


Abstract
Background The choice of surgical method for the treatment of multilevel degenerative cervical spine disease is based on the assessment of neurological symptoms and anatomical source of compression. However, such decision-making process remains complex and poorly defined.
Purpose To analyze the effectiveness of an algorithmic posterior approach to the surgical treatment of patients with multilevel degenerative disease of the cervical spine based on the preoperative clinical and imaging parameters.
Study Design Prospective nonrandomized multicenter cohort study.
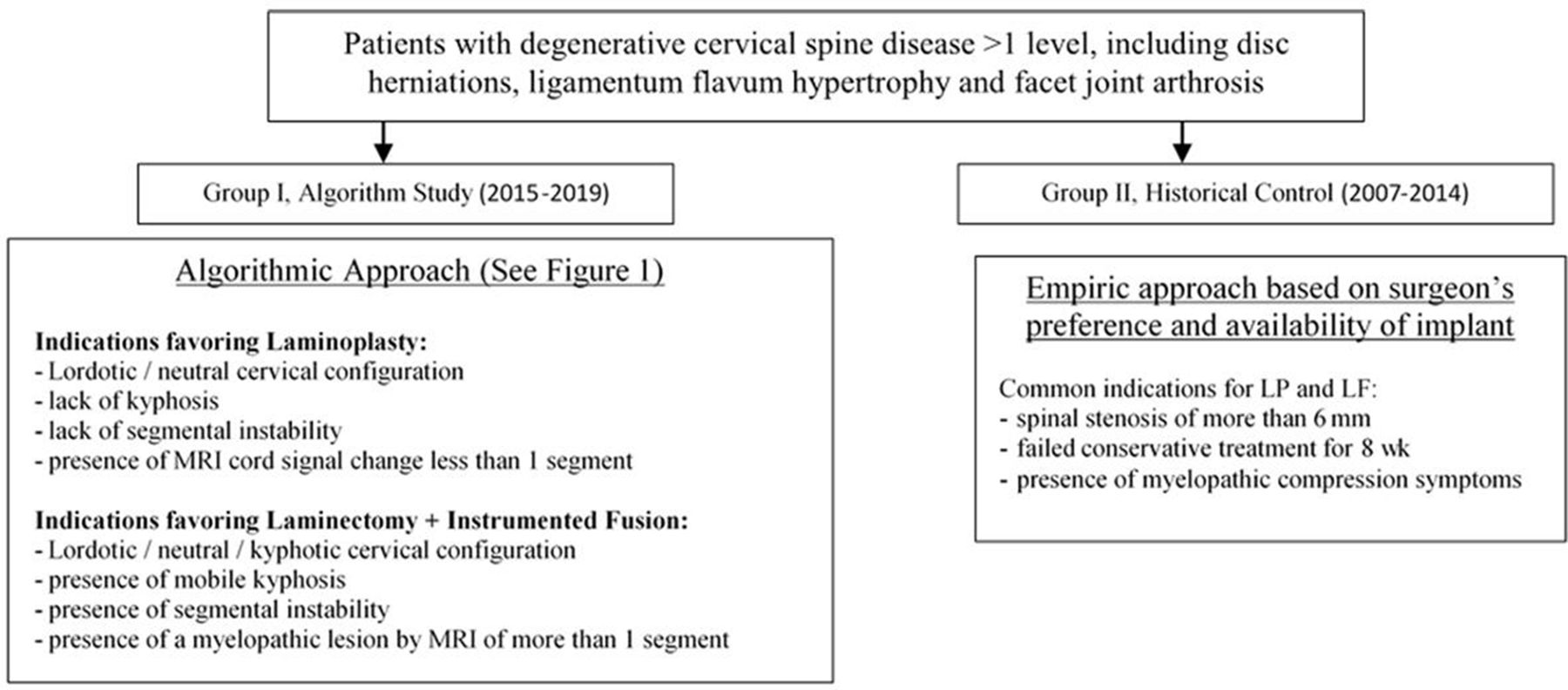
Methods The study included 338 patients with multilevel degenerative disease of the cervical spine. Two groups of patients were evaluated at 3 neurosurgical centers between 2015 and 2019. The prospective group (Group I, n = 214) consisted of patients who were treated using an algorithm to decide whether they should be treated with an instrumented arthrodesis or a nonfusion procedure. The control group (Group II, n = 124) consisted of patients who underwent posterior decompression with or without stabilization between 2007 and 2014. A total of 192 patients in Group I and 112 in Group II had more than 2 years of follow-up. Visual analog scale (VAS) neck pain, Neck Disability Index (NDI), MacNab and Nurick Scales were collected. Perioperative complications were identified.
Results At 2-year follow-up, Group I had significantly better clinical outcomes based on VAS neck pain score (P = 0.02), NDI score (P = 0.01), satisfaction with surgery on the MacNab Scale (P < 0.001), and outcome of surgery based on the Nurick Scale (P < 0.001). Complication rate was lower in Group I, 5.7% compared with 34.8% in Group II, P = 0.004.
Conclusions The algorithmic posterior approach to the surgical treatment of patients with multilevel degenerative disease of the cervical spine resulted in significant improvement of functional outcomes and a decrease in complications at a minimum 2 years of follow-up.
Level of Evidence 2.
