


Abstract
Background Osteoid osteoma (OO) is a common benign bone tumor; however, approximately 25% of cases have spine involvement. It is often treated by image-guided radiofrequency ablation to break down the nidus. Few reports have described full endoscopic resection of the lesion, but none have described postoperative remodeling of the lumbar facet joint after surgical resection of an OO. The study aimed to describe a rare case of remodeling of the lumbar facet joint and then delineate the least invasive surgical technique of endoscopic resection of an OO.
Methods A 26-year-old man presented with severe left buttock pain and sciatica that worsened at night and was relieved by ibuprofen. Magnetic resonance imaging indicated a left inferior facet of an L3 mass-like lesion. A thin-section computed tomography image revealed a nidus, which was compatible with an OO. Full endoscopic resection was performed to completely remove the nidus of the OO.
Results At the 2-year follow-up, the patient was symptom-free and computed tomography images indicated new bone formation.
Conclusions The present case and literature review demonstrate that endoscopic resection is safe and effective for managing a posterior element of lumbar OO. Furthermore, this technique allows complete removal of the nidus with minimal damage to surrounding structures and leads to remodeling of the resection site.
Clinical Relevance Patients with OO involving the posterior element of the spine can present with buttock and radicular pain, mimicking lumbar disc herniation. OO can be successfully removed by the full endoscopic method and remodeling of the resected site can be anticipated.
Level of Evidence 4.
- osteoid osteoma
- full endoscopic resection
- endoscopic resection
- minimally invasive spine surgery
- lumbar
- remodeling
- facet joint
- nidus removal
INTRODUCTION
Osteoid osteoma (OO) is an uncommon benign bone tumor that accounts for 3% of all primary bone tumor lesions. It is usually located in the long bones of lower extremities in children and young adults, particularly in male patients.1,2 Spinal involvement has been reported in 10%–25% of cases, most frequently affecting the posterior element of the lumbar vertebrae and rarely involving the vertebral bodies.3–5 Localized back pain is typically worse at night and is relieved with nonsteroidal anti-inflammatory drugs (NSAIDs) or salicylates.4,6–8 Computed tomography (CT)-guided radiofrequency ablation (RFA) has become the preferred treatment for OO. However, RFA use in the posterior element of the spine, which is closer to the nerves, requires careful attention because of heat production.
We describe a successful full endoscopic resection of an OO in the inferior articular process of the lumbar spine. CT imaging obtained 2 years postoperation indicated a new bone formation at the facet joint. Furthermore, we completed a systematic literature review regarding OO.
METHODS
The PubMed database was searched using the following terms: osteoid osteoma and (spine or vertebral) and (excision or resection or curette or ablation or coagulation or microscopic or endoscopic). Article reference lists were reviewed and assessed using the selection criteria.
Eligible studies included patients who underwent any surgical procedure for spinal OO. Inclusion criteria were human subject study and published in English. Studies were excluded if they did not report clinical outcomes, did not focus on spinal involvement as the OO location, and focused on the medical treatment. Abstracts and editorials were also excluded.
Case Presentation
A 26-year-old man with a 7-month history of progressive severe left buttock pain and sciatica that worsened at night and was relieved by ibuprofen. Magnetic resonance imaging indicated a mass-like lesion with peripheral soft tissue edema at the left inferior articular process of L3 vertebra (Figure 1). Thin-section CT indicated a 1-cm nidus compatible with an OO (Figure 2A). After obtaining consent, the patient was scheduled for minimally invasive full endoscopic resection of the OO.
