


Abstract
Background Various strategies have been used to reduce pedicle screw loosening following lumbar instrumented fusion, but all strategies have limitations. In this prospective multicenter cohort study, outcomes of elderly patients with reduced bone density who underwent primary or revision fusion surgery using a novel technique of pedicle screw augmentation with demineralized bone fiber (DBF) anchors were evaluated.
Methods This study included elderly patients (aged >65 years) with dual-energy x-ray absorptiometry-confirmed reduced bone density who required lumbar pedicle screw fixation and were treated with supplemental DBF allograft anchors during primary or revision surgery. The need for DBF anchors was determined by evaluating preoperative computed tomography (CT) scans (for revision surgery) and by the surgeons’ tactile feedback intraoperatively during pedicle screw insertion and removal. After determining the pedicle screw void diameter with a sizing instrument, DBF anchors and pedicle screws of the same diameter were placed into the void. CT scans were obtained on postoperative day 2 to assess pedicle breach, pedicle fracture, or anchor material extrusion and at 6 and 12 months postoperatively to assess screw loosening. Thereafter, to minimize radiation exposure, CT scans were only performed for recurrence of pain.
Results Twenty-three patients (79% women; mean age, 74 years) received 50 lumbosacral pedicle screws augmented with DBF anchors. Most surgeries (n = 18, 78%) were revisions, and most anchors were inserted into revision pedicle screw trajectories (n = 33, 66%). Day-2 CT scans revealed no pedicle breach/fracture or extrusion of anchor material. During a mean follow-up of 15 months (12–20 months), no screw loosening was detected, and no patient required pedicle screw revision surgery. There were no adverse events attributable to DBF allografts.
Conclusions DBF allograft anchors appear to be safe and effective for augmenting pedicle screws during revision surgeries in female elderly patients with reduced bone density.
Clinical Relevance Clinically, DBF reduced the rate of pedicle screw loosening in patients with reduced bone density. A significant reduction in screw loosening can decrease the need for revision surgeries, which are costly and carry additional risks. Enhanced bone integration from the DBF may promote better healing and long-term stability.
Level of Evidence 3.
- Allograft
- augmentation
- elderly
- fiber anchor
- lumbar
- pedicle screw
- reduced bone density
- revision
- screw loosening
- spine
Introduction
Pedicle screw loosening following lumbar instrumented fusion is a major problem in patients with reduced bone density, occurring in more than 50% of individuals.1 Screw loosening is more frequent when an interbody cage is not used and in patients who are elderly or undergo multilevel fusion.1–3 The issue of screw loosening is an ongoing challenge for surgeons, especially as the frequency of revision surgery in elderly patients with reduced bone density increases.4
Reduced bone density is typically identified by dual-energy x-ray absorptiometry.5 Management of reduced bone density is best accomplished with a team approach, including a primary care physician and an endocrinologist.6 While medical interventions can improve bone quality, these interventions may not be possible or effective prior to spinal surgery.6
Augmentation of pedicle screws with cement is one option currently available to improve pedicle screw pull-out strength,7 but cement extravasation remains a substantial concern, especially during revision surgery. Cement leakage can cause neural, vascular, and pulmonary complications. A recent meta-analysis found an overall 21.8% risk of cement leakage, with pulmonary cement embolism occurring in 3.0% of patients.8 Cement augmentation also prolongs surgical time, requires frequent fluoroscopy, and necessitates protective lead gowns for the surgical team.9 Augmentation with cement can be technically challenging and often increases the difficulty of subsequent revision surgery. Evidence for the effectiveness of cement augmentation is mixed.10 Although cement can fixate the distal screw tip, it may create a pivot point that contributes to screw toggling proximally in the pedicle and subsequent loosening.11
Demineralized bone fiber (DBF) anchors are a novel, United States Food and Drug Administration–approved technology consisting of molded allografts inserted directly into the pedicle before screw insertion. Although DBF anchors have been demonstrated to improve pull-out strength on biomechanical testing, no peer-reviewed publications have provided clinical data on patient outcomes associated with the use of these anchors.
In this study, we evaluated the effectiveness of DBF anchors for preventing screw loosening in elderly patients with reduced bone density who underwent primary or revision lumbar surgery.