- cervical spinal stenosis
- posterior cervical decompression
- laminoplasty
- cervical fusion
- surgical algorithm
INTRODUCTION
The optimal surgical treatment of degenerative cervical spine disease, accompanied by neurological symptoms such as radiculopathy or myelopathy, remains controversial.1,2 Common surgical interventions for cervical stenosis include ventral procedures such as anterior cervical discectomy and fusion and corpectomy, as well as dorsal ones, including laminoplasty (LP) and laminectomy with lateral mass fixation (LF).3,4 The choice of surgical treatment for a degenerated cervical spine depends on numerous factors, including surgeon preference, the severity of degenerative changes in the supporting elements of the vertebrae, spinal alignment, the number of affected segments, and the presence and severity of morphological changes in the spinal cord.5,6
Currently, there are few well-established guidelines regarding the choice of operation for multilevel degenerative cervical pathologies.7 A substantial percentage of unsatisfactory results necessitating revision surgical procedures adversely impacts the long-term outcomes.8 We had previously examined the causes of unsatisfactory outcomes following dorsal decompression, with and without stabilization in patients with multilevel degenerative disease of the cervical spine. They had been treated in the first author’s institution from 2007 to 2014 without any standardized protocol. A retrospective analysis of those patients found that those who had been treated with LP did best if they had the following characteristics: neutral or lordotic alignment of the cervical spine, absence of listhesis, magnetic resonance (MR) cord signal change less than 1 segment. On the other hand, the LF worked better in those with preoperative mobile kyphosis, instability, and the presence of MR signal change in the spinal cord of greater than 1 segment. Based on these findings, we came up with an algorithm that took into account all of these factors. We have confirmed that the best clinical and instrumental outcomes are associated: in patients with C2-C7 lordotic angle <−10° and predominant anterior compression during ventral interventions; in the case of circumferential compression, as well as at C2-C7 lordotic angle >−10°, dorsal operations have advantages. Those who had rigid kyphosis did best with circumferential decompression and correction of kyphosis.9
Given the above, we believe that a treatment algorithm aimed at improving clinical results would be of benefit to spine surgeons. Since 2015, we have been utilizing and prospectively investigating the effectiveness of an algorithmic approach to the surgical treatment of multilevel degenerative disease of the cervical spine. The purpose of the study was to evaluate the results using the proposed algorithm in a prospective group in order to confirm the feasibility of eliminating risk factors for the formation of unsatisfactory outcomes in this category of patients.
MATERIALS AND METHODS
Patients Data
Prospective nonrandomized multicenter cohort study was approved by the ethics committee (Irkutsk State Medical University) (Protocol No. 2 dated 13 July 2015). Each patient gave voluntary consent to be included in the study. We developed an algorithm to guide the posterior treatment of multilevel degenerative cervical disorders and prospectively evaluated its efficacy with radiographic and clinical outcome instruments. The prospective group underwent procedures in a nonrandomized manner from 2015 to 2019 in the neurosurgical departments of 3 hospitals: Irkutsk (Russia), Vladivostok (Russia), and Almaty (Kazakhstan). To minimize the influence on the treatment outcome of patient selection factors, the experience of the surgeon, and the operating technique at the bases of the 3 departments, the outcomes from that database were utilized, and a general research protocol was developed. This produced a uniform algorithmic approach that was agreed upon and approved by 3 operating surgeons—all heads of neurosurgical departments. Prior to the protocol development, none of the 3 centers had a uniform approach, and all 3 centers noted improved outcomes, as one would expect.
Their outcomes were compared with historical controls who had been treated from 2007 to 2014 without any standardized protocol at the Irkutsk (Russia).
To minimize the influence of the surgeon’s experience on the outcome of the operation, surgeons with at least 15 years of experience in surgery were included in the study. In the historical group, the surgeon had 20 years of experience. In the prospective group, there were 3 main surgeons, with 17, 19, and 20 years of experience.
Inclusion Criteria
For the prospective group, we utilized the algorithm for patients following inclusion criteria: symptomatic multilevel cervical spine disease (2 or more intervertebral discs); circumferential compression of the neurovascular structures; C2-C7 lordotic angle >−10°; absence of clinical symptoms and signs of myelopathy; and the presence of MR cord signal change less than 1 segment.
Exclusion Criteria
Isolated ventral compression, asymptomatic multilevel disease; single-level degeneration of the cervical spine; C2-C7 lordotic angle <−10°; clinical manifestations of myelopathy without cord compression on MR; the presence of MR cord signal change greater than 1 segment; traumatic or inflammatory disease of the cervical spine; previous cervical operation; significant osteoporosis; and instability.
