


Article Figures & Data
Figures
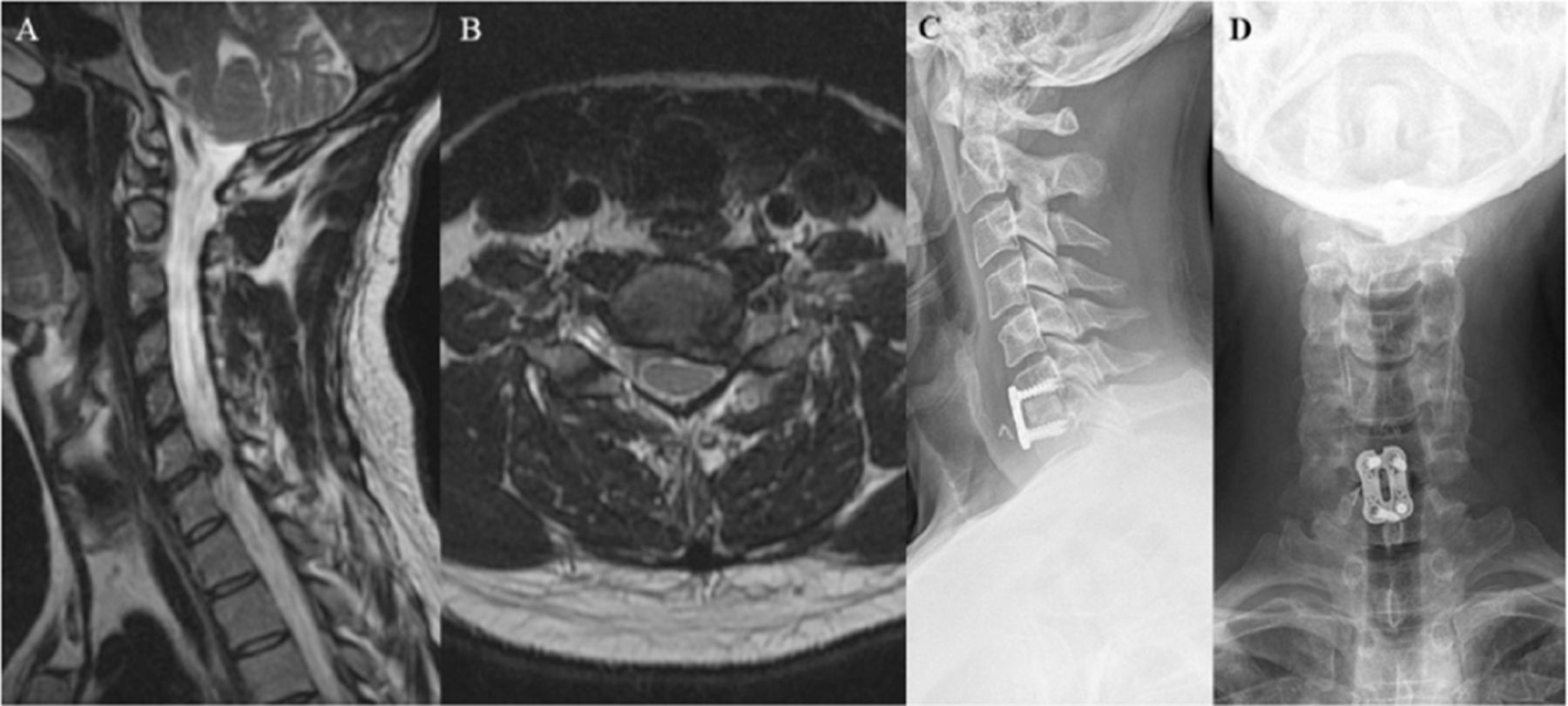
- Figure 1
A 44-year-old man with several months of worsening left C7 radiculopathy despite conservative management was found to have large paramedian C6–C7 disc rupture seen on parasagittal (A) and axial magnetic resonance imaging (B). The patient underwent a right-side anterior cervical discectomy and fusion with structural allograft (C and D) followed by complete resolution of his radicular symptoms 5 weeks after the operation.
