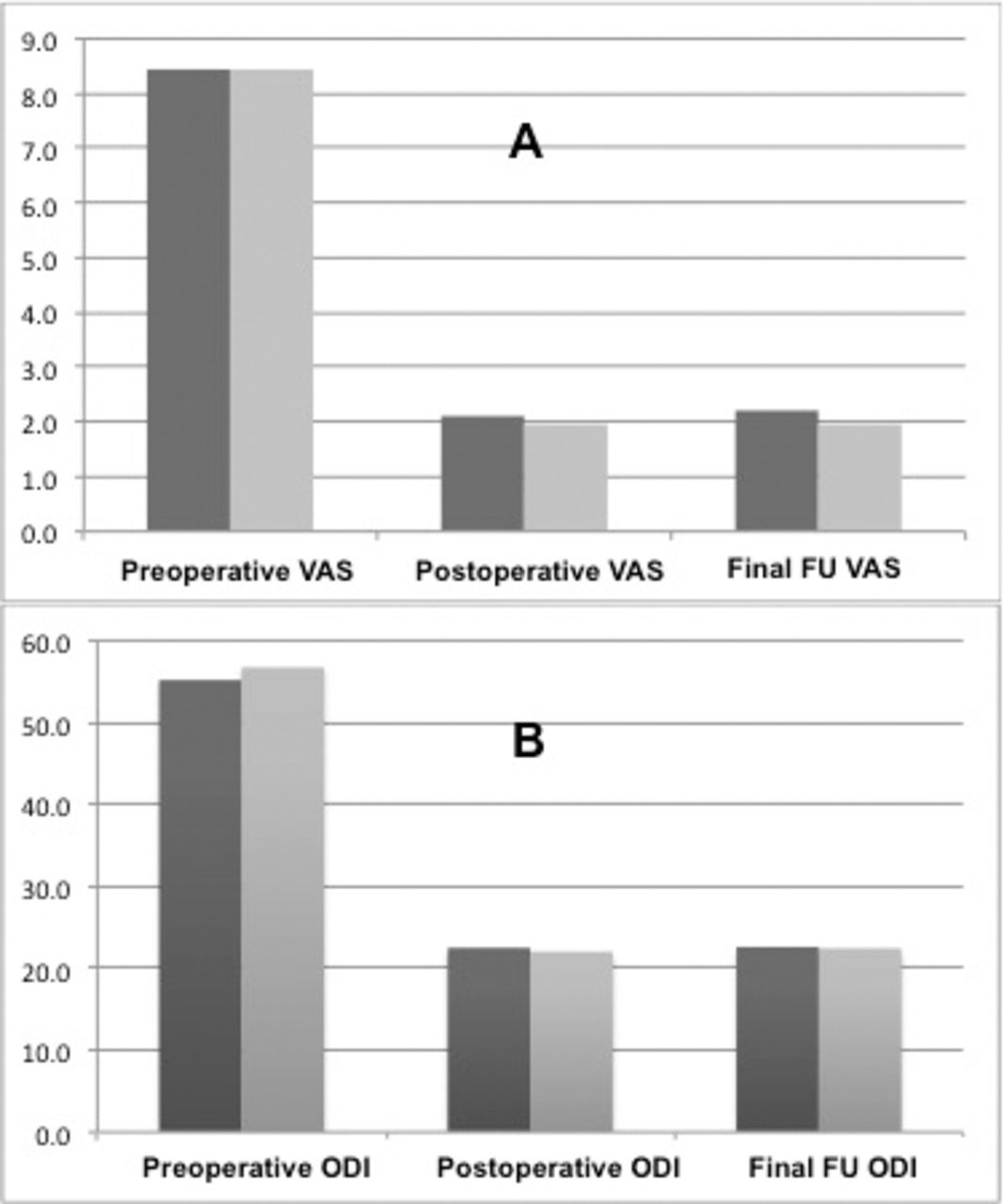
Bar diagram of average preoperative, postoperative, and final follow-up for (A) visual analog scale (VAS) and (B) Oswestry Disability Index (ODI) in open TLIF and MIS-TLIF (dark area is for open TLIF, and lighter area is for MIS-TLIF). TLIF indicates transforaminal lumbar interbody fusion; MIS-TLIF, minimally invasive surgery–transforaminal lumbar interbody fusion.