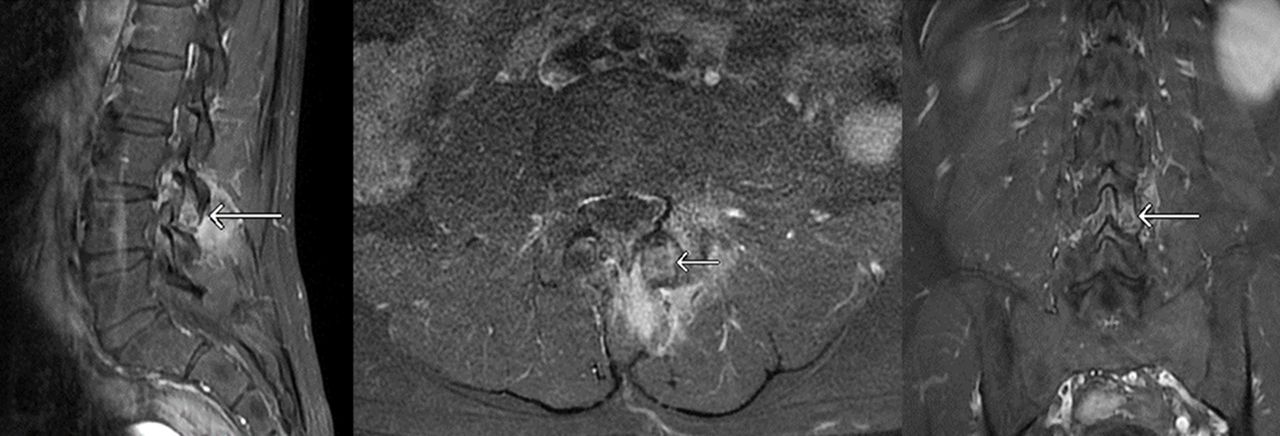
Magnetic resonance imaging images (T1-weighted fat suppression (T1FS) postgadolinium) show significant enhancement around the mass-like lesion at the left inferior articular process of the L3 vertebra.
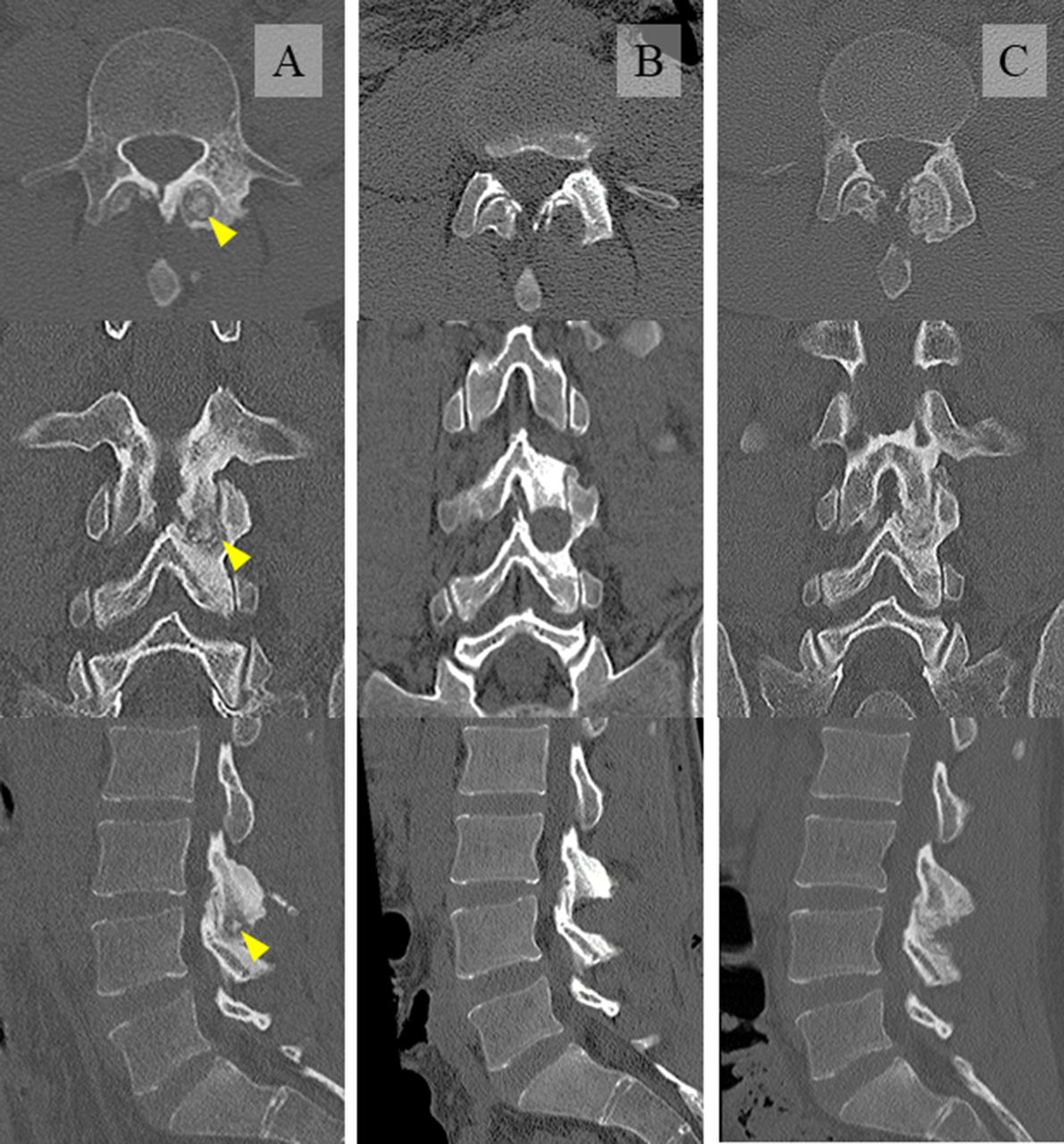
