


Article Figures & Data
Figures
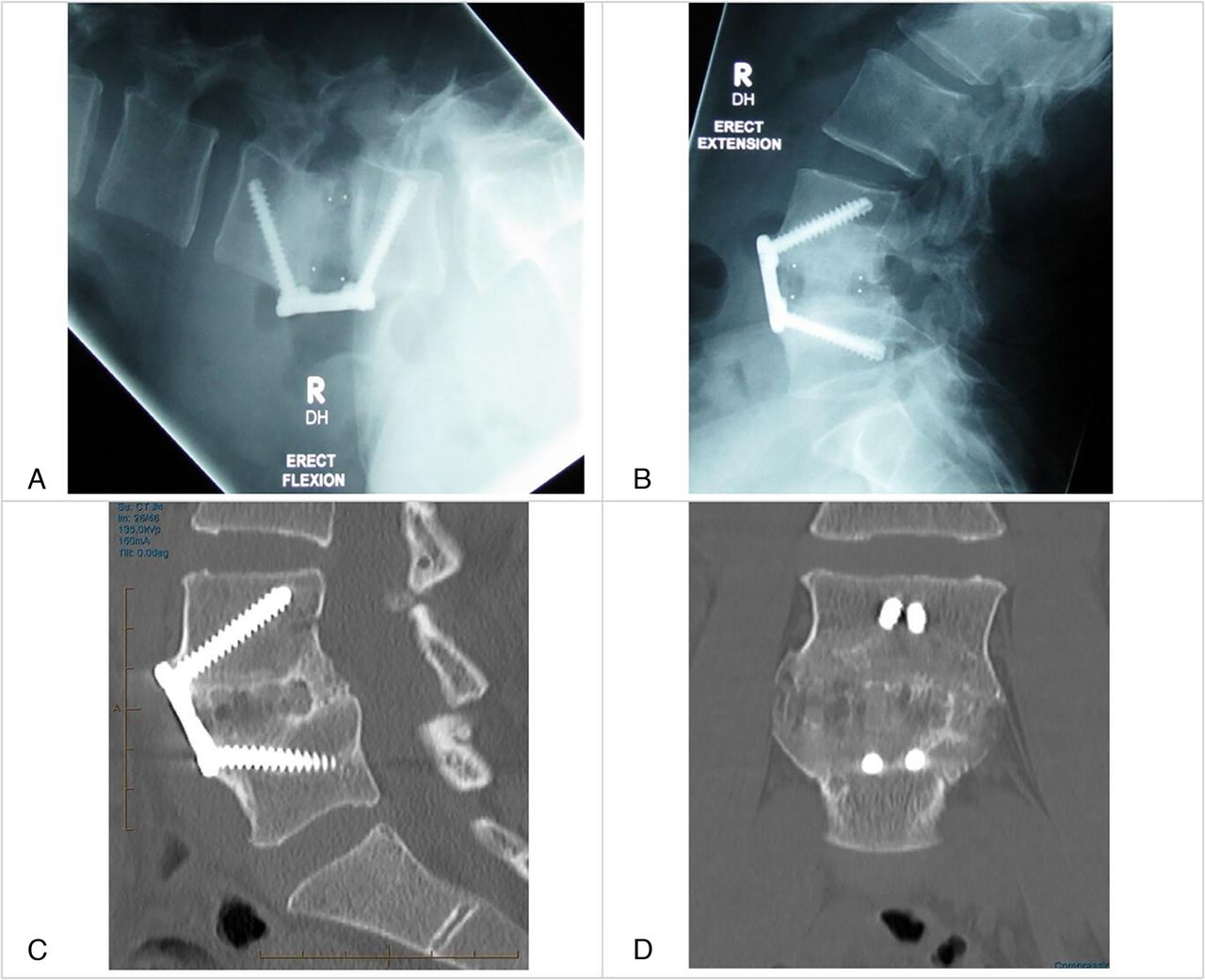
- Figure 1
Dynamic x-ray images showing stability across the anterior lumbar interbody fusion construct in flexion (A) and extension (B). Fine-cut computed tomography images showing confluent bridging bone assessed on sagittal (C) and coronal (D) sequences.