Bar diagram of average preoperative, postoperative, and final follow-up for (A) lumbar lordosis (LL), (B) pelvic incidence (PI), and (C) focal lordosis at the index level (FL) in open TLIF and MIS-TLIF (dark area is for open TLIF, and lighter area is for MIS-TLIF). TLIF indicates transforaminal lumbar interbody fusion; MIS-TLIF, minimally invasive surgery–transforaminal lumbar interbody fusion.
There were total 9 complications each in the open TLIF (11.8%) and MIS-TLIF (13%) groups (Table 4). In the open TLIF group, there were 4, 2, 1, 1, and 1 patients with persistent numbness, postoperative radicular symptoms, wound infection, mild back-out of cage, and foot drop postoperatively. Two patients who had postoperative wound infection and foot drop due to a malpositioned pedicle screw at L3 required revision surgery. Other patients were treated conservatively, as there was no obvious cause found on repeat imaging. A patient with mild back-out of cage was asymptomatic and therefore was treated conservatively. In the MIS-TLIF group, 3 patients had back-out of cage, of which 2 had revision surgery in the form of the removal of the cage, while 1 was treated conservatively, as there was no symptoms. In the MIS-TLIF group, 1 patient each had symptoms of postoperative numbness, postoperative radicular pain, wound infection, dural tear, hematoma, and screw breakage. The patients who had screw breakage, hematoma, and infection were reoperated, while others were treated conservatively. There was no difference found in terms of complications and revisions in both groups (P = .826 for complications and P = .146 for revisions, χ2test).
Complications in both groups.
DISCUSSION
TLIF is an established technique for the treatment of various lumbar disc degenerative diseases, instability (spondylolisthesis), severe lumbar stenosis, and lumbar disc herniation for which conservative treatment is ineffective. Since there is less violation of bony structure and spinal musculature, the MIS-TLIF technique is currently as widely accepted as the open TLIF technique.24,25 Moreover, less intraoperative blood loss and less tissue trauma during MIS-TLIF speeds up postoperative recovery of the patient, leading to earlier discharge from the hospital. Our study has shown that patients in the MIS-TLIF group had significantly shorter length of hospital stay than those in the open TLIF group (although the difference is minimal). Thus, MIS-TLIF can help reduce the total expenditure for surgery due to the shorter length of the stay in the hospital.26 In most meta-analyses, the length of the patient's hospital stay with the MIS-TLIF technique was found to be significantly shorter. Tian et al27 reported a difference of 2.7 days, while Hu et al28 in their meta-analysis observed a range of between 1.3 and 10.6 days. Lin et al29 analyzed 18 studies reporting a significant difference of 1.3 days less for MIS-TLIF.
In our study, EBL was 289.7 ± 58.5 mL and 139.6 ± 42.2 mL in the open TLIF and MIS-TLIF groups, respectively, suggesting significantly less blood loss in the MIS-TLIF group (P < .0001, unpaired t test). Ahmed et al30 found that EBL was 568.18 mL in the open TLIF group and 247.82 mL in the MIS-TLIF group. The difference was significant (P < .00001, unpaired t test). The mean length of stay was 5.05 days in the MIS-TLIF group versus 6.92 days in the open TLIF group. The difference was significant. Mean operative time was 130.8 ± 15.2 minutes and 170.1 ± 18.8 minutes in the open TLIF and the MIS-TLIF group, respectively, in our study. Mean operative time in the MIS-TLIF and open TLIF groups was mentioned as 375 minutes and 161 minutes, respectively, by Sulaiman et al31 and as 368.3 minutes and 252.5 minutes, respectively, by Hey and Hee.32 Operative time is certainly longer in the MIS-TLIF group, as the working channel is narrow and the surgeon has to develop depth sensation to work through the tube, making the learning curve long.33 Although the operative time is higher in the MIS-TLIF group of patients, less tissue trauma, preservation of the midline structure, and lesser osteotomy make the surgery superior with less blood loss, an earlier return to home, and less back and leg pain. Moreover, as the surgery is done under IITV guidance, the time required for taking IITV images has a significant contribution to total operative time. Our study also proved that although operation time is longer in the MIS-TLIF group than in the open TLIF group, it results in less EBL and less tissue trauma, favoring its acceptability. It also naturally understood that double-level surgery in open TLIF or MIS-TLIF would require a longer operation time, more EBL, and a longer hospital stay, as shown in Table 2; however, it did not make a significant difference with regard to the purpose of this study. Therefore, in terms of short-segment (up to two levels) surgery, further detailed analysis regarding single- or double-level surgery outcome would be of little significance and so was not included in the study.
