


Article Figures & Data
Figures
- Figure 1
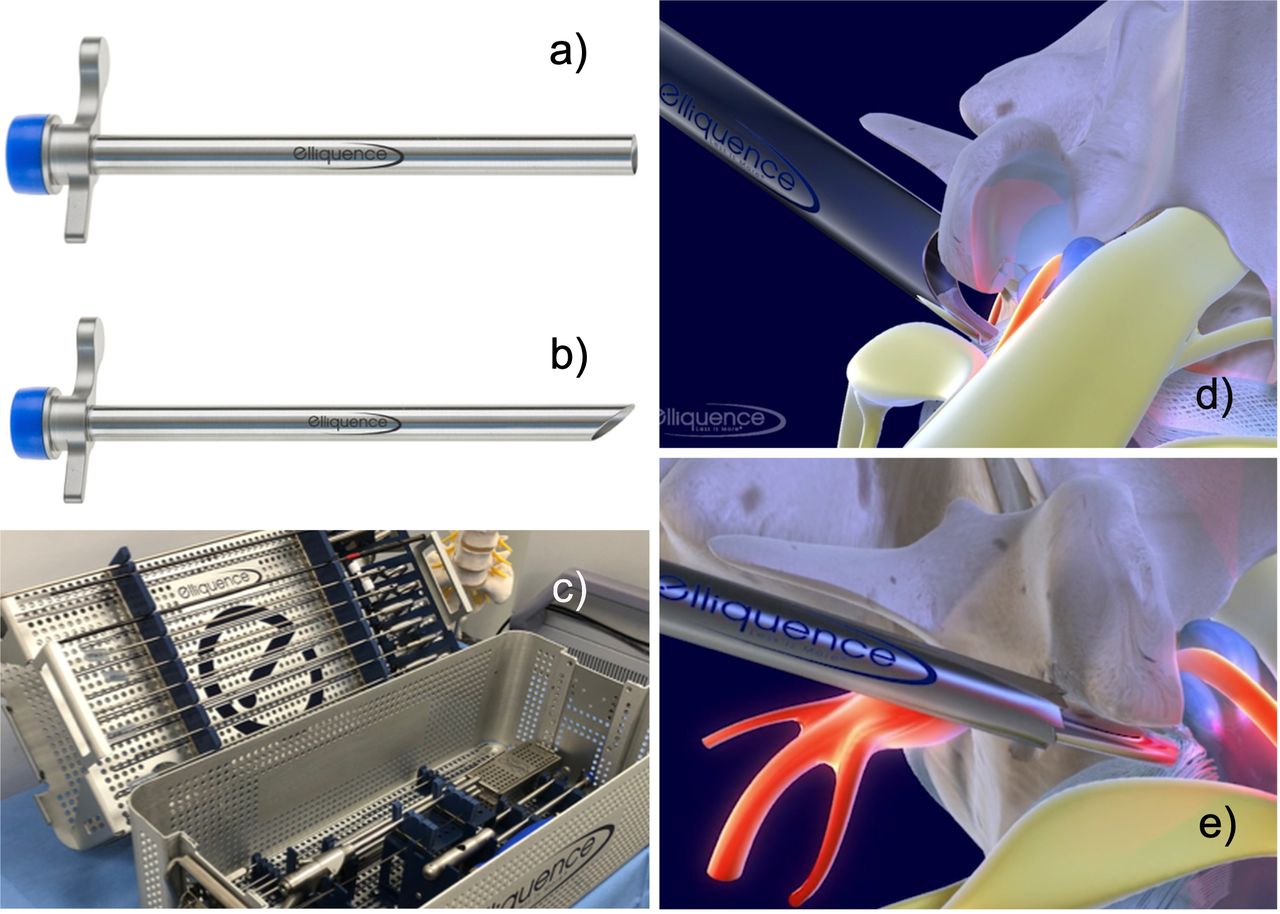
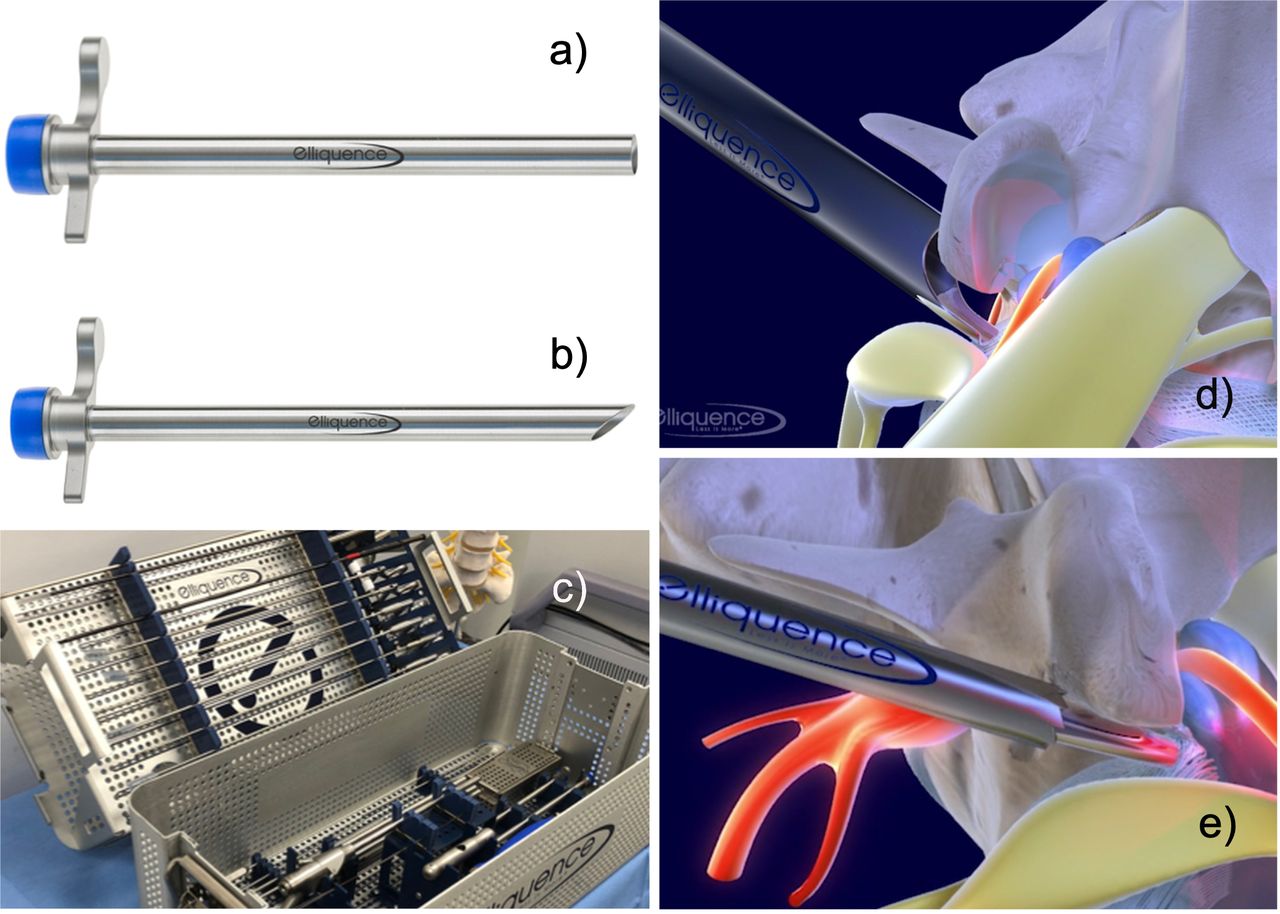
Endoscopic working cannulas resemble small tubular retractors with either 8.0- or 7.5-mm outer diameters and 7.1- or 6.5-mm inner diameters and are 165 mm in length. The endoscopic working sheath is offered with a straight (A), 40° beveled (B), or fenestrated tip. Several options are available in a standard lumbar transforaminal endoscopy tray (C). The beveled or fenestrated tip may be used to visualize and retract the exiting nerve root (D). Hydrostatic pressure and irrigation flow can be managed by attaching a plastic seal (blue cap) or by covering the end of the working cannula with the endoscopist’s thumb or a Luer lock stopcock when available. Trephines and rasps (E) can be used for a foraminoplasty when needed.