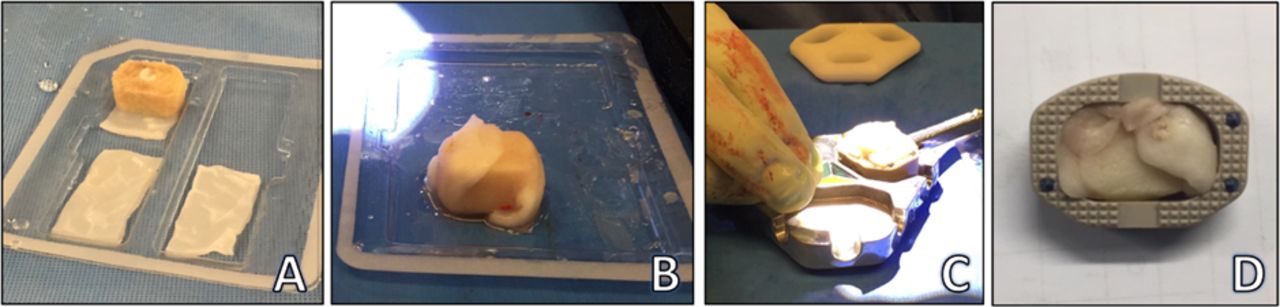
- Figure 2
Preparation of anterior lumbar interbody fusion surgical constructs. (A) Hole drilled through femoral head allograft and recombinant human bone morphogenetic protein-2 (rhBMP-2) sponge packed inside. (B) The allograft wrapped in rhBMP-2 sponge. (C) Construct press-fitted inside the polyetheretherketone cage. (D) Cage, allograft, and rhBMP-2.
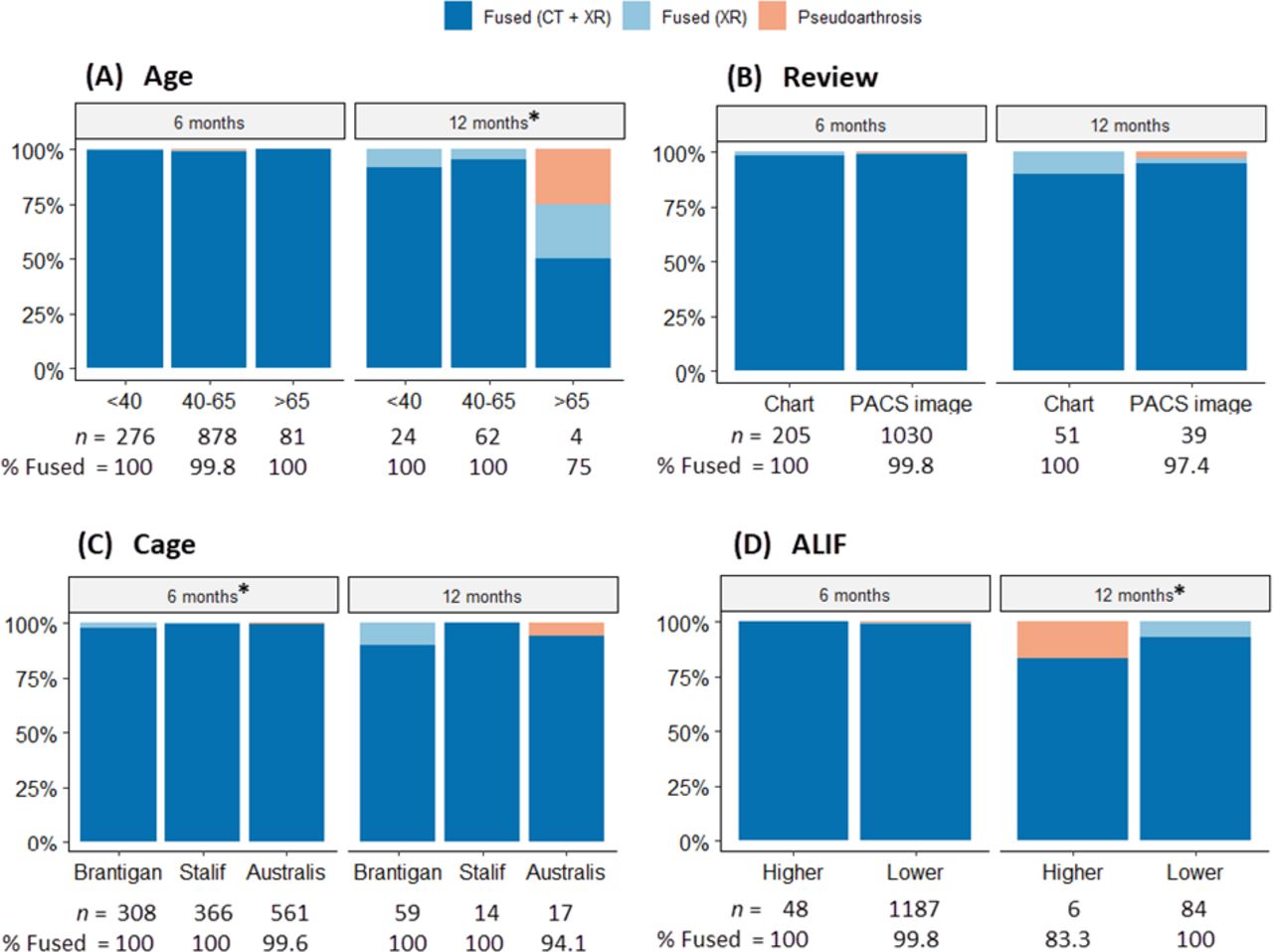
- Figure 3
Fusion rates at 6 and 12 months by age, review, cage, and anterior lumbar interbody fusion (ALIF) groups. (A) *Lower fusion rate of (n = 1 of 4) 75% at 12 months for the >65 groups compared with other groups: <40 (P < 