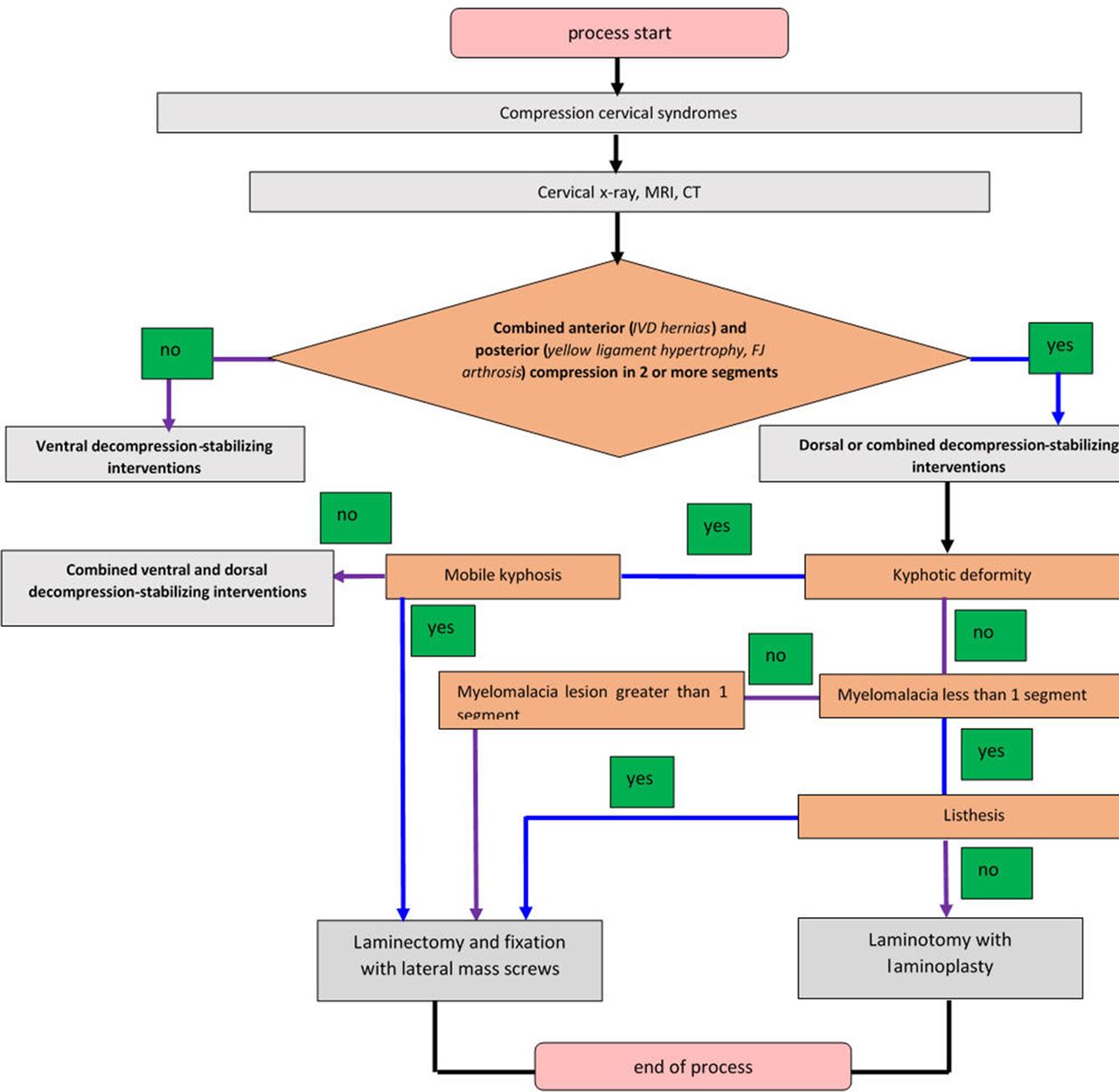
Figure 1 outlines the algorithm that was utilized for the prospective study. LP was limited to those with cord signal change less than 1 segment due to the fact that in our pilot retrospective study, those with more than 1 segment did better with an LF (Figure 2).
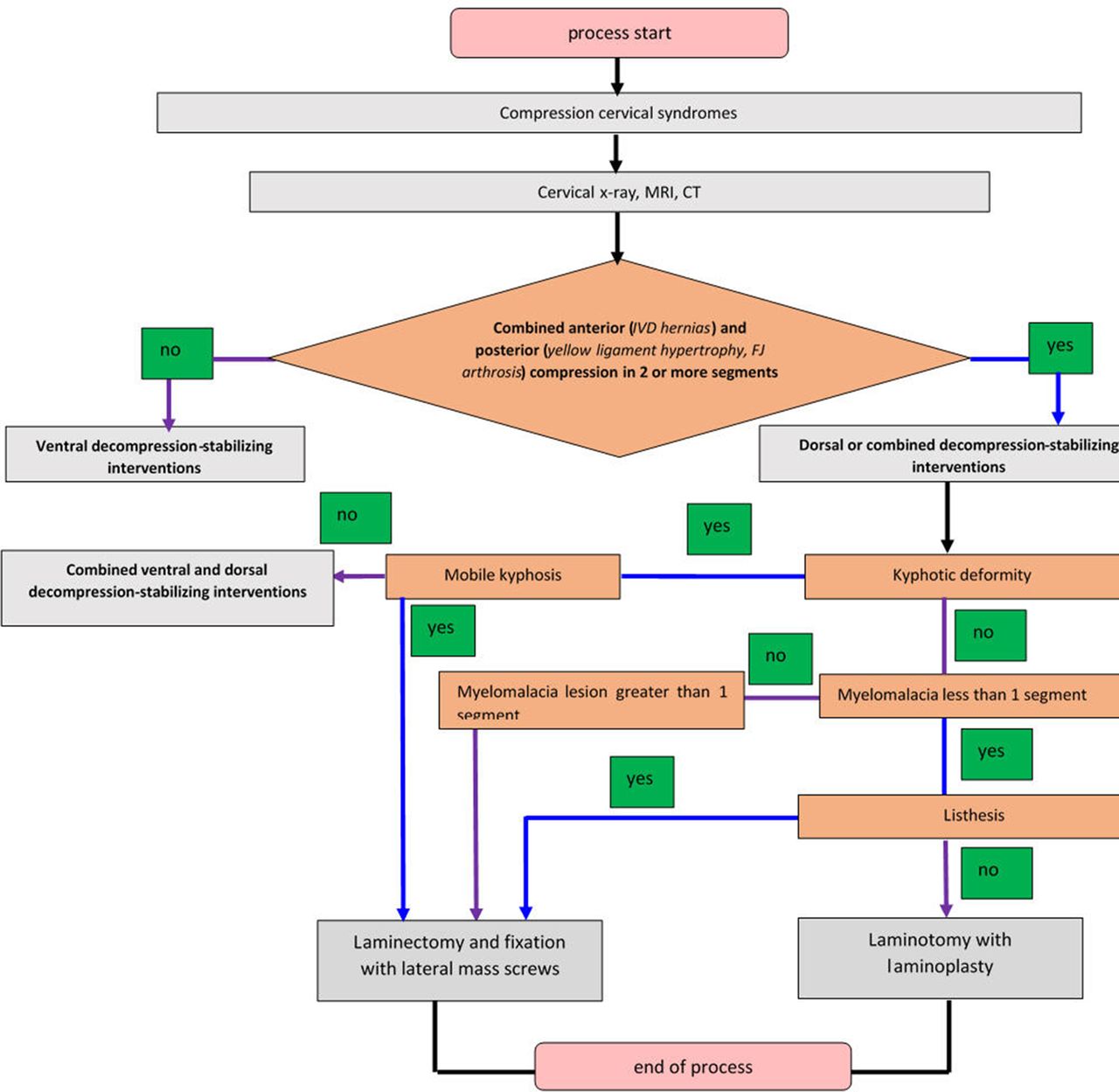
Algorithm for the surgical treatment of patients with multilevel degenerative disease of the cervical spine.9 CT, computed tomography; FJ, facet joints; IVD, intervertebral discs; MRI, magnetic resonance imaging.