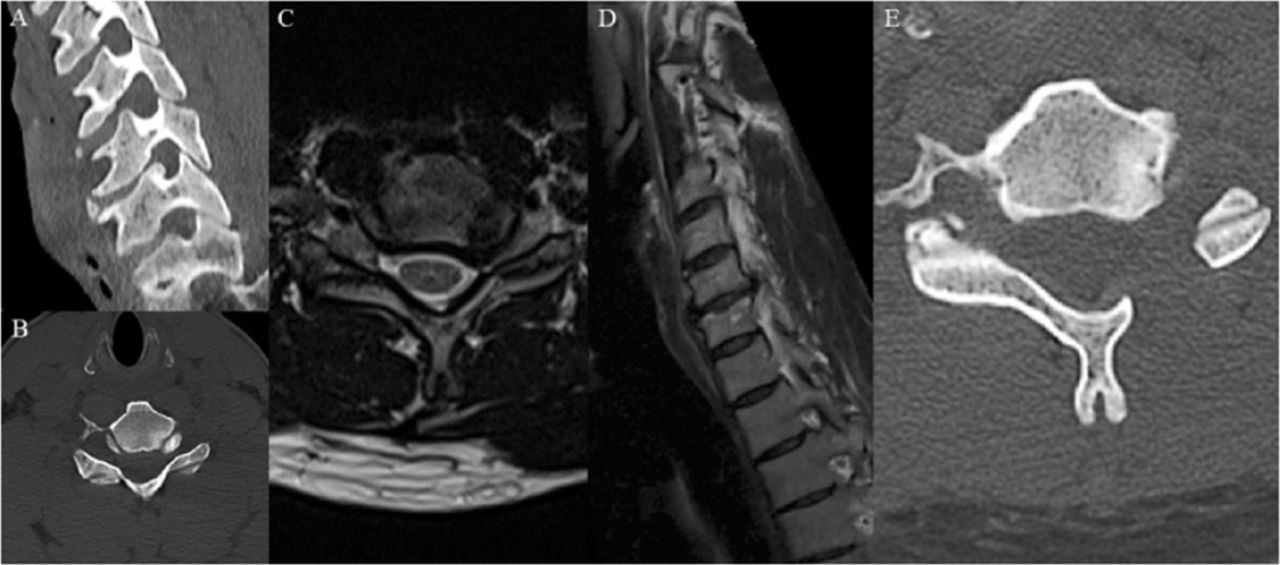
- Figure 2
A 46-year-old man with a history of fibromyalgia and postural orthostatic tachycardia syndrome presented with 10 months of left C7 distribution radiculopathy with left triceps and wrist extension weakness despite conservative management. Preoperative imaging showing bony left C6–C7 foraminal stenosis due to uncovertebral joint hypertrophy on sagittal oblique and axial cervical spine computed tomography (A and B) with concomitant stenosis from a C6–C7 paracentral disc bulge on axial and sagittal oblique magnetic resonance imaging (C and D). The patient underwent full endoscopic left C6–C7 posterior foraminotomy (E) with subsequent improvement in C7 radicular pain and full motor recovery at 90 days postoperatively.
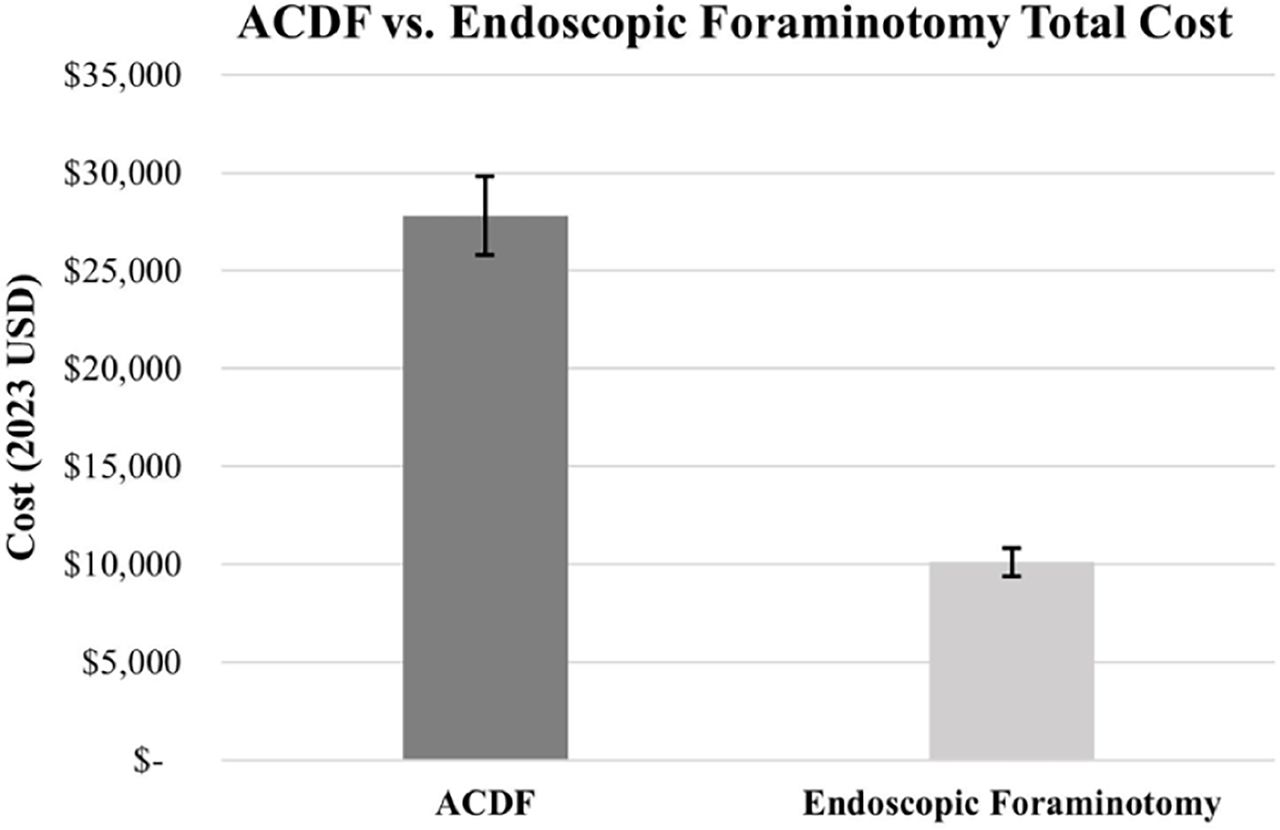
- Figure 3
Total initial anterior cervical discectomy and fusion (ACDF) vs endoscopic foraminotomy cost (mean ± 95% CI total surgical costs for each cohort).
- Figure 4
Sensitivity analysis of anterior cervical discectomy and fusion (ACDF) vs endoscopic foraminotomy shows the potential impact of surgical costs and revision rates on overall cost differences between ACDF and endoscopic cervical foraminotomy ($0 on X-axis). No input variability brought ACDF costs below endoscopic cervical foraminotomy costs. Median surgical costs were used as base values with variation between the highest (gray) and lowest (black) studied costs in each variable. Revision rate base values was the percentage of each cohort undergoing revision surgery with variation tested at ±10 absolute percentage points. For sensitivity analysis, all surgical failures were eventually assumed to undergo ACDF revision. Modeled incremental cost after including revision rates was higher for ACDF (+$16,743 [$28,557 ACDF vs $11,814 endoscopic foraminotomy/discectomy]).