0.001) and 40–65 (P = 0.014). (B) No significant difference was detected between reviews. (C) *Higher fusion rates (CT + XR) were obtained with STALIF (99.7%) and Australis (99.6%) cages at 6 months than with Brantigan (97.7%). There is no significant difference in overall fusion rates between cage types. (D) *At 12 months, all patients in the Lower ALIF group achieved fusion compared with (n = 1 of 6) 83.3% in the higher group (P < 0.001). CT, computed tomography; PACS, picture archiving and communication system; XR, x-ray imaging.
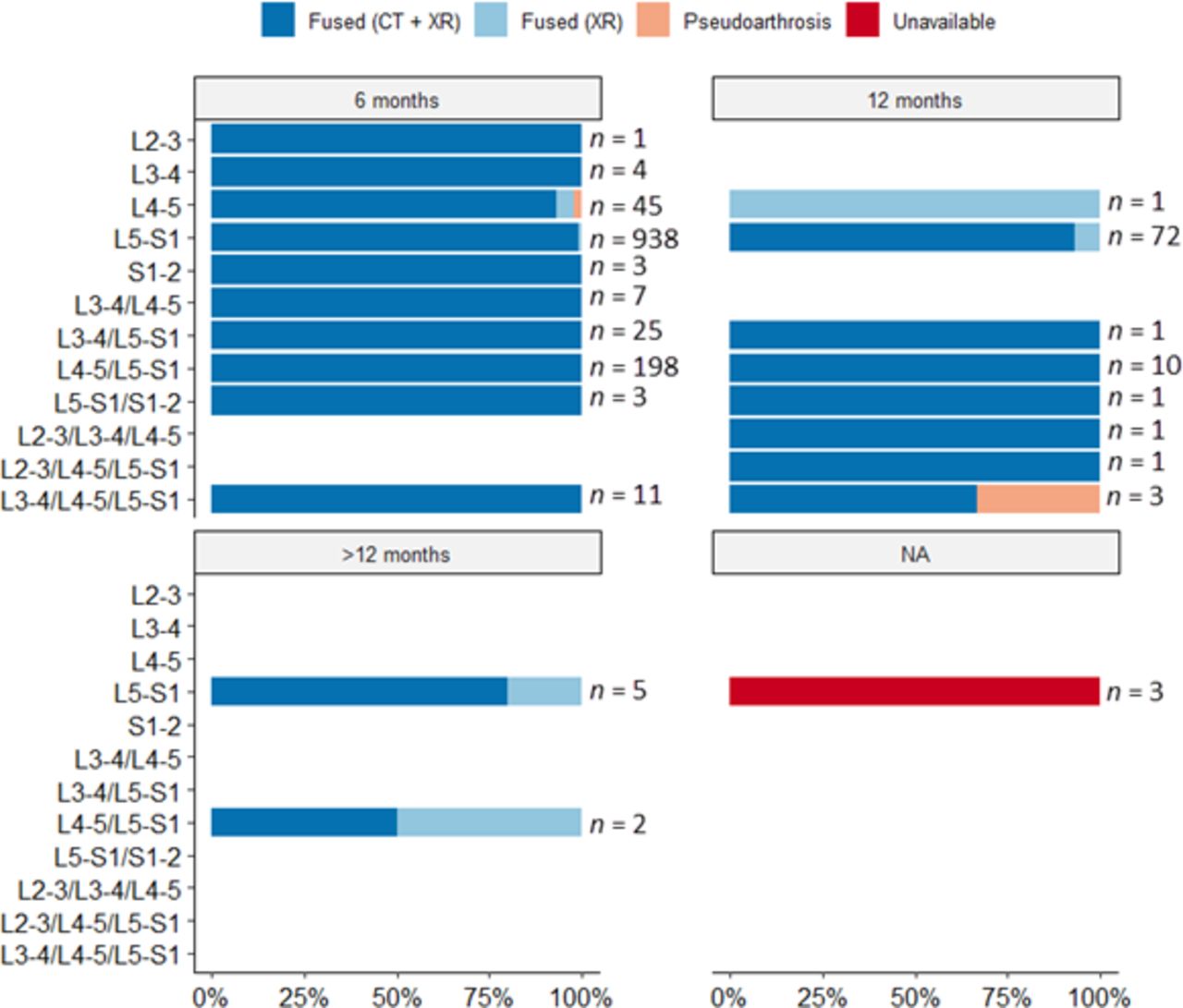
- Figure 4