Flowchart for study selection. LF, laminectomy with lateral mass fixation; LP, laminoplasty; MRI, magnetic resonance imaging.
Surgical Technique
Surgical interventions were performed under general anesthesia in a prone position with rigid head fixation, using optical magnification, and x-ray control. We used a midline posterior approach to perform an open-door LP10 or LF (Anderson-Sekhon technique).11
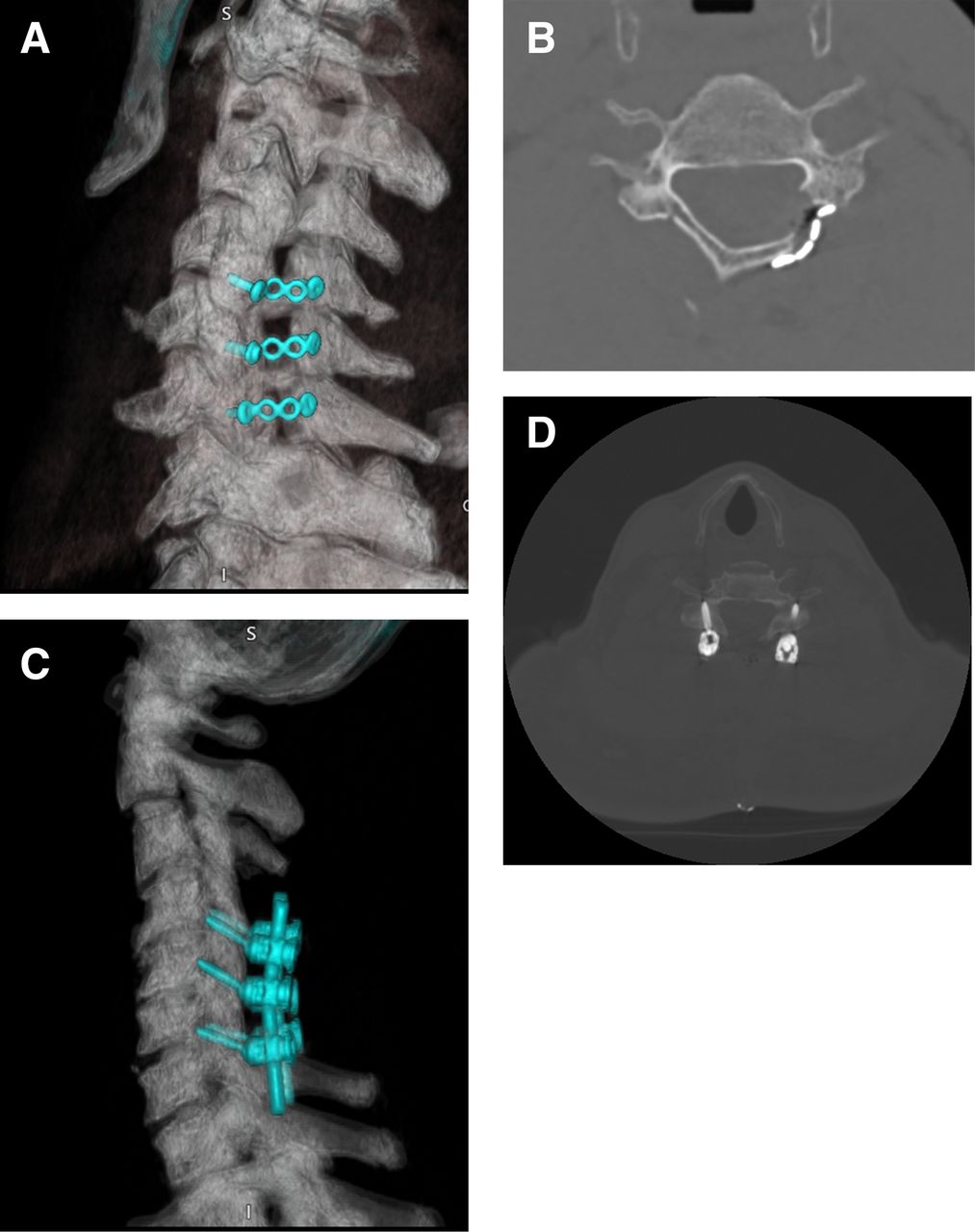
Group I consisted of patients who were treated per the algorithm outlined in Figure 1. Those with the following characteristics were treated with an LP (Figure 3A and B): neutral or lordotic alignment of the cervical spine, preservation of stable segmental motion, absence of clinical signs and symptoms of myelopathy or the absence of MR cord signal change greater than 1 segment. Those with the following characteristics were treated with an LF (Figure 3C and D): kyphosis of the cervical spine, presence of translational instability of the cervical vertebrae, absence of clinical signs and symptoms of myelopathy, or the presence of MR cord signal change at greater than 1 segment.