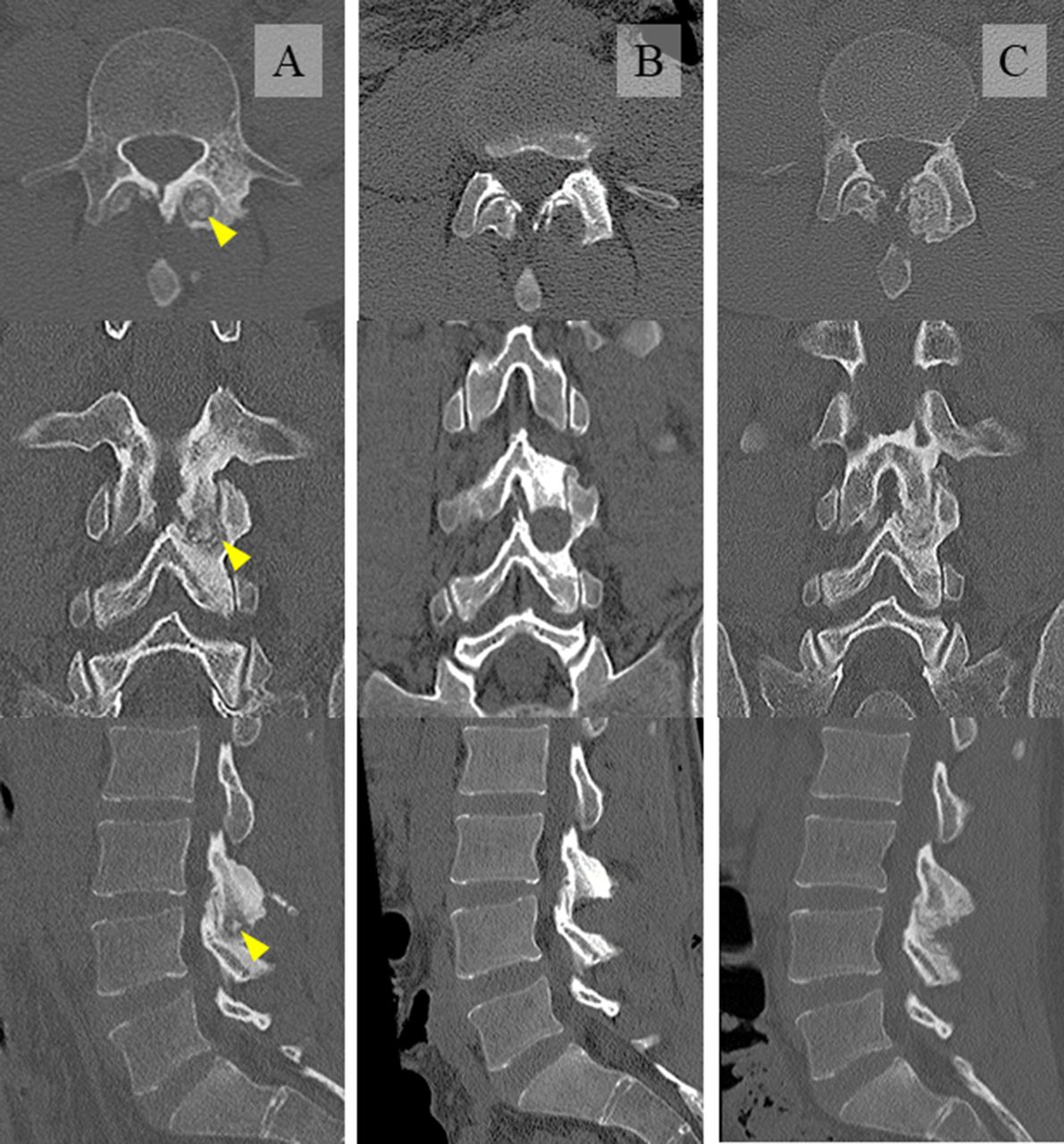
Computed tomography image comparison. (A) Preoperative image with a notable “nidus” (yellow arrowhead), (B) immediate postoperative image, and (C) 18-month postoperative image showing remodeling of resected area.
