


Article Figures & Data
Figures
- Figure 1
Webinar moderator (Kai-Uwe Lewandrowski, MD) and presenters who presented on the following topics: (1) Peter Derman, MD, Texas Back Institute—”Uniportal Transforaminal Discectomy/Foraminotomy“; (2) Zhen-Zhou Li, MD, Department of Orthopedics, Chinese PLA General Hospital, Beijing, China—”Transforaminal Full-Endoscopic Interbody Fusion for Hard Disc Herniation”; (3) Alvaro Dowling, MD, Endoscopic Spine Clinic, Santiago, Chile—”Endoscopic Standalone Lumbar Interbody Fusion”; and (4) Martin Knight, MD, Manchester University, The Spinal Foundation, London, UK—”The Importance of Patient Feedback During Endoscopic Spine Surgery.”
- Figure 2
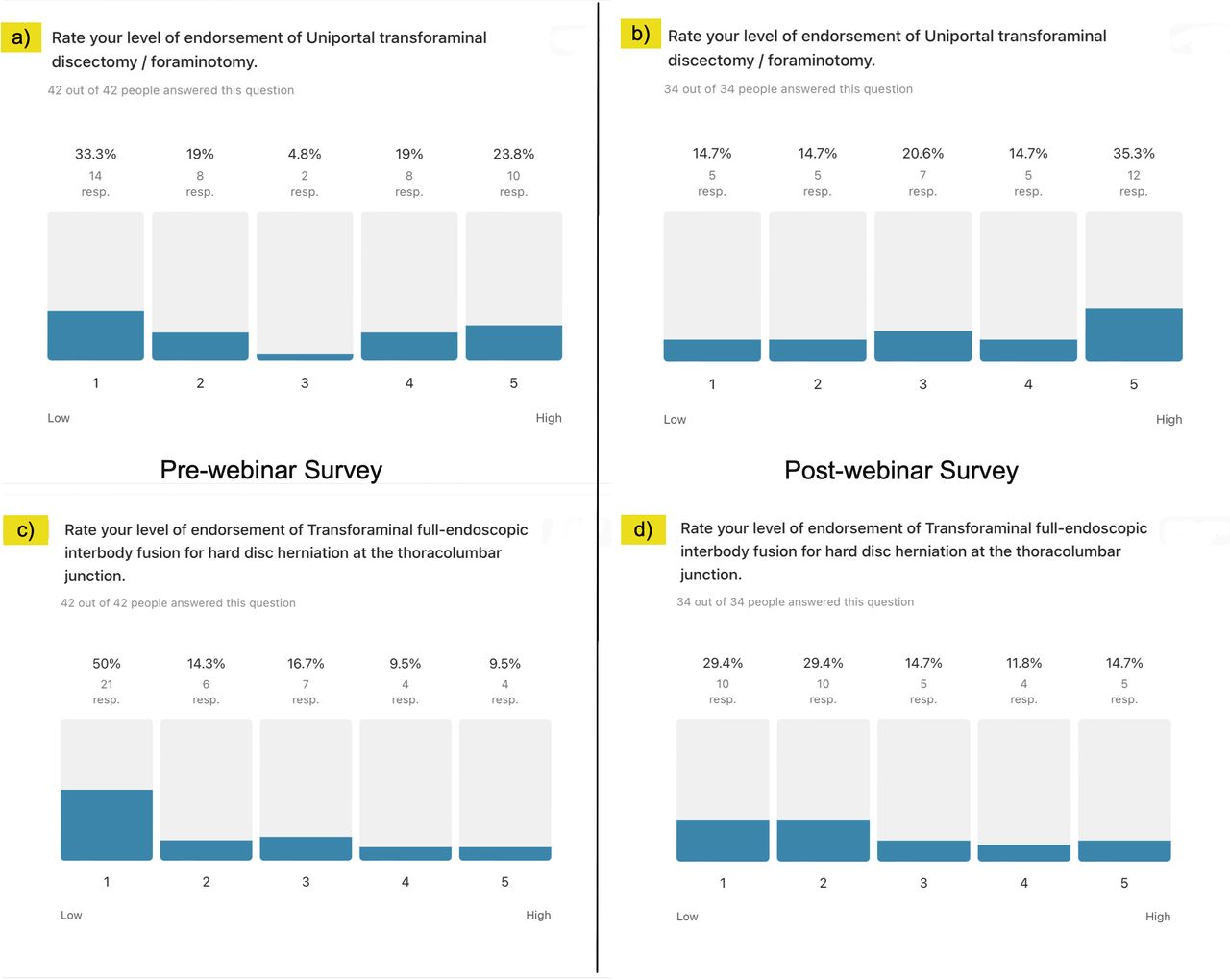
Descriptive statistics of level of endorsement analysis of endoscopic procedures. Regarding confidence in the uniportal transforaminal discectomy/foraminotomy technique, (a) 33.3% of participants had low confidence before the webinar and (b) 35.3% had high confidence after the webinar. Regarding confidence in the transforaminal full-endoscopic interbody fusion for hard disc herniation, (c) 50.0% had low confidence before the webinar and (d) 29.4% had low confidence after the webinar. The descriptive statistical analysis exposed the controversy surrounding the transforaminal full-endoscopic interbody fusion for hard disc herniation.