Fusion rates in spine surgery patients (n = 1335) were higher than 95% in all available cases, except for the L3–L4/L4–L5/L5–S1 anterior lumbar interbody fusion (ALIF) combination at 12 months, where two-thirds of the group achieved fusion (n = 1 of 3, 66.7%). However, it is noteworthy that all 11 cases with the same combination achieved fusion at 6 months. There were 2 cases of pseudoarthrosis at single levels (L4–L5 and L5–S1) at 6 months (the latter is hard to detect on the graph due to the high percentage of patients achieving fusion). The third case occurred at 12 months in a 3-level ALIF.
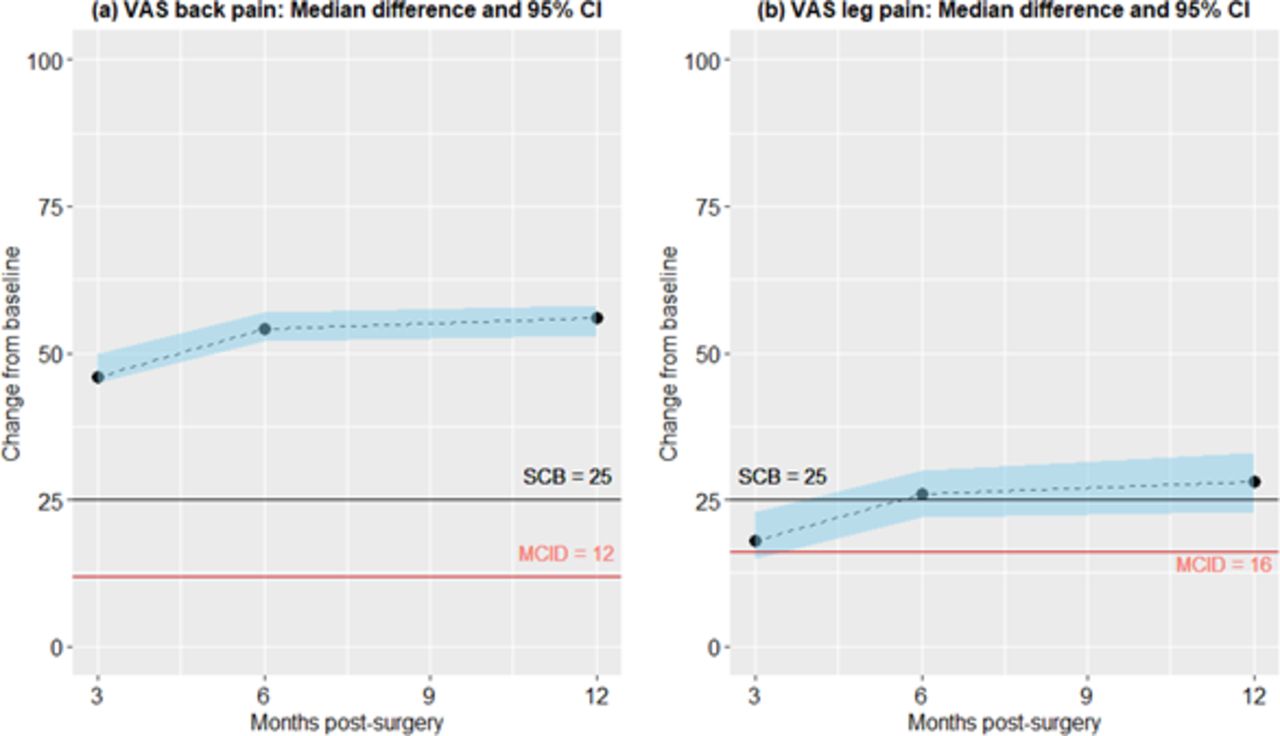
- Figure 5