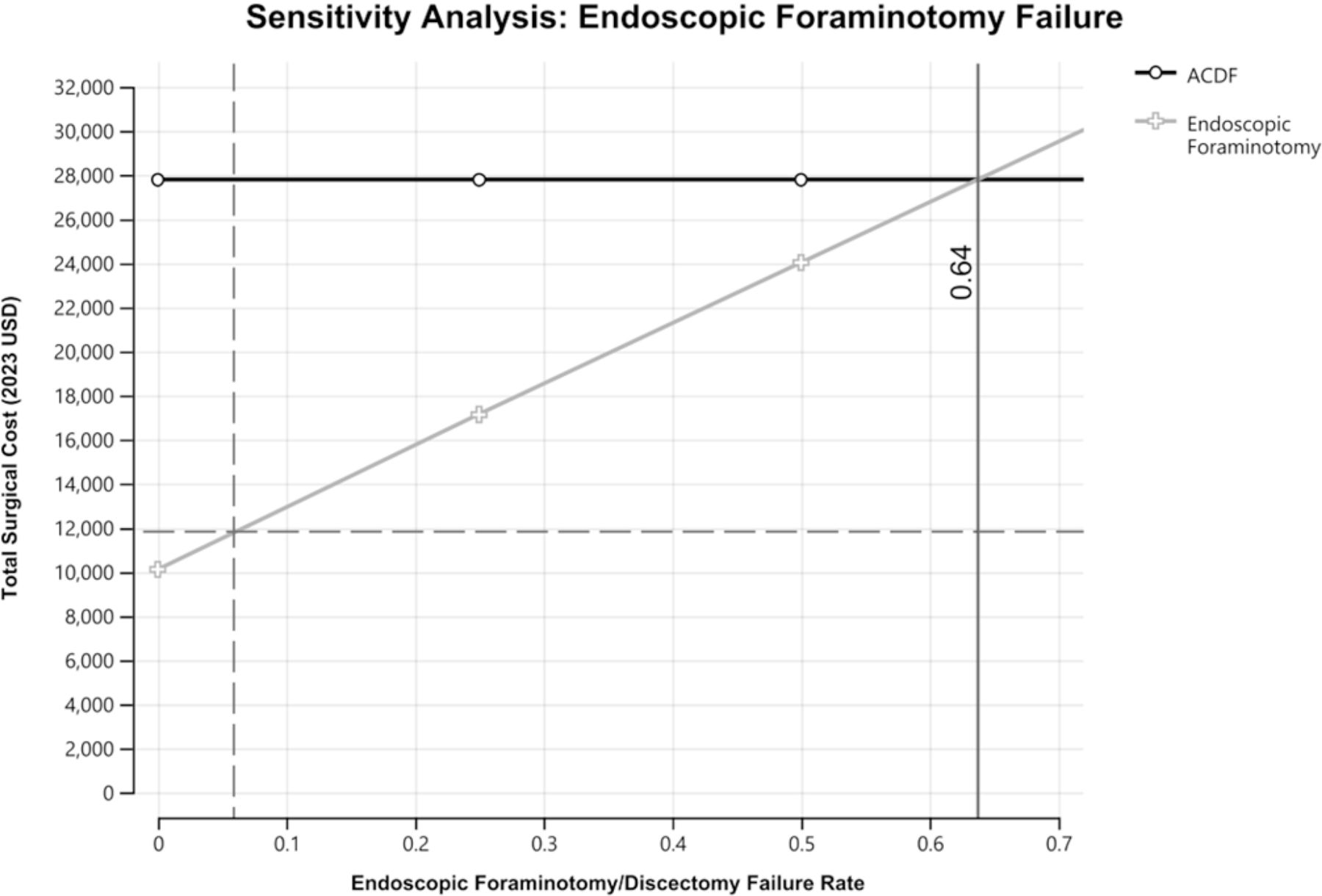
- Figure 5
Break-even analysis. Univariate sensitivity analysis testing endoscopic cervical foraminotomy failure rates (x axis) against the total cost of surgical care (y axis, including revisions), showed that break-even costs between initial ACDF and endoscopic foraminotomy occurred at a 64% endoscopic foraminotomy failure rate (solid gray line, x axis). Analysis assumes no ACDF failures and that every endoscopic foraminotomy failure was ultimately treated with an ACDF. Dashed gray lines show the currently observed endoscopic foraminotomy failure rate (x axis, 5.9%) and the corresponding modeled weighted-average total endoscopic foraminotomy cost including revisions with ACDF after failure ($11,814).





Tables
Demographics and Preoperative Variables ACDF (N = 38) Endoscopic Foraminotomy (N = 17) P Age, mean ± SD 46.8 ± 9.4 57.6 ± 10.3 0.002 Sex, woman, n (%) 20 (52.6%) 3 (17.6%) 0.076 Race, white, n (%) 31 (81.6%) 12 (70.6%) 0.482 BMI, mean ± SD 29.7 ± 5.9 29.6 ± 5.4 0.951 Calcification, n (%) 10 (26.3%) 3 (17.6%) 0.517 Diabetes 2 (5.3%) 1 (5.9%) >0.999 Coronary artery disease 1 (2.6%) 1 (5.9%) 0.527 Hypertension 15 (39.5%) 11 (64.7%) 0.143 Congestive heart failure 1 (2.6%) 0 >0.999 COPD 1 (2.6%) 0 >0.999 Osteoporosis 0 0 - Smoker 7 (18.4%) 2 (11.8%) 0.043 Insurance, n (%) 0.206 Private 30 (78.9%) 13 (76.5%) Public 4 (10.5%) 4 (23.5%) Uninsured 4 (10.5%) 0 Abbreviations: ACDF, anterior cervical discectomy and fusion; BMI, body mass index; COPD, chronic obstructive pulmonary disease.