- Figure 2
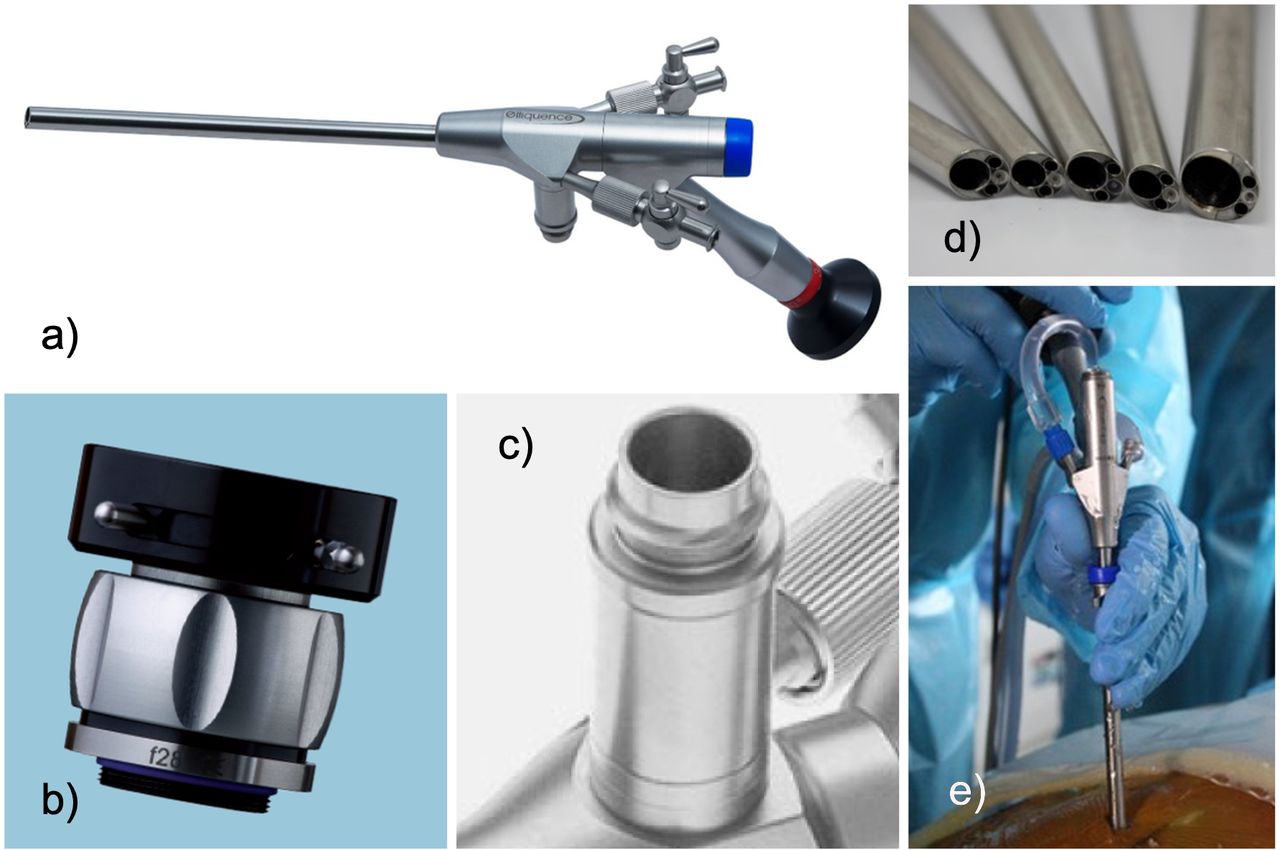
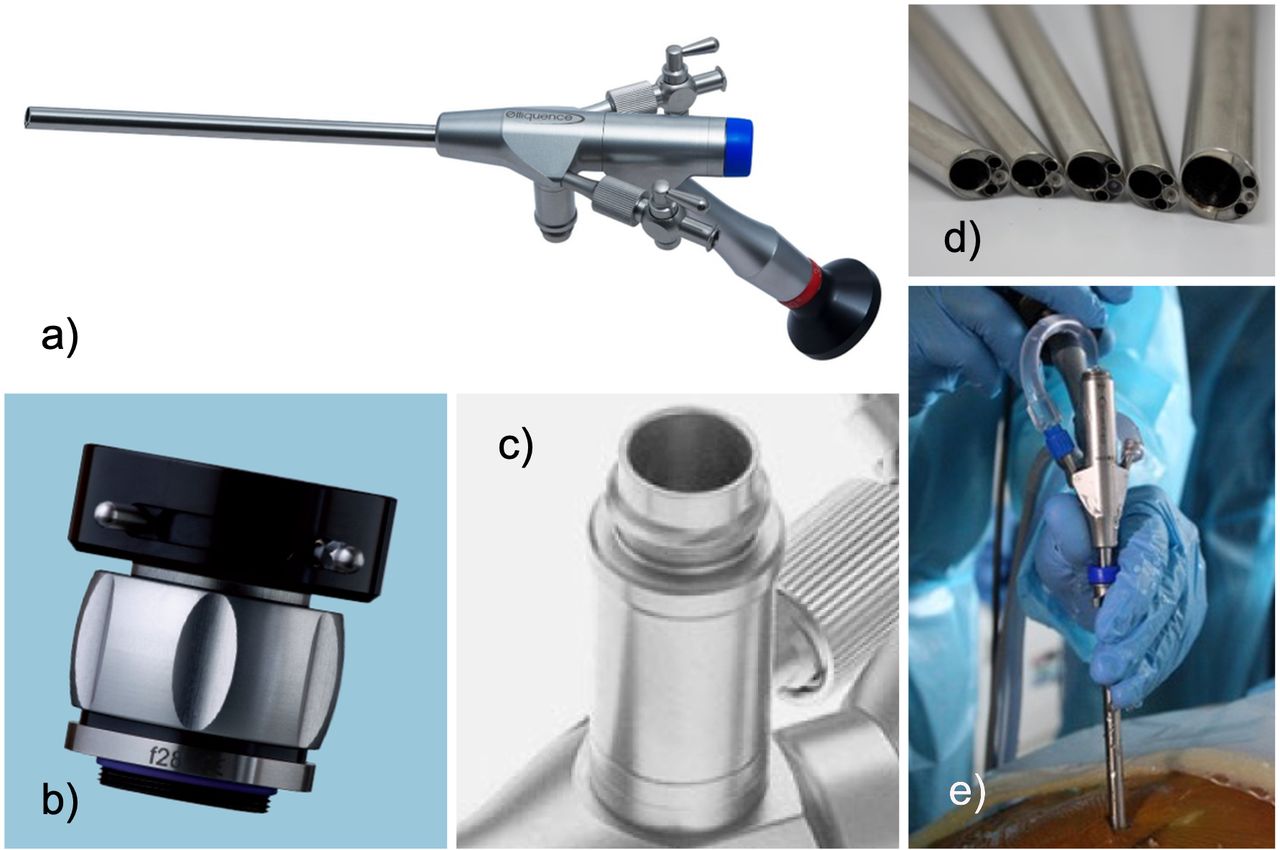
(A) Oval spinal endoscope (6.9 × 6.3 mm, length of 177 mm, 20° with one 4.1-mm oval working channel). A high-definition charge-coupled video camera can be attached to the HD-TV adapter (B). The light cable is connected via a standard coupler (C). Several configurations of the spinal endoscope with small and larger working channels are available, ranging from 3.7 to 6.9 mm. Typically, the lens between the light carriers is embedded in