Median differences from baseline and 95% confidence interval for visual analog scale (VAS) back and leg pain scores over 12 months after surgery. All median change scores were above the minimal clinically important difference (MCID), and most median scores were above the substantial clinical benefit (SCB).
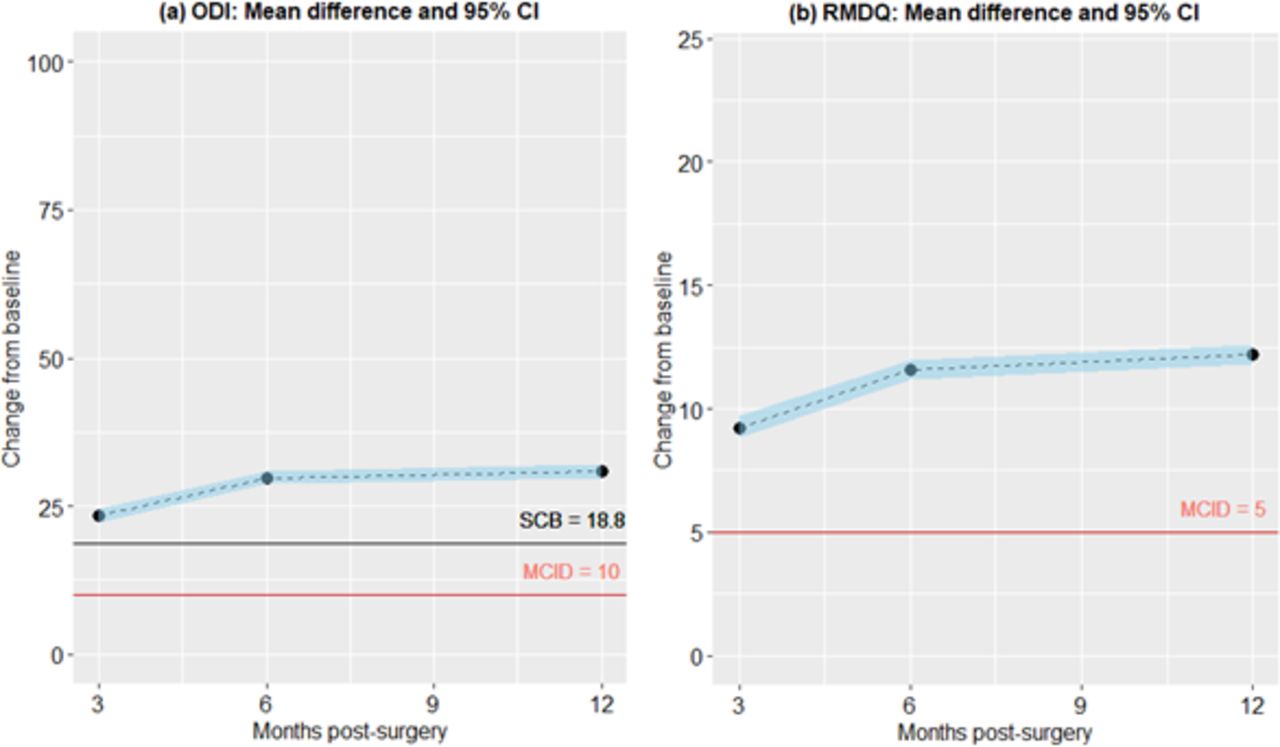
- Figure 6
Mean differences from baseline and 95% confidence interval for Oswestry Disability Index (ODI) and Roland-Morris Disability Questionnaire (RMDQ) disability scores over 12 months after surgery. All mean change scores were above the minimal clinically important difference (MCID) for both measures and above the substantial clinical benefit (SCB) for ODI. No SCB reference was available for RMDQ.