Better VAS and ODI outcomes result from shorter durations of intramuscular pressure and less tissue injury caused by a more experienced surgeon, but long operation time is associated with poor VAS and ODI scores when surgery is performed by surgeons in the early stage of the learning curve.34–38 A multicenter randomized study conducted by Alamin et al39 to evaluate the effect of MIS-TLIF versus open TLIF on paraspinal musculature using MRI showed that both quantitative and qualitative measures of edema in the multifidus were significantly less in the MIS-TLIF group, which is consistent with less muscle injury. In our study, we found significant improvement in both VAS and ODI scores postoperatively in both groups, which were maintained at the final follow-up. Hammad et al30 found that the complication rate was lower with MIS-TLIF (11.3%) versus open TLIF (14.2%) but not statistically significantly different (P > .05). No significant differences were found in VAS (back and leg) and ODI scores between techniques at the final follow-up. In our study, we found similar complications in both groups (11.8% in open TLIF and 13% in MIS-TLIF), similar to published reports. Additionally, there was no significant difference found between reoperation rates in both groups. On the other hand, Villavicencio et al25 reported complication rates of 31.6% in MIS-TLIF and 31.7% in open TLIF. Their reported complications included infection, malpositioned pedicle screws, neurologic deficit (foot drop), hematoma, conversion of percutaneous to open technique, and leaks of cerebrospinal fluid. We also found similar types of complications in our series; however, none of the patients had to convert from a percutaneous technique to an open technique. However, 2.7% of patients from open TLIF and 7.2% of patients from MIS-TLIF had to undergo revision surgeries in our series. The difference was not statistically significant.
Regarding sagittal parameters, we compared 3 parameters—lumbar lordosis, PI, and focal lordosis—at the index level in both groups. In our study, the values of preoperative, postoperative, and final PI angle were approximately same (P = .584 for open TLIF and P = .472 for MIS-TLIF), which supports the statement that the PI is a fixed angle for the same person.40,41 The effect on PI has been investigated in our series with TLIF procedures. Similar preoperative, postoperative, and final PI values further emphasize the fact that PI acquired during individual development is definitively stabilized in adults.42 Carlson et al43 found average preoperative lumbar lordosis to be 39.6°, which improved to 45.0° postoperatively with a difference of 5.2°, and, similarly, average preoperative segmental lordosis was 12.7°, which improved to 15.0° postoperatively with a difference of 2.1°. In our series, we also demonstrated that lumbar lordosis and segmental (focal) lordosis at the index level improved postoperatively with a difference of 3.9° and 2.5°, respectively, in open TLIF and 4.0° and 2.9°, respectively, in MIS-TLIF (Table 3). This also proves that the majority of the lordosis gets corrected at the index level with the TLIF procedure. We agree that we have excluded those patients who had significant coronal or sagittal deformities preoperatively, and therefore we recommend further studies, especially in patients with significant coronal or sagittal deformities, to compare the difference in these parameters postoperatively.
CONCLUSIONS
At present, both MIS-TLIF and open TLIF are widely used surgeries that address degenerative, traumatic, neoplastic, and developmental disorders in the spine. Therefore, comparative study of MIS-TLIF with open TLIF has been necessary and done in different parts of the world.21,44,45 Several meta-analyses have been done on this subject46,47; however, such studies in the Indian context are limited.48,49 Our study has provided a comprehensive comparative study with a good number of patients and includes a comparative analysis of MIS-TLIF and open TLIF in terms of parameters of sagittal balance. We believe that a large patient population and follow-up of more than 2 years would make it more acceptable. Our study found MIS-TLIF and open TLIF equally effective in correcting lumbar lordosis and focal lordosis. Some studies revealed success in improving segmental lordosis and pelvic tilt; simultaneously, the minimally invasive nature of the approach has raised controversy regarding its capacity to do so.50–52 Few studies have proved the superiority of anterior and lateral approaches over TLIF regarding the correction of segmental lordosis and disc height.22,53 As this study compared different aspects of MIS-TLIF and open TLIF surgery, the study of other approaches is beyond the scope of this study. Being a comparative study, our study found MIS-TLIF and open TLIF to be equally effective in correcting lumbar lordosis and focal lordosis.
Footnotes
Disclosures and COI: There are no relevant financial interests or financial conflicts within the past 5 years and for the foreseeable future. The authors have no financial interests related to the material in the manuscript. There has been no funding support for this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.