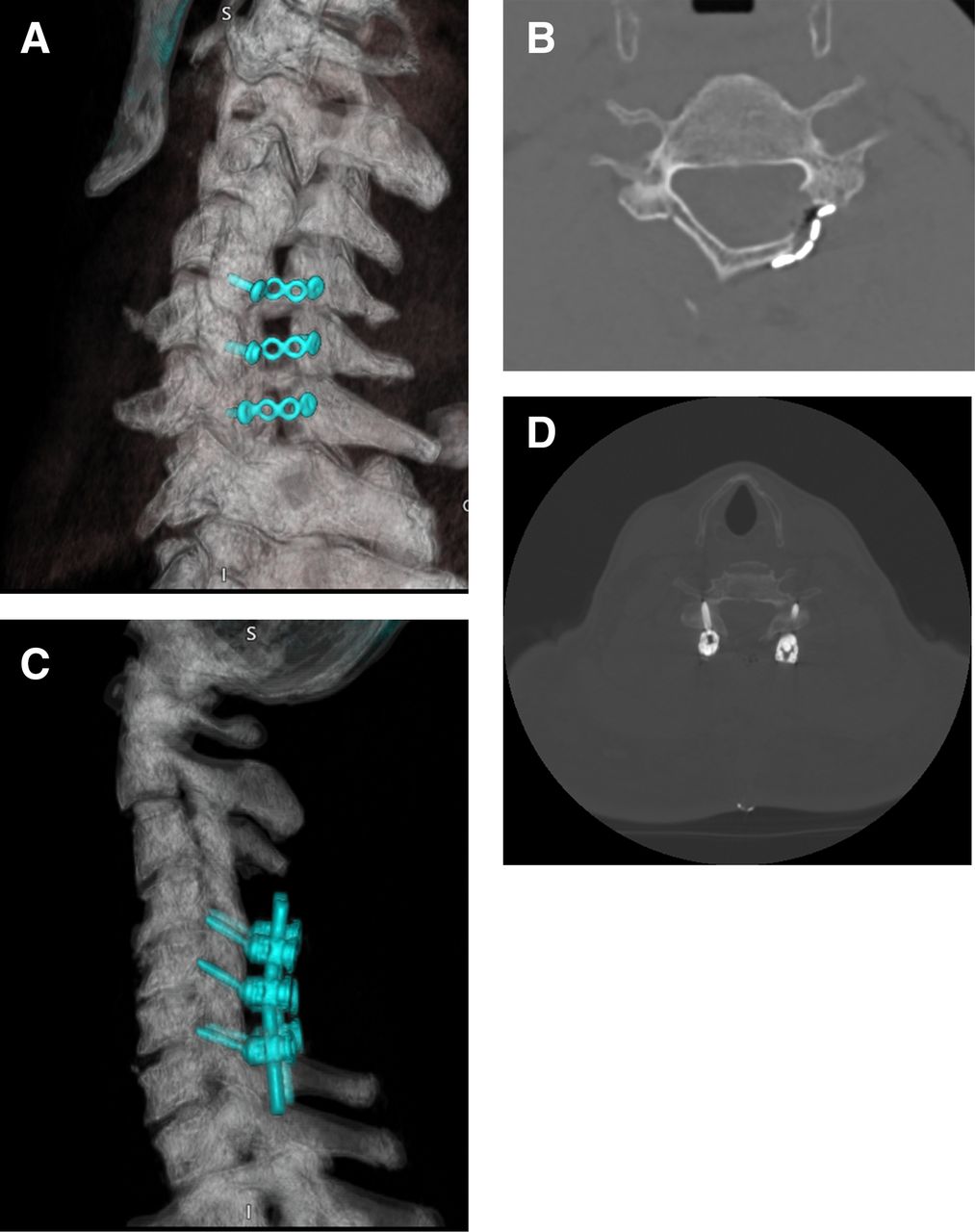
Computed tomography of the cervical spine after open-door laminoplasty was performed from C4 to C6 (A, B); posterior decompression and instrumented fusion were performed from C4 to C6 (C, D).
Group II consisted of patients who had been treated with posterior cervical procedures during 2007 to 2014 without any defined protocol. To be included, they had to have 2-year follow-up.
Outcomes of the Study
All patients in both groups had the following assessments preoperatively and at each postoperative visit: sagittal radiographs of the cervical spine using the Toyama method,12 flexion-extension radiographs, 1.5 T MR imaging, perioperative complications, visual analog scale (VAS) for cervical pain, Neck Disability Index (NDI), and MacNab and Nurick Scales.
Statistical Analysis
Data were entered into Microsoft Excel and Statistica 8.0. The distribution pattern was based on the Shapiro-Wilk, Kolmogorov-Smirnov, and Lil’efors tests. Taking into account the presence of significant differences according to these tests (P < 0.05), the distribution was considered to be different from normal, in connection with which the assessment of the significance of the differences in the sample sets was made according to the criteria of nonparametric statistics; a level of P < 0.05 was considered as the lower confidence limit. The data are presented as the median with the first and third quartiles (Q25; Q75). The following nonparametric statistics criteria were used: the Mann-Whitney test for intergroup comparison, Friedman criterion for dependent samples, and Fisher exact test for binomial parameters.