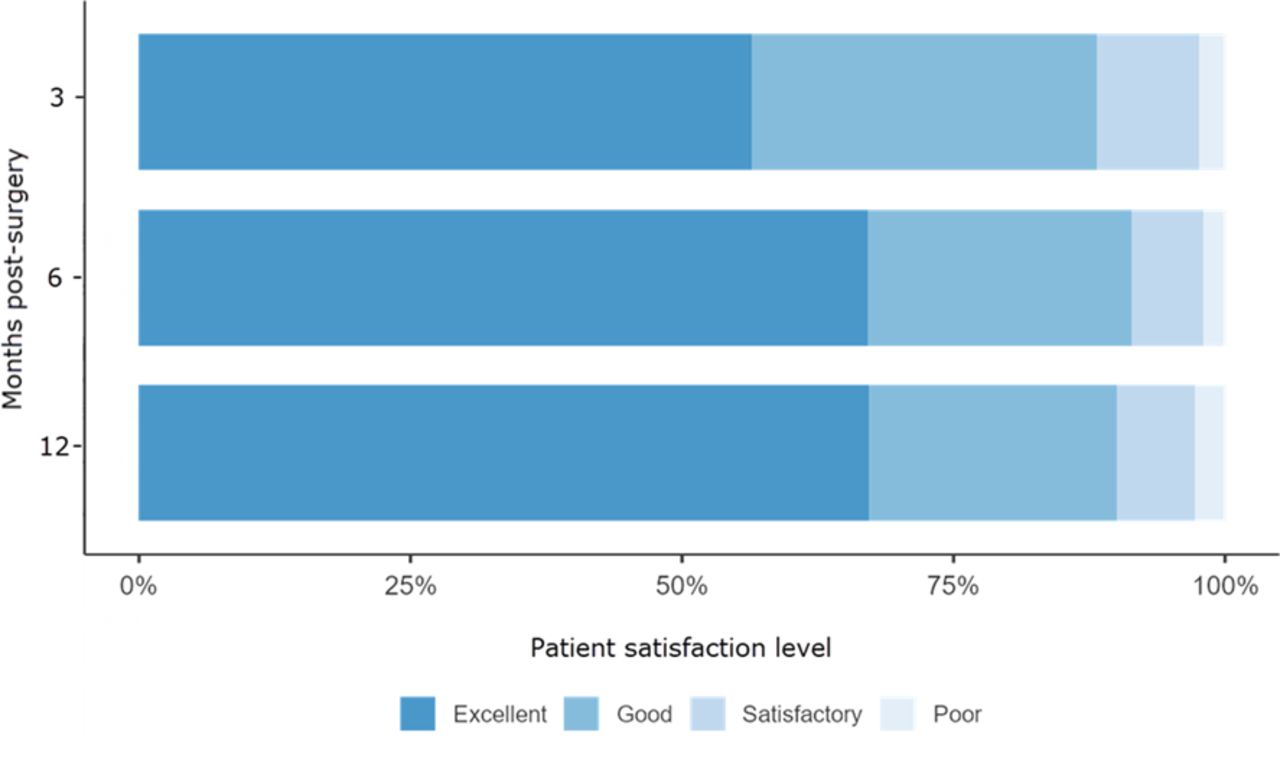
- Figure 7
Patient satisfaction levels within 12 months after surgery rated as poor (1), satisfactory (2), good (3), or excellent (4).