Surgical Technique
Preoperative measurements of the nidus using CT and magnetic resonance imaging were used for intraoperative correlation. Under general anesthesia, the patient was placed in a prone position. The index level of surgery was located using fluoroscopy, and the skin was marked. After adequate antiseptic skin preparation and draping, the index level was rechecked. A 7-mm stab incision was made approximately 1.5 cm from the midline. A soft dilator was inserted, followed by a working cannula. The fluoroscope was turned to identify the lateral view, which aided the craniocaudal orientation. The endoscope was later inserted through the working cannula. Water pressure and flow were set at 60–90 mm H2O and 0.6–1.0 L/min, respectively, during surgery.
Muscle dissection was performed using the dissecting radiofrequency probe and pituitary rongeur. After the tumor mass at the inferior articular process of L3 was clearly exposed (Figure 3), bone work was performed. The nidus was partly removed using a diamond head burr (Figure 4). A pituitary rongeur was used to remove and collect the nidus tissue for pathological examination (Figures 3 and 4). The nidus was thinned down until normal bone was reached. Four-megahertz bipolar radiofrequency coagulation and ablation were applied over the raw surface of the bone to ensure remnant ablation (Figures 3 and 4). The decompression surface was rechecked thoroughly, bleeding points were controlled, and the skin was closed in subcutaneous fashion. The operation time was 40 minutes, and the estimated blood loss was 10 mL.
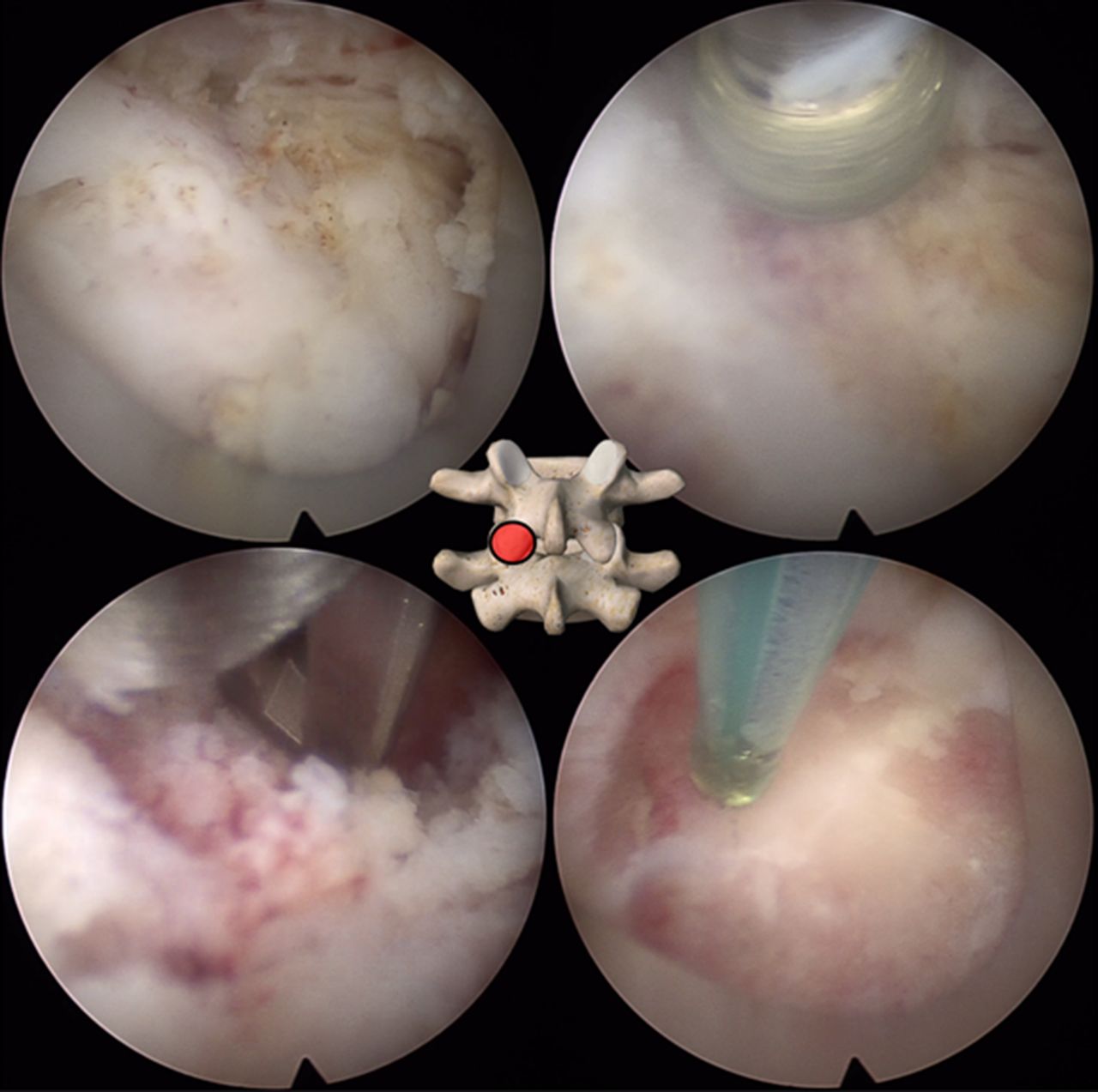
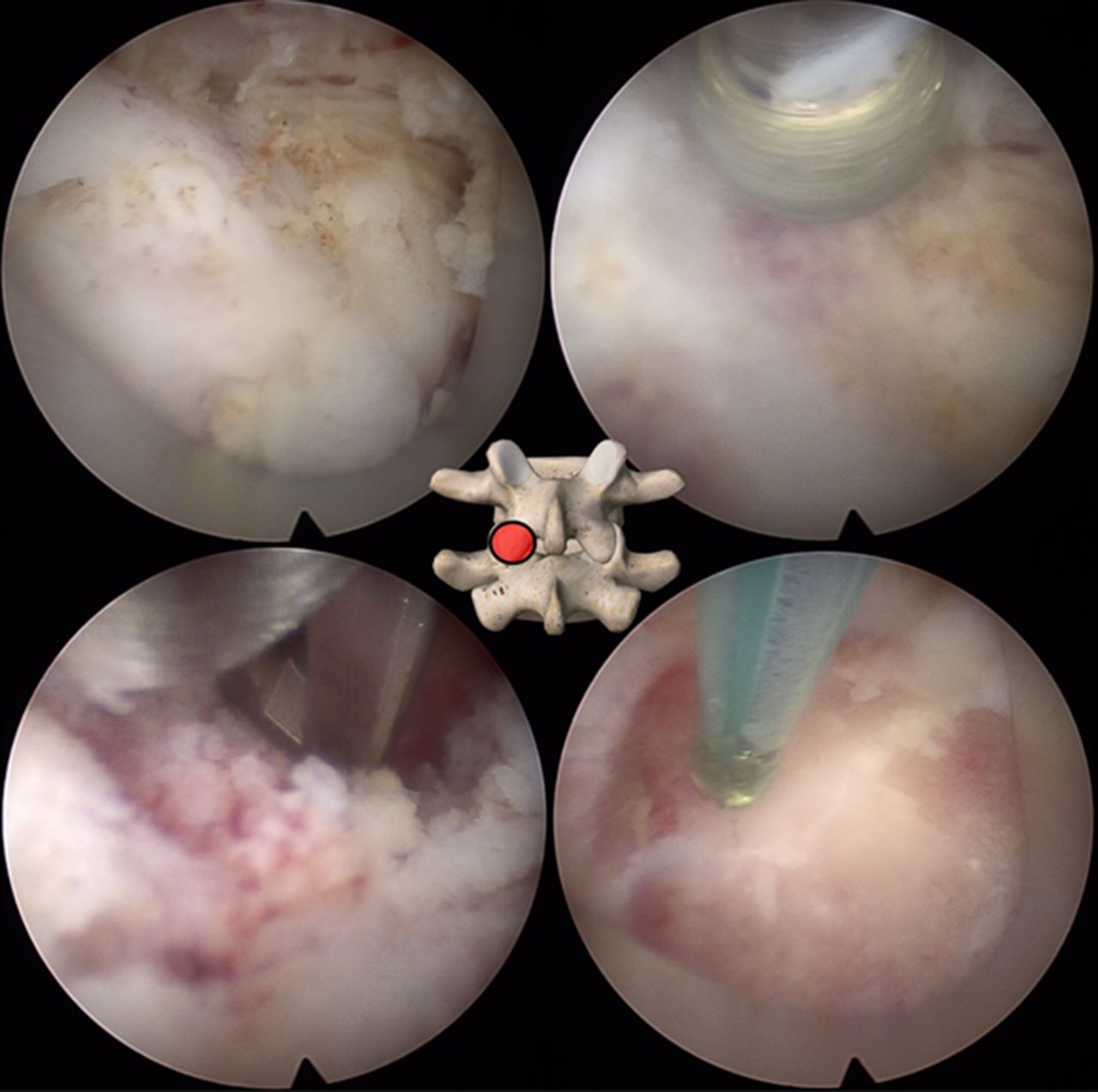
Intraoperative endoscopic views. Tumor mass after tissue dissection (top left). Diamond tip burr use (top right). Kerrison rongeur nidus removal (bottom left). Radiofrequency cauterization after nidus removal (bottom right). Orientation and working area (middle).

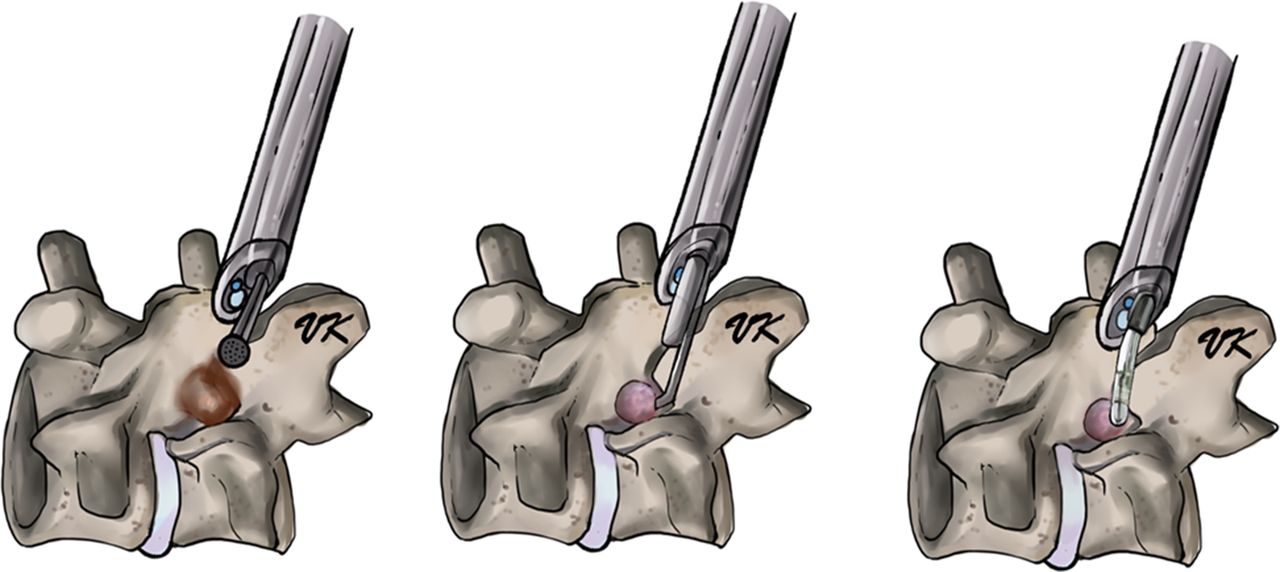
Schematic of endoscopic procedure at L3 left inferior articular process shows diamond tip burr, Kerrison rongeur, and radiofrequency electrocautery.