the sidewall of the endoscope (D). The ergonomic design of the lumbar foraminoscopes shown (E) allows the surgeon to rotate the endoscope easily without tangling up light and video cables when attempting to target painful spinal pathology.
- Figure 3
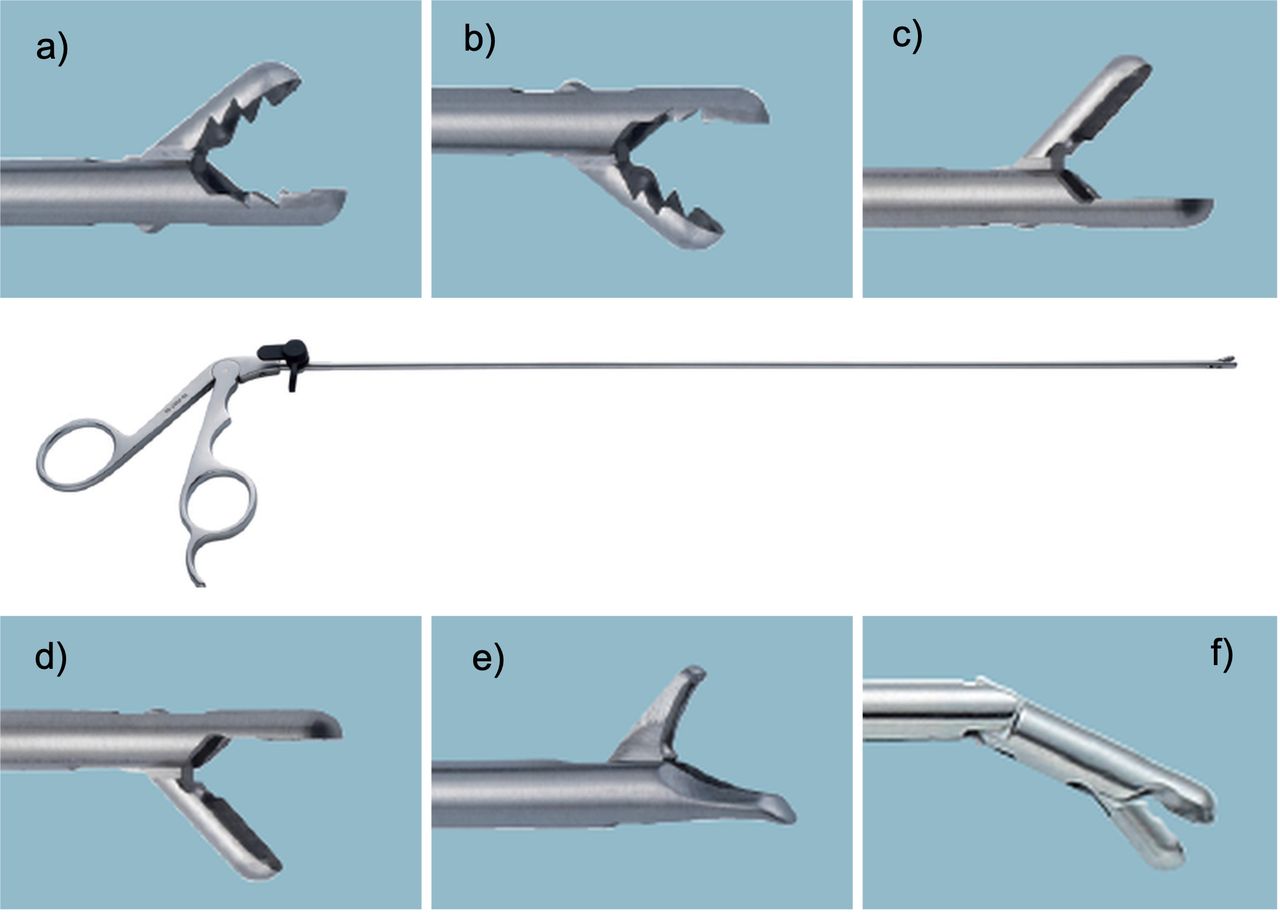
Commonly used grasping forceps designs: (A) 3.0-mm upbiter. (B) 3.5-mm downbiter. (C) 3.5-mm micro spoon upbiter. (D) 3.5-mm micro spoon downbiter. (E) 3.5-mm endoscopic punch. (F) Articulating grasping forceps with ratchet with a 5-mm jaw.