Tables
Characteristic n (%) Age at time of surgery, y, mean (SD) 48.5 (11.4) Age group <40 y 303 (22.7) 40–65 y 946 (70.9) >65 y 86 (6.4) Review type Chart (2005–2008) 263 (19.7) PACS image (2009–2019) 1072 (80.3) Cage type Brantigan (2005–2009) 374 (28.0) STALIF (2010–2013) 381 (28.5) Australis (2014–2019) 580 (43.4) ALIF level 1614 (100.0) L2–L3 3 (0.2) L3–L4 52 (3.9) L4–L5 279 (20.9) L5–S1 1273 (95.4) S1–S2 7 (0.5) ALIF group Higher (cases with L2–L3 and L3–L4) 54 (4.0) Lower (cases with L4–L5 and lower) 1281 (96.0) Single level 1072 (80.3) L2–L3 1 (0.1) L3–L4 4 (0.3) L4–L5 46 (3.4) L5–S1 1018 (76.3) S1–S2 3 (0.2) 2-Level 247 (18.5) L3–L4/L4–L5 7 (0.5) L3–L4/L5–S1 26 (1.9) L4–L5/L5–S1 210 (15.7) L5–S1/S1–S2 4 (0.3) 3-Level 16 (1.2) L2–L3/L3–L4/L4–L5 1 (0.1) L2–L3/L4–L5/L5–S1 1 (0.1) L3–L4/L4–L5/L5–S1 14 (1.0) Abbreviations: ALIF, anterior lumbar interbody fusion; PACS, picture archiving and communication system.
Note: Data presented as n (%) unless otherwise noted.
Fusion Overall
(n = 1335)Months After Surgery 6
(n = 1235)12
(n = 90)>12
(n = 7)NA
(n = 3)Fused (CT + XR) 1313 (98.4) 1225 (91.8) 83 (6.2) 5 (0.4) - Fused (XR) 16 (1.2) 8 (0.6) 6 (0.4) 2 (0.1) - Pseudoarthrosis 3 (0.2) 2 (0.1) 1 (0.1) - - Unavailable 3 (0.2) - - - 3 (0.2) Abbreviations: CT, computed tomography; NA, not applicable; XR, x-ray imaging.
Note: Data are presented as n (%). Percentages for cells under “months after surgery” are calculated from the total sample size.
Months Postsurgery VAS Outcome Change From Baseline n Median IQR n Median Differencea 95% CI P b Back Pain 0 (baseline) 1058 72.0 56.3–83.0 3 1274 17.0 5.3–38.0 1019 46.0 45.0–50.0 <0.001 6 1227 11.0 3.0–26.0 975 54.0 52.0–57.0 <0.001 12 1120 9.0 2.0–23.0 915 56.0 53.0–58.0 <0.001 Leg Pain 0 (baseline) 1049 43.0 9.0–72.0 3 1274 9.0 0.0–30.0 1010 18.0 15.0–23.0 <0.001 6 1225 2.0 0.0–15.0 965 26.0 22.0–30.0 <0.001 12 1116 2.0 0.0–13.0 900 28.0 23.0–33.0 <0.001 Months Postsurgery Disability Outcome Change From Baseline n Median IQR n Mean
Differencea95% CI P b ODI 0 (baseline) 1058 42.0 32.0–53.0 3 1262 18.0 8.0–29.8 1011 23.4 22.2–24.5 <0.001 6 1222 10.0 2.0–20.0 972 29.8 28.8–30.9 <0.001 12 1115 8.0 0.0–20.0 910 30.9 29.8–32.1 <0.001 RMDQ 0 (baseline) 1059 16.0 12.0–19.0 3 1266 5.0 2.0–9.0 1012 9.2 8.8–9.7 <0.001 6 1221 2.0 0.0–5.0 970 11.6 11.2–12.0 <0.001 12 1115 1.0 0.0–4.0 908 12.2 11.8–12.6 <0.001 Abbreviations: IQR, interquartile range; ODI, Oswestry Disability Index (0 = no disability to 100 = worst disability); RMDQ, Roland-Morris Disability Questionnaire (0 = no disability to 24 = worst disability).
↵a A positive mean difference indicates an improvement or reduction in disability score.
↵b All differences from baseline were statistically significant.