The following day, the patient’s symptoms completely resolved, and he was discharged from the hospital with minimal physical restrictions. An immediate postoperative CT image revealed that the inferior articular process was resected in a round shape (Figure 2B). The pathological report confirmed the OO diagnosis (Figure 5). At the 2-year follow-up, the patient was symptom-free and had no limitations of back movements or daily activities. Interestingly, CT images revealed remodeling of the left inferior articular process of L3, without local recurrence of the tumor (Figure 2C).
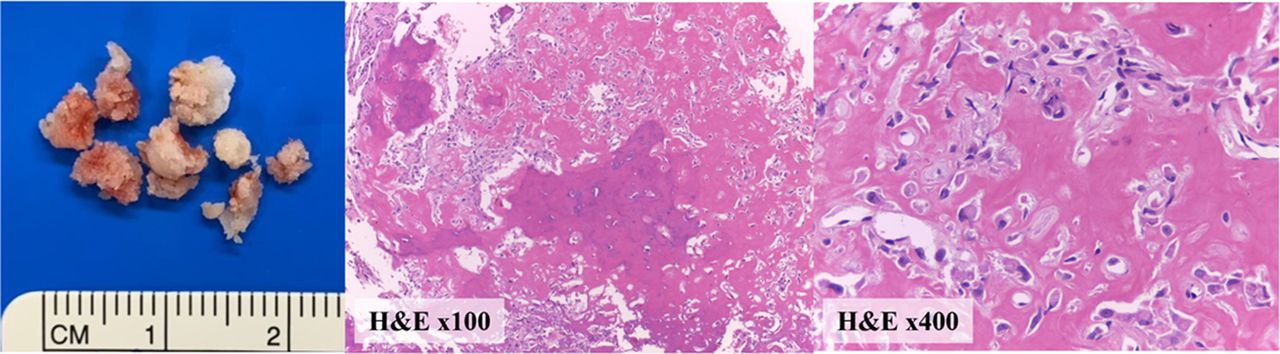
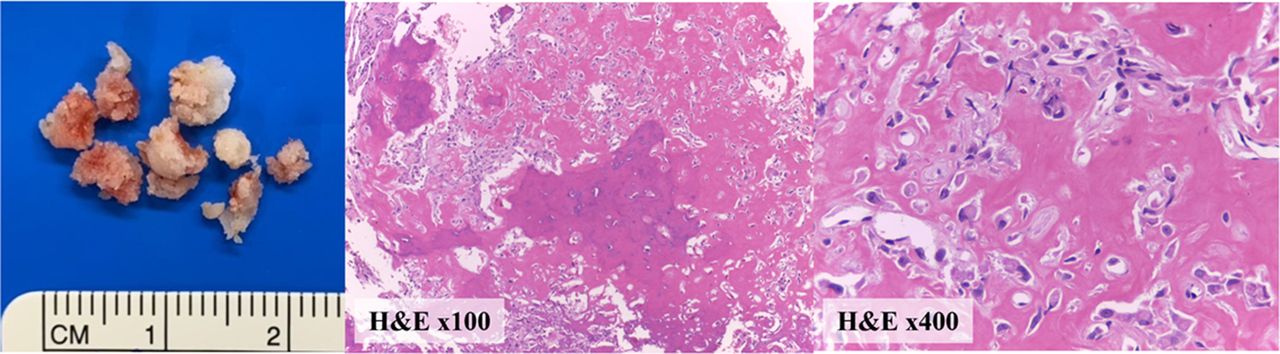
Pathology and microscopic views. Microscopic examination with hematoxylin and eosin stain revealed fragments of nodular lesion, composing anastomosing network of irregular trabeculae of woven bones with variable mineralization and central loose fibrovascular stroma. Layers of osteoblasts and sporadic osteoclasts rim the trabeculae of woven bone.
DISCUSSION
OO of the spine mostly affects the posterior lumbar vertebrae. Radiographically, it appears as a small radiolucent lesion or a nidus <15 mm in diameter and is characterized by a central nidus surrounded by a sclerotic reactive bone, comprising osteoid, osteoblasts, and fibrovascular stroma.5,6 Patients usually present with back pain that worsens at night and is well relieved with NSAIDs. In cases of spinal OO located close to a nerve root, back pain can radiate distally and cause radiculopathy, mimicking disc herniation, making diagnosis difficult and thus delay appropriate treatment initiation.1,6,9–11 Our patient also presented with localized low back pain with radiculopathy that was relieved with ibuprofen. Imaging revealed a 1-cm nidus lesion involving the left inferior articular process of L3, compatible with lumbar OO.