Note: Mean ± SD or 95% confidence interval tested with 2-tailed t test; n (%) differences tested with Fisher’s exact test. Boldface indicates statistically significant findings.
Outcomes ACDF (N = 38) Endoscopic Foraminotomy (N = 17) P Perioperative Duration of symptoms, mo, mean ± SD 6.3 ± 5.2 19.1 ± 33.3 0.737 Disc location, n (%) 0.248 Central 2 (5.3%) 1 (5.9%) Paramedian 11 (28.9%) 2 (11.8%) Lateral 20 (52.6%)* 14 (82.4%) Disc bulging/herniation, n (%) 38 (100.0%) 17 (100.0%) - Operative time, min, mean ± SD 167.7 ± 22.0 142.7 ± 27.4 <0.001 Estimated blood loss, mL, mean ± SD 32.2 ± 47.6 9.9 ± 11.6 <0.001 Outpatient, n (%) 0 16 (94.1%) <0.001 Discharge home, n (%) 38 (100.0%) 17 (100%) - Length of stay, d, mean ± SD (range) 1.1 ± 0.51–4 0.1 ± 0.2 (0–1) <0.001 Postoperative Neurological/pain improvement at 6 wk, n (%) 38 (100.0%) 17 (100.0%) - Postoperative opioid use, n (%) 30 (78.9%) 0 <0.001 Follow-up, mo, mean ± SD 11.5 ± 10.7 7.1 ± 7.4 0.247 Readmission, n (%) 0 1 (5.9%) 0.309 Reoperation, n (%) 1 (2.6%) 1 (5.9%) 0.527 Complications, n (%) 3 (7.9%) 0 0.544 Total initial surgical cost, mean ± 95% CI $27,782 ± $2011 $10,103 ± $720 <0.001 Note: Mean ± SD or 95% confidence interval tested with 2-tailed t test; n (%) differences tested with Fisher’s exact test. Boldface indicates statistically significant findings.
Independent Variables Univariate Analysis (P) Multivariable Cost Analysis ACDF Foraminotomy All β (±95% CI) P Preoperative variables BMI 0.243 0.801 0.549 - - Age 0.091 0.006 <0.001 - - Race (white) 0.505 0.072 0.211 - Gender 0.675 0.559 0.049 - - Insurance (private) 0.529 0.026 0.297 - - Operative variables LOS (nights) 0.604 - <0.001 - - Operative minutes 0.427 0.122 <0.001 - - Surgical procedure ACDF - - <0.001 $17,723 ± $3065 <0.001 Endoscopic (reference) - - - $10,103 ± $2537 <0.001 Abbreviations: ACDF, anterior cervical discectomy and fusion; BMI, body mass index; LOS, length of stay.
Note: Univariate analysis performed with 2-tailed t test for binary independent variables and simple linear regression for independent continuous variables with a cutoff at alpha = 0.2. Multivariable stepwise regression including any significant univariate variables was performed with a significance cutoff at alpha < 0.05. Boldface indicates statistically significant findings.
Outcome Measure ACDF Endoscopic Complications n = 3 n = 0 Description Mild dysphagia causing coughing and choking, though regular diet was still advised, lasting for 3 mo
Superficial infection treated with oral antibiotics
Postoperative pneumonia requiring oral antibiotics
Reoperations n = 1 n = 1 Description Right C6 radiculopathy after C5–C6 ACDF—lead to removal of instrumentation at C5–C6 and redo ACDF C5–C7 Right C4–C5 soft disc herniation leading to C5 radiculopathy and weakness in the deltoid/biceps (2/5–3/5)—lead to C4–C5 cervical disc arthroplasty Abbreviation: ACDF, anterior cervical discectomy and fusion.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.