- Table 5
Results of the between-groups post-hoc comparisons of the change in pain outcomes after controlling for baseline scores in a multivariable mixed-effects regression model.
Comparison Estimated Differencea 95% CI P Lower Upper Change in VAS back painb 3 mo 6 mo 5.30 3.92 6.68 <0.001c 6 mo 12 mo 1.47 0.04 2.90 0.13 3 mo 12 mo 6.77 5.36 8.18 <0.001c <40 y 40–65 y 2.37 −0.30 5.04 0.25 40–65 y >65 y 1.45 −3.02 5.92 >0.99 <40 y >65 y 0.92 −3.97 5.80 >0.99 Brantigan STALIF 2.51 −0.19 5.20 0.21 STALIF Australis 3.01 0.25 5.77 0.10 Brantigan Australis 5.51 2.84 8.19 <0.001c Higher ALIF Lower ALIF 7.49 1.83 13.14 0.010c Change in VAS leg paina 3 mo 6 mo 7.86 6.31 9.41 <0.001c 6 mo 12 mo 0.64 −0.97 2.25 >0.99 3 mo 12 mo 8.50 6.91 10.09 <0.001c <40 y 40–65 y 4.36 1.92 6.80 0.001c 40–65 y >65 y 6.60 2.33 10.87 0.007c <40 y >65 y 10.96 6.34 15.58 <0.001c Brantigan STALIF 2.26 −0.27 4.79 0.24 STALIF Australis 1.89 −0.66 4.44 0.44 Brantigan Australis 4.15 1.63 6.68 0.004c Higher ALIF Lower ALIF 0.49 −4.72 5.70 0.85 Abbreviations: ALIF, anterior lumbar interbody fusion; VAS, visual analog scale.
↵a The estimated difference is the more significant improvement experienced by the category in bold text for each pairwise comparison. None of the estimated differences between groups were clinically significant.
↵b The estimated mean improvement at 3 months postsurgery for a <40-year-old patient with mean baseline, Brantigan cage, and higher ALIF were 44.7 for back pain and 26.6 for leg pain.
↵c Statistically significant difference P < 0.05.
- Table 6
Results of the between-groups post-hoc comparisons of the change in disability outcomes after controlling for baseline scores in a multivariable mixed-effects regression model.
Comparison Estimated Differencea 95% CI P Lower Upper Change in ODIb 3 mo 6 mo 6.46 5.72 7.21 <0.001c 6 mo 12 mo 0.90 0.12 1.67 0.07 3 mo 12 mo 7.36 6.60 8.12 <0.001c <40 y 40–65 y 2.88 1.12 4.63 0.004c 40–65 y >65 y 0.37 −2.55 3.29 >0.99 <40 y >65 y 3.25 0.05 6.44 0.14 Brantigan STALIF 0.11 −1.67 1.88 >0.99 STALIF Australis 1.86 0.04 3.68 0.14 Brantigan Australis 1.97 0.22 3.72 0.08 Higher ALIF Lower ALIF 5.74 2.01 9.46 0.003c Change in RMDQa 3 mo 6 mo 2.37 2.10 2.64 <0.001c 6 mo 12 mo 0.49 0.21 0.77 0.002c 3 mo 12 mo 2.86 2.58 3.14 <0.001c <40 y 40–65 y 0.80 0.19 1.42 0.030c 40–65 y >65 y 0.42 −0.60 1.44 >0.99 <40 y >65 y 1.22 0.11 2.34 0.10 Brantigan STALIF 0.15 −0.47 0.77 >0.99 STALIF Australis 0.93 0.29 1.56 0.013c Brantigan Australis 1.08 0.47 1.69 0.002c Higher ALIF Lower ALIF 2.61 1.32 3.91 <0.001c Abbreviations: ALIF, anterior lumbar interbody fusion; ODI, Oswestry Disability Index; RMDQ, Roland-Morris Disability Questionnaire.
↵a The estimated difference is the more significant improvement experienced by the category in bold text for each pairwise comparison. None of the estimated differences between groups were clinically significant.
↵b The estimated mean improvement at 3 months postsurgery for a <40-year-old patient with mean baseline, Brantigan cage, and higher ALIF were 25.5 for ODI and 9.8 for RMDQ.
↵c Statistically significant difference P < 0.05.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.