RESULTS
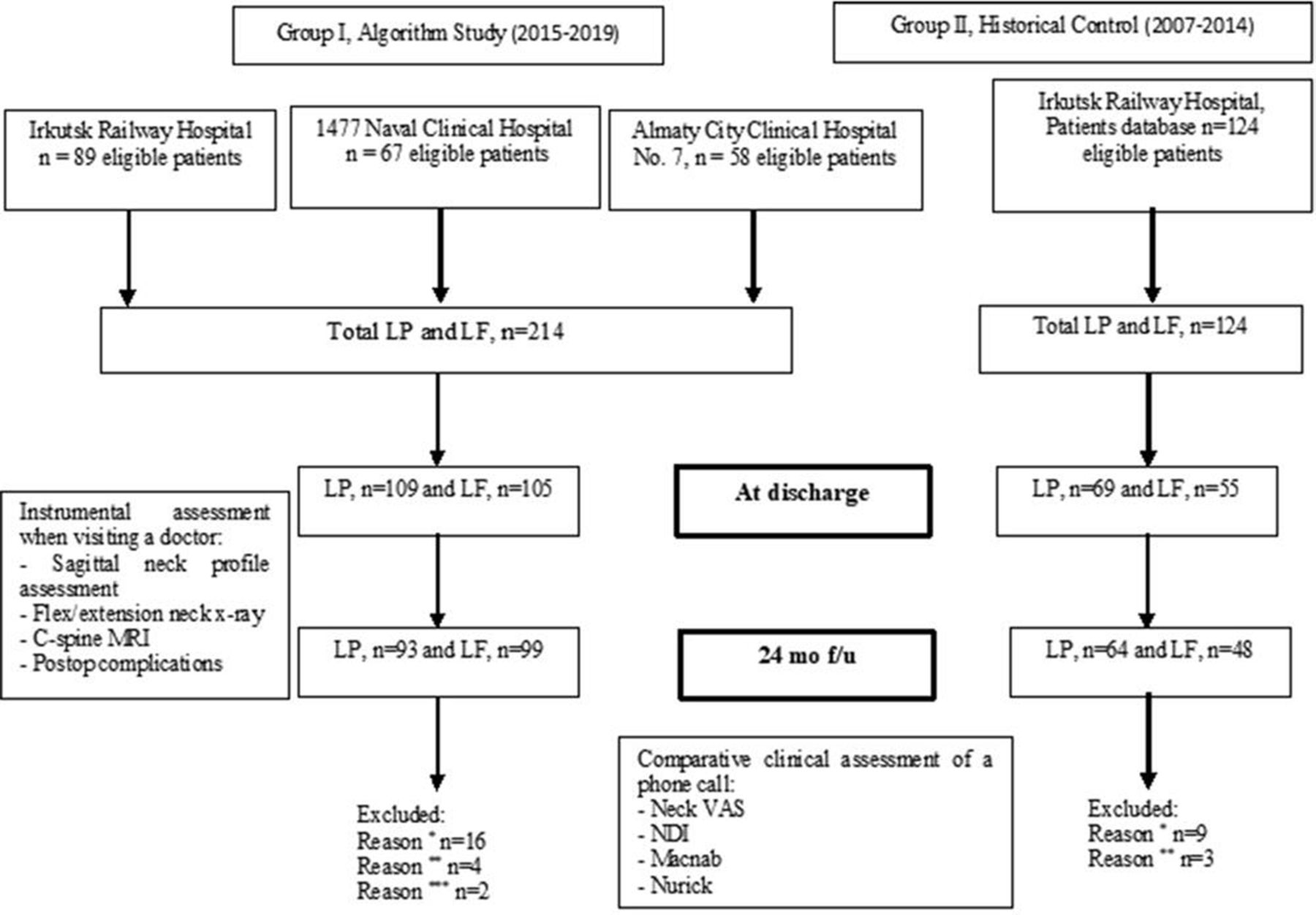
There were a total of 338 patients with degenerative disease of the cervical spine enrolled in the study (Figure 4). Information about the patients included in the study is shown in Table 1. According to the studied characteristics, there were no intergroup differences revealed in gender, age, and number of operated vertebrae (P > 0.05). The average follow-up was 28 months in Group I and 40 months in Group II. In Group I, information was available on 192 out of 214 treated patients (LP, n = 93, and LF, n = 99). In Group II, 112 patients were available for analysis (LP, n = 64, and LF, n = 48).