Materials and Methods
This prospective multicenter study included elderly patients with reduced bone density requiring lumbar pedicle screw fixation who were treated with supplemental DBF anchors between 1 November 2021 and 1 July 2022. The study was approved by our Institutional Review Board (Epworth HealthCare EH2023-1009), and the DBF anchors were approved by the Australian regulatory body (Therapeutic Goods Administration).
Inclusion and Exclusion Criteria
All elderly patients treated with DBF anchors during the study period were included. The elderly demographic was defined as individuals older than age 65 years in accordance with the definition of the National Institutes of Health.12 All patients underwent dual-energy x-ray absorptiometry prior to surgery. DBF anchors were indicated when the T-score was –1.0 SD or less (reflecting osteopenia or osteoporosis), although not all patients with reduced bone density received DBF anchors. Patients undergoing primary or revision surgery were included, whereas those with malignancy, active infection, or acute spine trauma were excluded.
DBF Anchors
DBF Fiber Anchors (TheraCell, Inc., Los Angeles, CA; Australian Biotechnologies, Sydney, Australia) are made of osteoconductive and osteoinductive material.13 They have a pointed distal tip for insertion and a proximal flare to resist migration and are manufactured by shaving the cortex of long donor bones to produce strands of longitudinal fibers. This process preserves the donor bone microstructure and collagen alignment. The anchors are cleaned with supercritical pressurized carbon dioxide,14 which is a benign solvent. Gamma irradiation is not used because it damages the osteogenic properties of bone. The allografts are molded into grafts with a length of 30 mm and of varying diameters and then heat-treated to preserve their shape (Figure 1). They are subsequently lyophilized/freeze-dried for storage at ambient temperature.

Demineralized bone fiber anchors of different diameters. All are 30 mm in length.
DBF anchors are applied prior to screw insertion to provide support for the fixation device in the pedicle. They cost approximately US$600 to US$2480, depending on local regulations and geography.
DBF Anchor Use During Primary Surgery
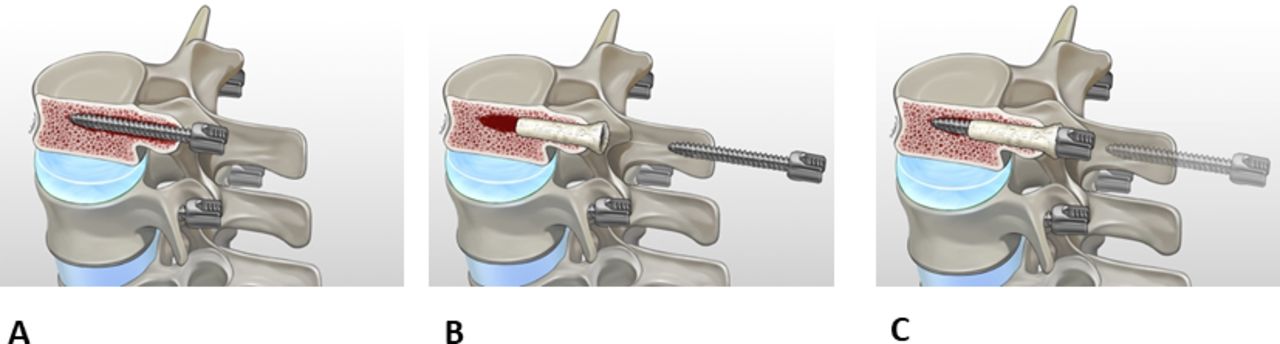
Pedicles were prepared in the usual fashion. During pedicle cannulation, if the surgeon determined that a tap or pedicle screw was loose by tactile feedback, a DBF anchor was sized and placed (Figure 2). A sizing instrument was inserted into the pedicle void to determine the diameter of the required anchor. The surgeon then asked the scrub nurse to open the package containing the corresponding sterile implant. The same anchor-sizing tool was then used to push the anchor into the cannulated pedicle screw tract. The proximal flange prevented the anchor from being pushed too far anteriorly during insertion, and the anchor flange may be pressed down with blunt instruments (Figure 3). Once inserted into the pedicle, each anchor was tapped with a 4.5-mm tap to a depth of 10 mm. For larger anchors (≥7 mm), an additional larger tap was used to increase the size of the starter hole to facilitate initial screw purchase in the anchor. In all cases, the diameter of the anchor was the same as the diameter of the pedicle screw.