In patients who are refractory to medical treatment or in whom NSAIDs and salicylates are contraindicated, surgical management is usually curative. Many options for surgical excision of spinal OO have been proposed: intralesional curettage, marginal or wide resection, and thermoablation including percutaneous RFA or laser coagulation.3,9,12 Conventional procedures for open surgical excision often require paraspinal muscular detachment and facet disruption to perform complete resection of the nidus as the principle of treatment to achieve pain remission.13 This affects spinal stability and necessitates spinal fusion and instrumentation, which is associated with increased blood loss, longer operative time and length of hospital stay, loss of spinal motion, and long-term complications including heterotopic ossification and adjacent segment disease.3,4,14
In this article, we demonstrated the complete excision of a lumbar (L3) OO at the inferior articular process using a full endoscopic technique. Our patient presented with left buttock pain and sciatica, which were relieved but not improved by medical treatment. Postoperatively, the buttock pain and sciatica were completely relieved the next day and no complications were observed. The patient was free from pain with full regular activities at the 2-year postoperative follow-up. Two-year postoperative three-dimensional CT images showed no local recurrence of the tumor and revealed remodeling at the resected area.
In recent years, minimally invasive surgical techniques for resection of spinal OO have been proposed and considered the preferred treatment.3 Thermoablation, including percutaneous RFA and laser coagulation, is effective to resect lesions with less bone destruction. Many image-guided RFA techniques, such as CT-guided RFA and navigational bipolar RFA electrode system, are available to help locate the lesion more precisely without compromising spinal stability.1,6,9,15–17 However, RFA techniques can be dangerous, especially when the lesion is near neural or vascular structures and may cause postoperative neurological deficit.1,2,18
Endoscopic surgery for excision of the spinal OO minimizes the morbidity associated with other surgical techniques.19 Many reports following this approach in the cervical, thoracic, and lumbar spine have shown successful results with low complications.3,19–23 Kalkarni et al reported an OO case involving C2 lamina and lateral mass, which was completely excised with microendoscopic excisional biopsy, with excellent pain relief without compromising the stability.24 Hikata et al reported a CT finding of resection site remodeling after total microendoscopic resection of the nidus without tumor recurrence.22 Yoshioka et al presented an OO case located in the L3 pedicle manifesting as lumbar radiculopathy.20 The patient underwent complete microendoscopic excision, and the pain disappeared immediately postsurgery. Xie et al reported a series of 11 patients with lumbar OO who underwent endoscopic excision and subsequent ablation around the residual osteoma cavities.3 All patients reported immediate pain relief without serious complications.
While many effective minimally invasive techniques have been described for complete resection of the nidus with minimal damage to soft tissue and bone, this is the first case to describe bone remodeling of the lumbar facet joint after excision at 2-year follow-up.
Four phases of bone remodeling were observed and classified by Engel et al. The final phase is the complete bone remodeling following tumor removal, possibly suggesting the success of the procedure; this is well known to be associated with the blood supply to the bone.25 Injury to the blood supply to the bone could impede the osteoblast function and bone formation. In contrast to other surgical resection techniques for OO, the distinct advantage of the full endoscopic technique is that it is currently the least invasive procedure to effectively remove the tumor while providing minimal damage to surrounding structures including soft tissue, normal bone, and preserving blood supply to the bone. This positively affects the result of the operation, including less risk of iatrogenic mechanical instability or fractures, less hospitalization, and more preserved biological bone healing process, which reduces time for bone remodeling, compared with other resection techniques.
CONCLUSIONS
Full endoscopic resection is an effective minimally invasive treatment for posterior lumbar OO. It minimizes damage to surrounding soft tissue and bone and allows remodeling of the resected site after a complete nidus resection.
Acknowledgments
The authors would like to acknowledge the “CU Spine Conference” line group for an open and friendly discussion about spine cases.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Jin-Sung Kim is a consultant for RIWOSpine, GmbH, Germany, and Elliquence, LLC, USA. The remaining authors have nothing to declare.
Disclosure The authors report no financial disclosures related to this article.
Ethics approval Ethical approval was obtained from Queen Savang Vadhana Memorial Hospital’s ethical committee (EC no: 2020/30).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}