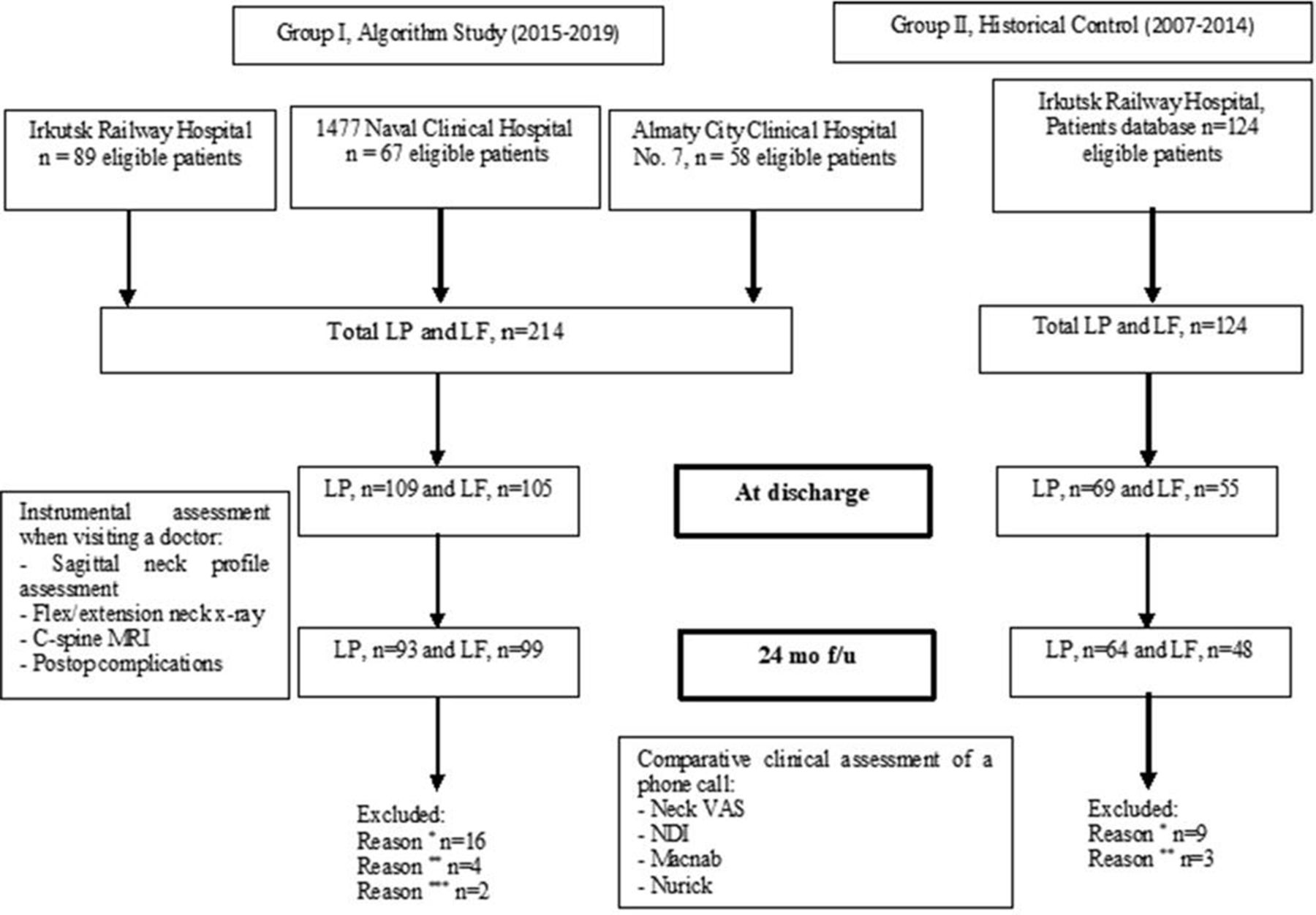
A total of 338 patients underwent surgery for multilevel degenerative cervical spine disease. Out of these, 34 patients were excluded. Reason *, loss of follow-up; Reason **, refusal to participate in the study; Reason ***, death unrelated to the operation (in these cases, there were no postoperative complications). f/u = follow-up; LP, open-door laminoplasty; LF, laminectomy with instrumented fusion; MRI, magnetic resonance imaging; NDI, Neck Disability Index; VAS, visual analog pain scale.
Characterization of patients of the studied groups.
There were 69 LP and 55 LF cases in the retrospective group (55.6% vs 44.4%, respectively) and 109 LP and 105 LF cases in the algorithm group (50.9% vs 49.1%, respectively). Thus, the use of the proposed criteria slightly increased the proportion of patients operated on using LF. At the same time, if we followed the algorithm, we would have done in the retrospective group 58 LP and 66 LF (46.8% vs 53.2%, respectively).
Preoperatively, in both Groups I and II, the majority of patients had radicular pain (95.8% and 97.3%, respectively, P = 0.67), neck pain (89.6% and 88.4%, respectively, P = 0.51), dermatomal loss of sensation (61.5% and 58%, respectively, P = 0.24), and decreased deep tendon reflexes of the upper extremities (67.7% and 64.3%, respectively, P = 0.39).
Preoperatively, there were no statistically significant differences (P > 0.05) between the 2 groups in neck pain and NDI. Postoperatively, there was a significant decrease in the severity of neck pain according to VAS from 81 (75; 86) to 10 mm (9; 12) (P = 0.001) in Group I, and their NDI values improved postoperatively from 47.5 (42; 48) to 12 (8; 14) (P = 0.002). Group II also had a significant improvement in the severity of neck pain from 82 (72; 94) to 22 mm (12; 35) (P = 0.012), and NDI improved from 46 (43; 48) to 18 (13; 27) (P = 0.034). At 2-year follow-up, there was a statistically significant difference in VAS neck pain and NDI scores between Group I and Group II (P < 0.05) (Table 2).
Comparison between Groups I and II for VAS and NDI scores preoperatively and at 2 y postoperatively.
Satisfaction with surgery on the MacNab Scale after 24 months was better in Group I than II (P < 0.001) (Table 3). Outcomes of surgery on the Nurick Scale after 24 months were better in Group I than II (P < 0.0001) (Table 3).
Intergroup comparative analysis of the outcome of surgical treatment on the MacNab and Nurick Scales at long-term postoperative follow-up.
There was a statistically significantly higher complication rate in Group II than Group I (P < 0.0001) (Table 4).
Complications.