(A) A loose screw is identified intraoperatively and subsequently explanted. (B) An appropriately sized demineralized bone fiber anchor is placed into the cannulated pedicle screw tract. (C) A screw of the same diameter is then placed through the anchor.

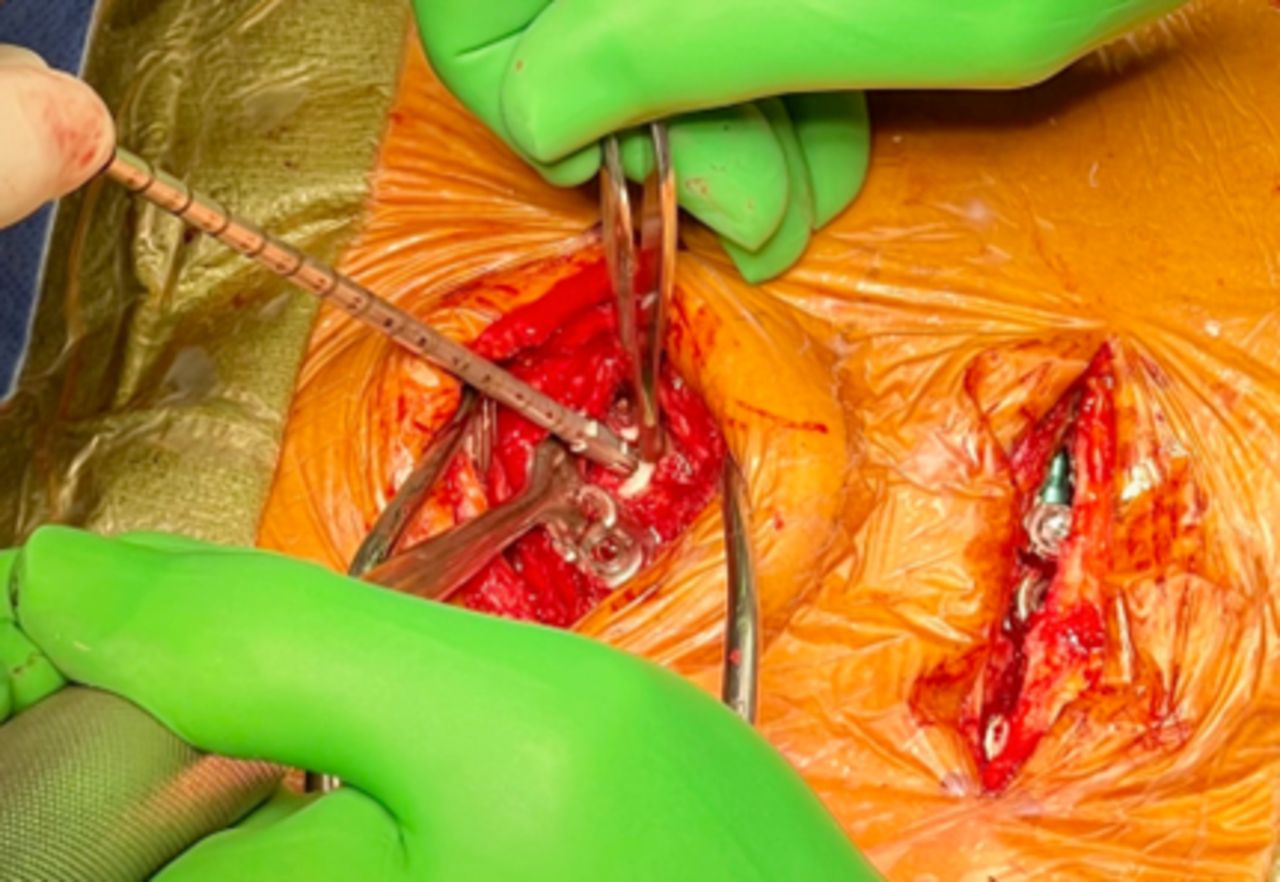
Demineralized bone fiber anchor insertion into a pedicle void from an explanted screw during revision surgery.