- Figure 4
The initial step of the transforaminal endoscopic approach to the lateral spinal canal is to place a guidewire into the triangular safe zone between the exiting and traversing nerve root (A). The optimum access trajectories angles for the L3-4, L4-5, and L5-S1 levels are shown in the axial (B), sagittal (C), and coronal plane (D). It is best to measure these trajectory angles on the patient in the posterior-anterior plane (E, F) and in the lateral plane (G, H). These determined access lines should be drawn on the patient in both the posterior-anterior and lateral fluoroscopic projection (F, H).
- Figure 5
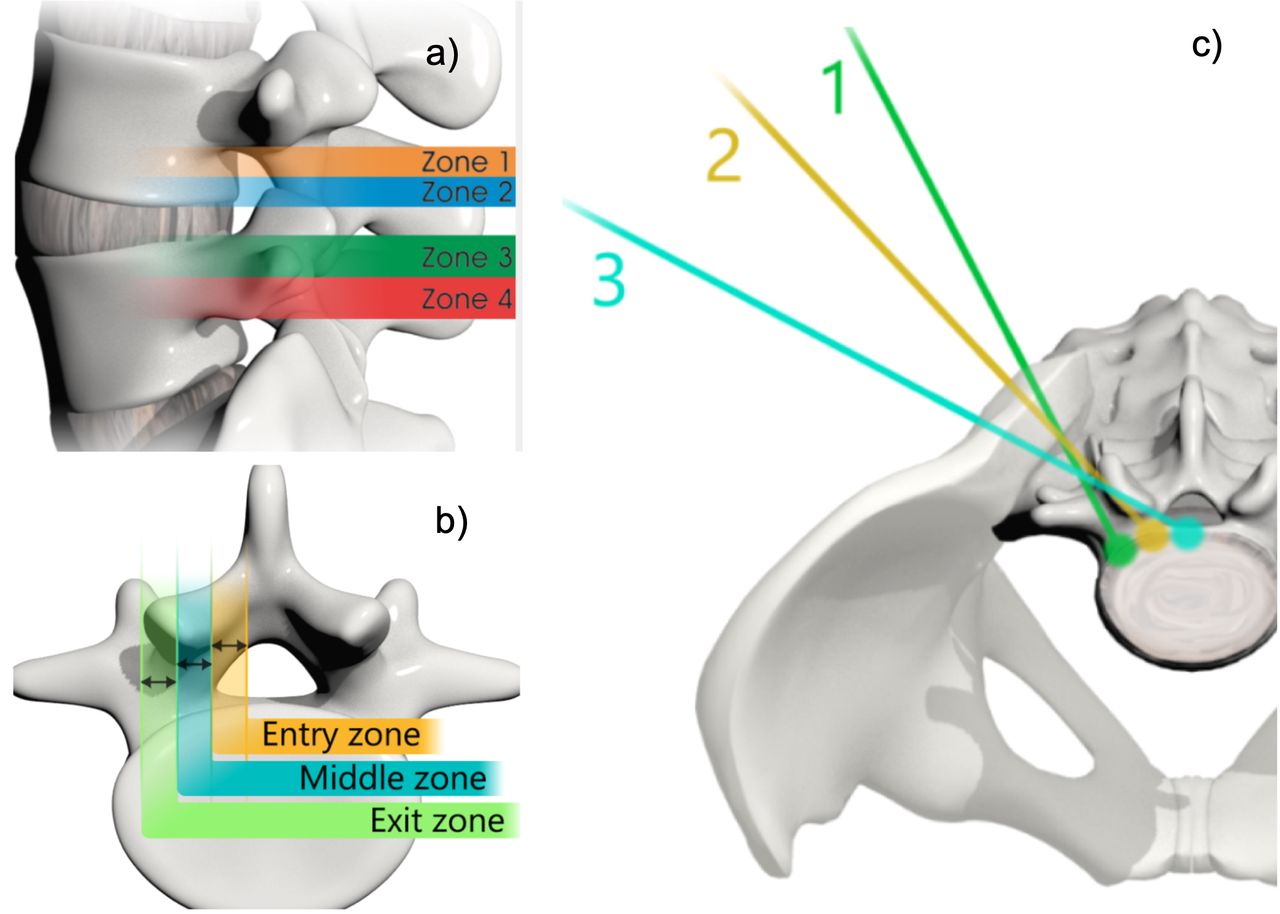
The assessment of cranial-caudal localization of a pathology such as a herniated disc may dictate whether the surgeon should choose a steep or shallow craniocaudal angle (A). Lee et al published a magnetic resonance imaging classification system of herniated discs to direct the endoscopic access. This classification categorizes the disc migration into 4 zones, depending on the direction and distance from the disc space (Table 1). Lee’s classification of foraminal stenosis (B) can be used to define the location of the offending bony pathology within the neuroforamen by dividing it from medial to lateral into entry (dura to pedicle), middle (medial pedicle wall to center pedicle), and exit zones (center pedicle to the lateral border of the facet joint). Bony foraminal stenosis in the entry, middle, and exit zones is frequently due to hypertrophy of the superior articular facet, an osteophytic process underneath the pars interarticularis, and a subluxed and hypertrophic facet joint, respectively (Table 2). The skin entry point can be chosen from the midline depending on the location of the herniation in the entry, middle, or exit zone of the neuroforamen (B, C). Assessing the pathology on axial views allows the distance of the entry point from the midline to be determined (C).