DISCUSSION
Multilevel degenerative disease of the cervical spine can be treated either anteriorly or posteriorly, depending on various factors, including the compressive pathology, extent of disease, cervical alignment, and surgeon preference.13,14 Many spine surgeons prefer a posterior approach with an LP or LF for multilevel pathology.15,16 Currently, however, there are few well-done prospective studies that have determined which of these treatment modalities should be utilized for a given condition and which is superior for a given condition.6,17 A poor choice of surgical approach can result in unsatisfactory clinical results due to postoperative pain, deformity, instability, or inadequate decompression.18,19 To help prevent such poor preoperative plans, in 2014, we set out to develop a uniform algorithmic approach to the surgical treatment of multilevel degenerative disease of the cervical spine. We compared the results from this prospectively treated group to historical controls that had been treated at one of the hospitals to determine the impact of the algorithmic approach on surgical outcomes.
Not unsurprisingly, we found that the algorithmic approach, which standardizes surgical treatment, resulted in significant improvement of functional status at long-term follow-up based on VAS pain scores, NDI, MacNab Scale, and Nurick scores, compared with an unstandardized conventional approach based on surgeon whim or preference. Postoperatively, there was a significant decrease in the severity of neck pain from 81 (75; 86) to 10 mm (9; 12) (P = 0.001) in Group I, and their NDI values improved postoperatively from 47.5 (42; 48) to 12 (8; 14) (P = 0.002). There was also a decreased complication rate in Group I—5.7%, compared with Group II—34.8% (P = 0.004), including for neurologic deficits, revision procedures, and postoperative deformity. We think that the algorithm per se does not eliminate the development of surgical complications, but we are confident that different procedures can affect the morbidity.
The results of surgical treatment in our historical control group were comparable with what is in the literature. However, our results using the algorithmic approach appear to be better than the results reported in the literature regarding posterior cervical procedures.20–22 We believe that LP is a less invasive option than LF.
While our results using the algorithm appear to be better than the results of previous studies, it must be cautioned that one cannot directly compare different studies with different methodologies and different patient populations, even if the type of procedure remains constant. Nevertheless, our successful results using an algorithmic approach appear to indicate the promise of using our proposed algorithm for choosing the type of posterior cervical procedure in patients with multilevel degenerative disease of the cervical spine.
Limitations
There are several limitations to this study. First, while it was a multicenter study, only 3 institutions from 2 countries were involved in the study. We believe that it is not likely, but certainly possible, that a more widespread usage of such an algorithmic approach might not yield comparable results. Only a larger study with more centers in different regions can determine the effectiveness of the algorithm. Second, while our follow-up period meets the minimal 2-year follow-up requirement of many journals, 2 years are not long enough to determine the true long-term outcomes. For this reason, we plan to continue to follow these patients. Third, this study does not address the superiority of either LP or LF, since we are simply determining whether an algorithmic approach to choosing one vs the other can result in better outcomes and reduction of complications. Since the 2 groups had, by definition, different preoperative factors, we cannot compare the 2 groups for superiority. Fourth, we did not obtain any computed tomography (CT) images to verify the fusion status for any of the instrumented fusion cases. But CT images expose the patient to substantial radiation, and we believed that it was not necessary to obtain such images in asymptomatic patients. Therefore, we did not feel that the additional information was adequate justification for obtaining routine CT images on hundreds of patients. Fifth, we compared the results of a prospective cohort (3 neurosurgical centers from 2 countries) with a historical control group (1 neurosurgical center from 1 country). The heterogeneity of the 2 groups may have introduced some unknown bias. Sixth, in our algorithm, we chose LF over LP for cases with greater than 1 level of myelomalacia. While we based this choice on our retrospective analysis, there is literature that demonstrates that LP can yield good results, even in cases with more than 1 level of myelomalacia. Seventh, Group II had a longer follow-up period. This may be a reason why there were higher long-term complication rates in Group II, such as development of kyphotic deformity, stabilization failure, adjacent segment disease, and progression of symptoms. Finally, since the operations used for historical controls were performed from 2007 to 2014, prior to when the algorithm-based prospective study was performed (2015–2019), it is possible that the surgeons gained more experience in the interim, contributing to some of the improved outcomes. Only a prospective, randomized study could determine the validity of that argument. However, once an algorithm, based upon scientific evidence and best practices of the surgeons, has been established, it would be difficult, if not impossible and unethical, to not abide by such a standard. In any event, the main goal of our study was to prospectively evaluate the efficacy of our algorithm at obtaining reasonable outcomes and minimizing complications, based on a large number of prospectively enrolled patients from 3 different centers in 2 different countries.
CONCLUSION
We developed and prospectively tested, in a multicenter trial, an algorithm to guide us in the posterior treatment of multilevel degenerative disease of the cervical spine. We found that it resulted in good clinical and radiological outcomes. In comparison with historical controls, there was a decrease in the complication rate along with an improvement in functional outcomes.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethics Approval This study was approved by the Irkutsk State Medical University ethics committee.
Author Contributions (1) Conception and design: Vadim A. Byvaltsev. (2) Data acquisition: Vadim A. Byvaltsev, Andrei A. Kalinin, Marat A. Aliyev, Valerii V. Shepelev, Bobur R. Yusupov, Bakhyt M. Aglakov. (3) Analysis of data: Vadim A. Byvaltsev, Andrei A. Kalinin, Eugenii G. Belykh, Marat A. Aliyev, Valerii V. Shepelev, Mikhail Y. Biryuchkov, Bobur R. Yusupov, Bakhyt M. Aglakov. (4) Drafting of the manuscript: Vadim A. Byvaltsev, Andrei A. Kalinin, Marat A. Aliyev, Valerii V. Shepelev, Mikhail Y. Biryuchkov. (5) Critical revision: Vadim A. Byvaltsev, K. Daniel Riew. (6) Administrative support: Vadim A. Byvaltsev. (7) Supervision: K. Daniel Riew.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.