DBF Anchor Use During Revision Surgery
Loose screws during revision surgery were identified by preoperative imaging and intraoperative assessment. The explanted pedicle screw diameter was not used to determine the new screw or anchor size. After the pedicle screw was removed, the anchor sizing instrument was used to determine the required anchor diameter. A screw diameter matching the anchor diameter was subsequently inserted; for example, if a 7.5 mm anchor was sized and used, then a 7.5 mm screw was inserted. The procedures for anchor insertion, tapping, and pedicle screw placement were the same as those used for the primary surgery cases.
Postoperative Computed Tomography
Computed tomography (CT) was performed 2 days postoperatively to detect pedicle breach or fracture or extrusion of DBF anchor material. Follow-up CT scans were obtained at 6 and 12 months after surgery to assess screw loosening as part of routine clinical follow-up. Thereafter, to minimize radiation exposure, CT scans were only performed for recurrence of pain. An independent radiologist blinded to the treatment evaluated the CT scans.
Results
A total of 23 patients (78% women) received 50 lumbosacral pedicle screws augmented with DBF anchors (Table). The procedures were performed by 3 senior spine surgeons at 3 tertiary spine centers. The patients’ mean age was 74 years (range, 67–84 years), and the mean T-score was –1.7 SD (range, –1.1 to –2.6 SD). The majority of procedures were revision operations (18/23, 78%), with a mean time from original surgery to revision surgery of 22 months (range, 5–98 months). Most anchors were inserted into revision pedicle screw trajectories (33/50, 66%).
Patient demographics.
The mean follow-up duration after DBF anchor surgery was 15 months (range, 12–20 months), and no patients were lost to follow-up. No pedicle breaches, pedicle fractures, or extrusion of anchor material was detected on postoperative day 2 CT imaging. Follow-up CT imaging at 6 and 12 months and after 12 months for recurrence of pain revealed no periprosthetic lucencies (haloing) indicative of screw loosening. Follow-up imaging at 6 and 12 months revealed reconstitution of posterior cortical bone beneath the anchor flange and no periprosthetic lucencies (haloing) indicative of screw loosening (Figure 4).

(A–C) Preoperative computed tomography (CT) images showing pedicle screw lucencies indicative of left L5 and right S1 screw loosening. (D–F) Postoperative CT at 12 months showing reconstitution of posterior cortical and periprosthetic cancellous bone with no evidence of left L5 or right S1 screw loosening.
There were no recorded adverse events (eg, anterior anchor migration or neural, vascular, or visceral injuries) attributable to DBF anchors. No revision surgery was required to replace pedicle screws during the follow-up period.
Discussion
Screw loosening following lumbar instrumented fusion contributes to pseudoarthrosis and worse clinical outcomes.15 Haloing around pedicle screws on CT images11 or increased radiotracer update on isotope bone scans indicate the presence of screw loosening.16
Preventive measures available to surgeons to reduce the incidence of screw loosening include optimizing bone density through pharmacological management by an endocrinologist,6,17 encouraging smoking cessation,5 maximizing the diameter and accuracy of pedicle screws by utilizing image guidance or robotics,18 avoiding chromium-cobalt rods, limiting fusions to <5 levels, and using cement augmentation.19,20 Use of wider footprint cages during anterior column surgery may also reduce subsidence and subsequent screw loosening.1 However, all of these techniques have limitations.
DBF anchors are a promising new approach to reduce screw loosening, as most of the screw pull-out strength arises from the pedicle.21 These anchors encase screws with allograft in the pedicles, thereby reinforcing screws at their strongest point, in contrast to injecting cement into the weaker vertebral body.
The rate of pedicle screw loosening in spinal fusion surgery ranges from <1% to 15% in patients without osteoporosis15 but can be >50% in osteoporotic vertebrae.1 In this study, we evaluated the effectiveness and safety of DBF anchors in a patient population at high risk of pedicle screw loosening: elderly patients with reduced bone density undergoing primary or revision surgery. Our study cohort included mostly women, which is consistent with reduced bone density being more common in women.17 The natural history of failed fusion secondary to screw loosening typically involves screw loosening as early as 6 weeks in patients with osteoporosis (because of poor bone formation), with graft failure (from pseudoarthrosis) usually occurring 6 to 12 months after surgery.3 Thus, our follow-up duration of 12 to 20 months covered this period of increased risk.