- Figure 6
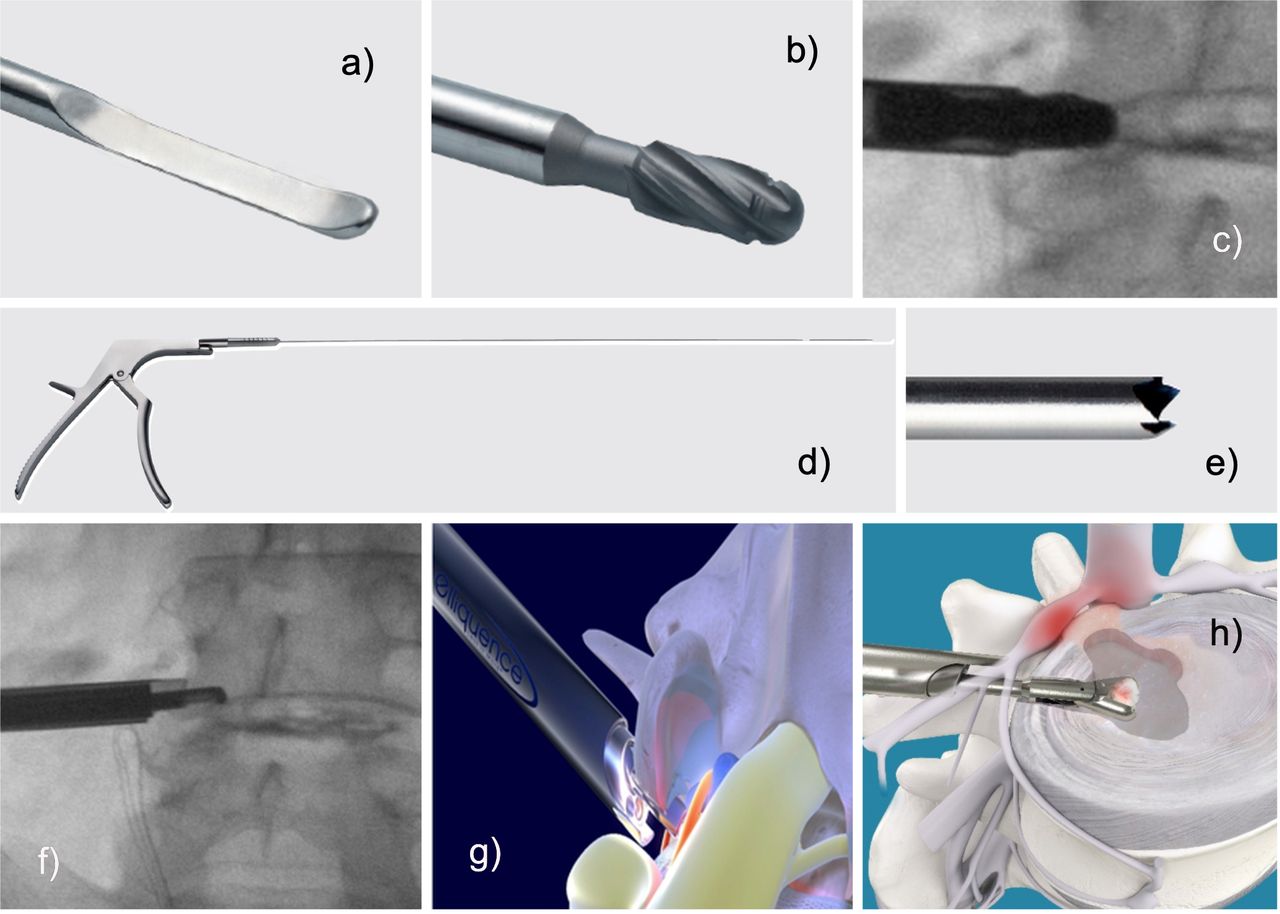
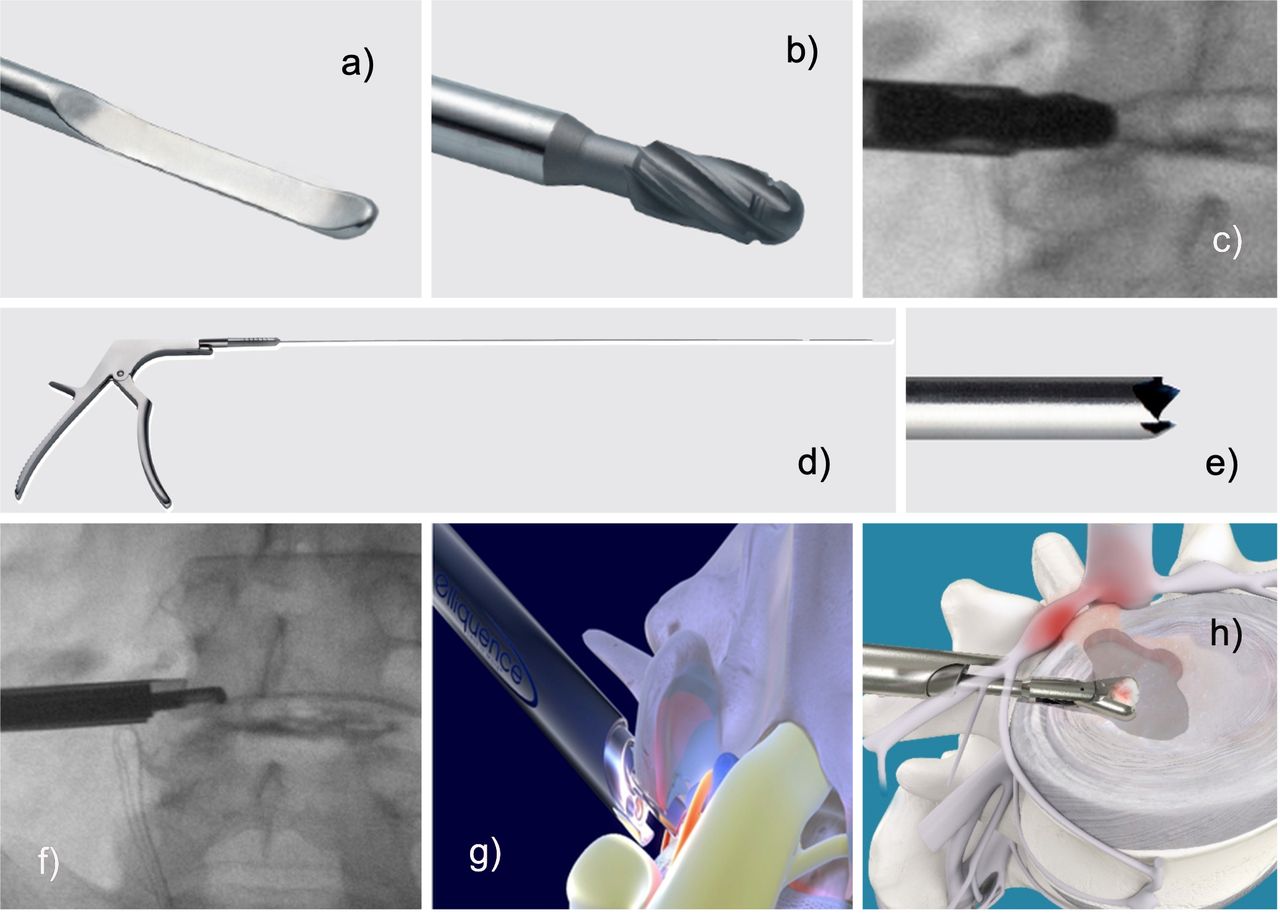
Foraminal decompression can be facilitated with endoscopic dissecting tools (A). Facet raspers (B, C) and Kerrison rongeurs (D, F) are helpful to remove bone and soft tissue. Trephines (E) may also be beneficial. Typically, these maneuvers play out at the superior articular process or the inferior pedicle. Finally, the removal of disc tissue may commence once the intervertebral disc is sufficiently exposed (H). The lateral recess decompression may involve bony resection (F, G) from the superior articular process or the ring apophysis below the traversing nerve root to accomplish adequate decompression.
- Figure 7
Several challenging case scenarios are shown that the novice spine surgeon should not attempt until a sufficient level of proficiency has been achieved: (A) A paracentral disc herniation should be treated with a targeted fragmentectomy. (B) An upward-migrated disc herniation should be tackled with the exiting nerve root approach, employing a round working channel to protect the exiting root. The axilla should be carefully inspected. (C) A downward-migrated disc herniation is best treated with a targeted fragmentectomy by accessing the epidural space via aggressive foraminoplasty. (D) For far-lateral herniated decompression, the exiting nerve root approach is preferred with a round working channel to protect the exiting root. (E) A facet cyst should be treated via the transforaminal approach with foraminoplasty to identify and remove the stalk of the cyst. (F) A large central herniated disc causing severe central canal compromise should be treated via the outside-in transforaminal approach. Expect multiple fragments. (G) A foraminal herniated disc is also best approached via the exiting nerve root, employing a round working channel. The decompression is complete once the remnant disc behind it is identified. (H) Focally calcified lumbar disc herniation should be removed using the punch and rongeur. Very large calcified disc herniations may have to be drilled down with a shaver or burr.
- Figure 8
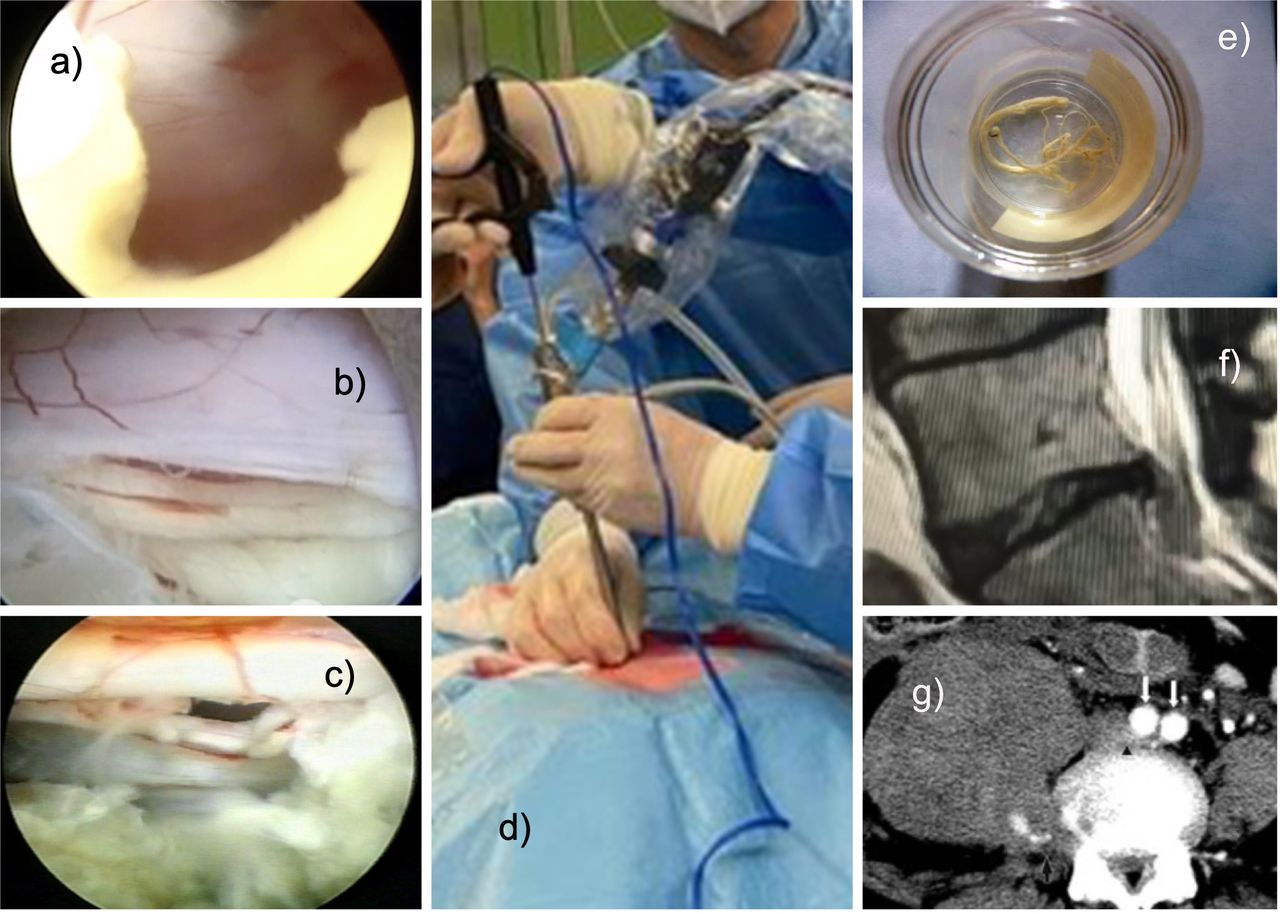
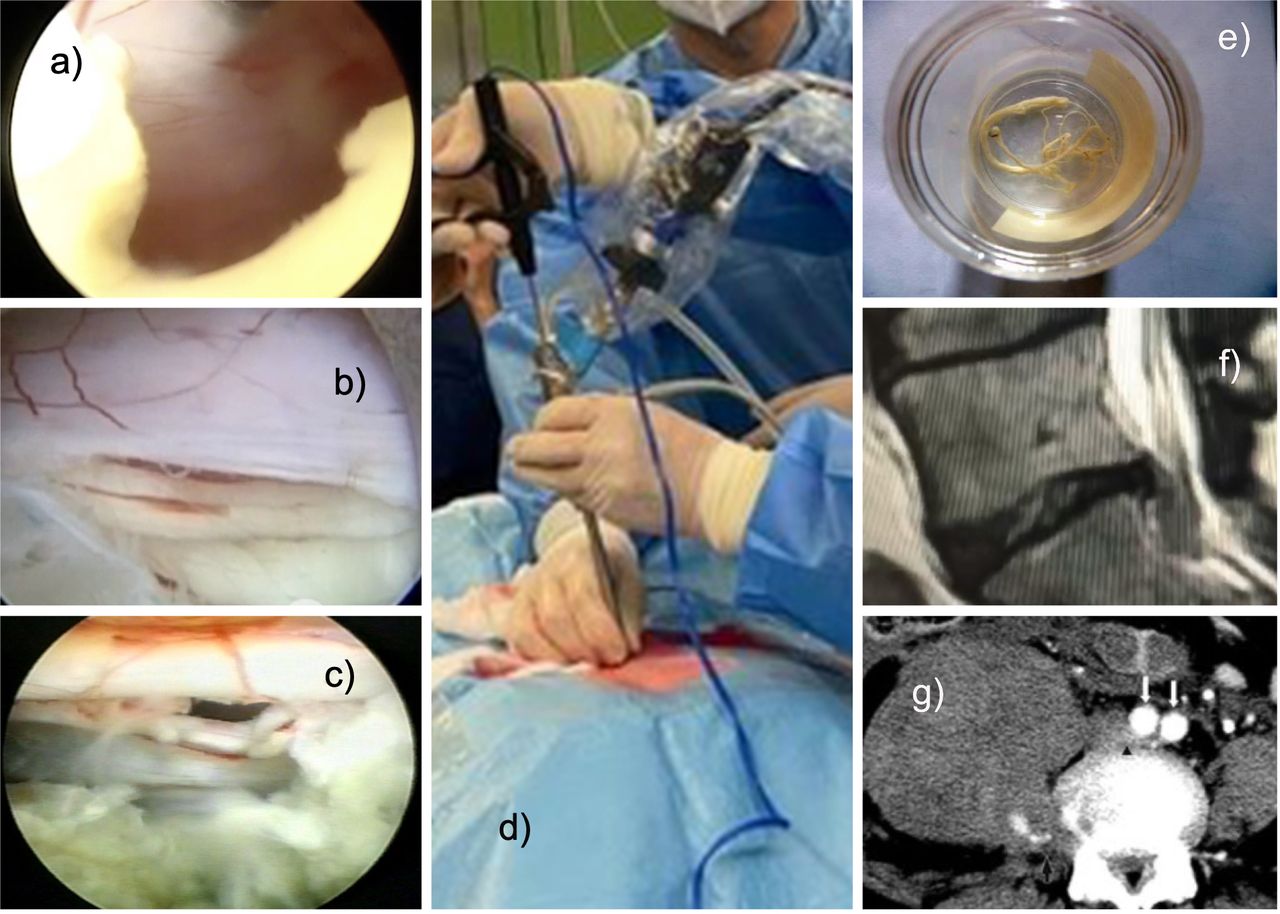
Intraoperative complications are rare during lumbar endoscopic decompression surgery. The interlaminar approach (D) has a higher risk of incidental durotomy (A–C). It typically occurs with the use of power burrs. During the interlaminar approach, care must be taken not to cause an incidental durotomy when perforating the ligamentum flavum (A). During the transforaminal approach, small incidental durotomies typically occur in the axilla between the exiting and traversing nerve root, the hidden zone of Macnab (B, C). Rarely, true rootlet herniations may occur. Power burrs or drills are notorious for wrapping up rootlets around the spinning tip of the instrument (E). Other examples of postoperative complications include recurrent disc herniation (F) and retroperitoneal hematoma from accidentally severing the segmental vessels located in the lateral aspect of the vertebral bodies of the surgical level (G).