Cement augmentation has been available to spine surgeons for more than 4 decades,22 but its usage remains sporadic. Contemporary cementing techniques utilize cannulated pedicle screws with fenestrations at the distal third of the screw.19 Polymethylmethacrylate is injected through the distal tip of the screw, typically delivering between 1.0 and 3.0 mL of cement into the vertebral body.7 The use of cement augmentation adds time to surgery, requires frequent fluoroscopy and the wearing of lead gowns, is technically difficult, risks cement extravasation,16 and can make future revision surgery more challenging.
Furthermore, Choy et al described a biomechanical problem with the use of cement augmentation.11 Fixation of the distal tip of the screw with cement can create a fulcrum effect whereby micromovements may lead to toggling of the proximal uncemented portion of the screw within the pedicle. Repetitive toggling can lead to the creation of a halo effect around the screw in the pedicle and worsen screw loosening.11
Cement augmentation also has potential economic drawbacks, as it requires low-viscosity cement, a delivery device, and a cannulated fenestrated pedicle screw system. The costs for the cement and delivery devices vary considerably,23 while fenestrated cannulated pedicle screws are more complex and more expensive to manufacture than nonfenestrated noncannulated screws.24 Overall, the conflicting evidence of clinical benefits of cement augmentation, combined with its potential disadvantages and variable utilization, suggests the need for additional options to prevent screw loosening.10
DBF anchors add to the cost of spinal fusions. Each DBF anchor costs between US$600 and US$2480, with the exact cost varying across regions. This additional cost may be justified if DBF anchors reduce the need for revision surgery. Revision spinal surgery is expensive, with an average cost exceeding US$20,000 to replace a misdirected or loose pedicle screw.25 No patient in our cohort required revision surgery, although higher-powered studies with larger sample sizes are necessary to determine whether revision surgery rates are truly reduced by using DBF anchors. DBF anchors may also reduce costs by allowing reuse of removed loose pedicle screws rather than upsizing to new, larger diameter screws. Nevertheless, DBF anchors are more expensive than cement on a per-screw cost basis. There is currently insufficient information to compare clinical outcomes after cement augmentation vs DBF anchors or to perform a comparative cost analysis of the 2 techniques. However, based on our small cohort, the safety profile of DBF anchors seems favorable.
The strengths of this study included the prospective evaluation of surgical outcomes and the performance of the same surgical technique by 3 experienced spine surgeons from 3 tertiary spine centers. Our follow-up period encompassed the high-risk period (within 12 months) for postoperative pedicle screw loosening. There was a low number of male patients (n = 5) and anchor use in primary surgeries (n = 5) within this cohort. Therefore, we cannot draw conclusions for these subsamples. Furthermore, the use of CT scans reviewed by independent radiologists, rather than plain radiographs, allowed accurate identification of screw loosening. Although this study described our experience in a relatively small patient cohort during medium-term follow-up, we plan to conduct larger multicenter studies with longer follow-ups in the future to determine the clinical efficacy and cost effectiveness of DBF anchors more definitively.
Conclusions
Our early experience with DBF allograft anchors suggests that they are a safe and effective strategy for augmenting pedicle screws during revision lumbar fusion surgeries in female elderly patients with reduced bone density. No pedicle screw loosening was observed postoperatively, and there were no adverse effects attributable to the device. Thus, DBF allograft anchors were effective in preventing screw loosening in a small, but high-risk, group of patients during the first 12 months after surgery, the period when screw loosening is most likely to occur.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests G.M.M., M.S., and G.R. have received travel support from LifeHealthcare. G.M.M. also reports consulting fees from LifeHealthcare, Globus Medical, and A-Tech. M.S. also reports consulting fees from Stryker, Additive Surgical, and SI Bone. T.A.W.Q. is a Stryker Corp. employee. D.T.B has no disclosures.
IRB Approval This study was approved by the IRB at Epworth HealthCare (EH2023 - 1009).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.