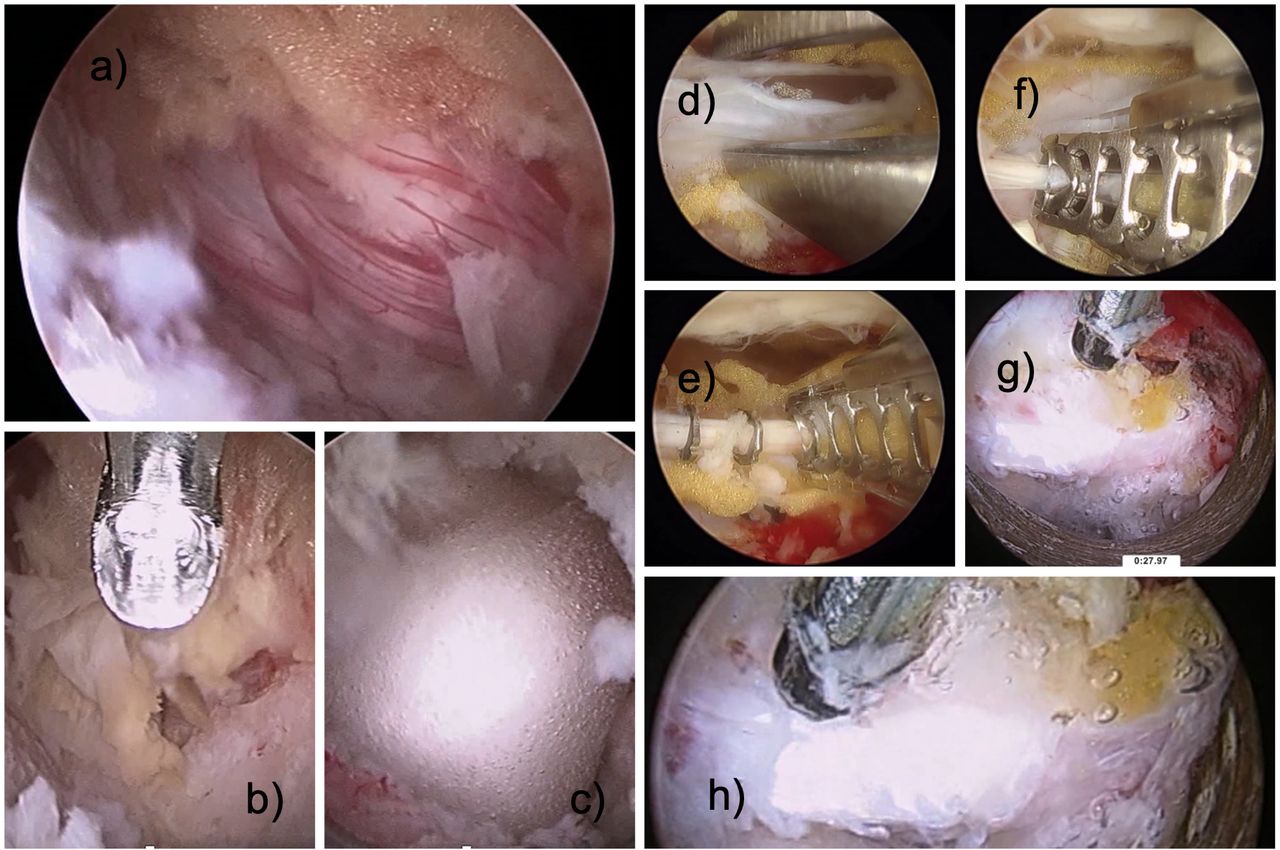
- Figure 9
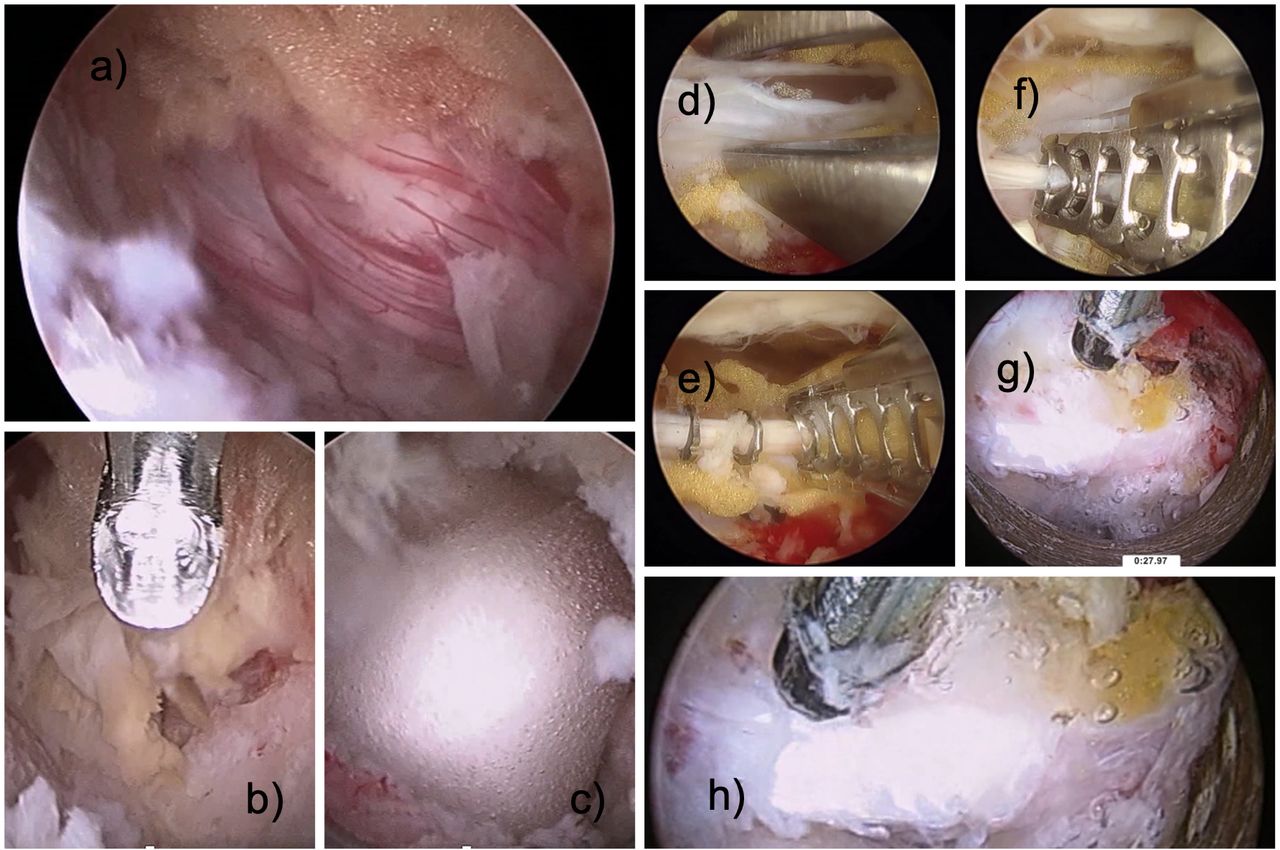
Interlaminar decompression is associated with a high risk of tears in the posterior dural sac (A). The durotomy may occur during the medial facet resection of a hemilaminectomy (B). Durotomies may be treated with a sealant (C), approximated with a bipolar probe (D), and secured with clips (E, F) or stuffed with sealant foam that can be shrunk into the durotomy site (G, H).




Tables
Zone Direction Range of Distance Zone 1 Far-upward From the inferior margin of the upper pedicle to 3 mm below the inferior margin of the upper pedicle Zone 2 Near-upward From 3 mm below the inferior margin of the upper pedicle to the inferior margin of the upper vertebral body Zone 3 Near-downward From the superior margin of the lower vertebral body to the center of the lower pedicle Zone 4 Far-downward From the center of the lower pedicle of the lower vertebral body to the inferior margin of the lower pedicle - Table 2
Radiological classification of lumbar neuroforaminal and lateral recess stenosis according to Lee et al55 and Hasegawa et al.57
Zone Location Range of Distance Zone 1 Entry From dura to pedicle Zone 2 Middle From medial pedicle wall to center pedicle Zone 3 Exit From center pedicle to the lateral border of the facet joint
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.