- Figure 3
Descriptive statistics of level of endorsement analysis of endoscopic procedures. For endoscopic standalone lumbar interbody fusion, (a) 57.1% of participants had low confidence before the webinar (b) 44.1% had low confidence after the webinar. Regarding the need for patient feedback during endoscopic spine surgery, (c) 47.8% had high confidence before the webinar and (d) 58.3% had high confidence after the webinar. The descriptive statistical analysis exposed the controversy surrounding the endoscopic standalone lumbar interbody fusion.
- Figure 4
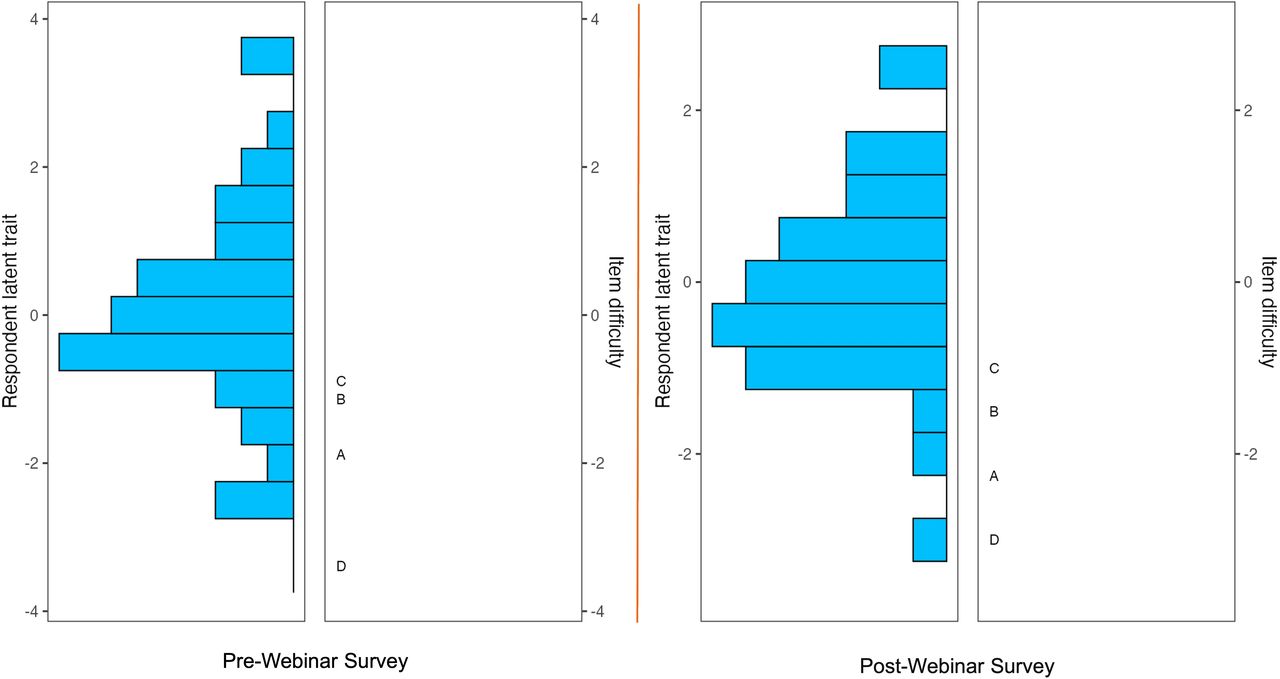
Wright plot obtained in the polytomous Rasch analysis of prewebinar (left panel) and postwebinar (right panel) survey responses. The item response theory polytomous Rasch partial agreement analysis was employed to assess spine surgeons’ level of endorsement of the 4 procedures (test items) presented during the webinar: (a) uniportal transforaminal discectomy/foraminotomy, (b) transforaminal full-endoscopic interbody fusion for hard disc herniation, (c) endoscopic standalone lumbar interbody fusion, and (d) patient feedback during endoscopic spine surgery. On the left side of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The surgeons represented by horizontal bars at the top indicated a higher level of endorsement for the individual test components of endoscopic spinal surgery (positive logits) than those on the bottom (negative logits). On the right, the higher-level endorsement items are listed at the top vs the more controversial ones on the bottom. Directly across from 0, those surgeons had a 50% chance of endorsing a test item. One logit above suggests an approximately 25% chance that the test item was endorsed vs 1 logit below suggests an approximately 75% chance of endorsement. There were no assessment gaps, suggesting there was no redundancy between test items.
- Figure 5
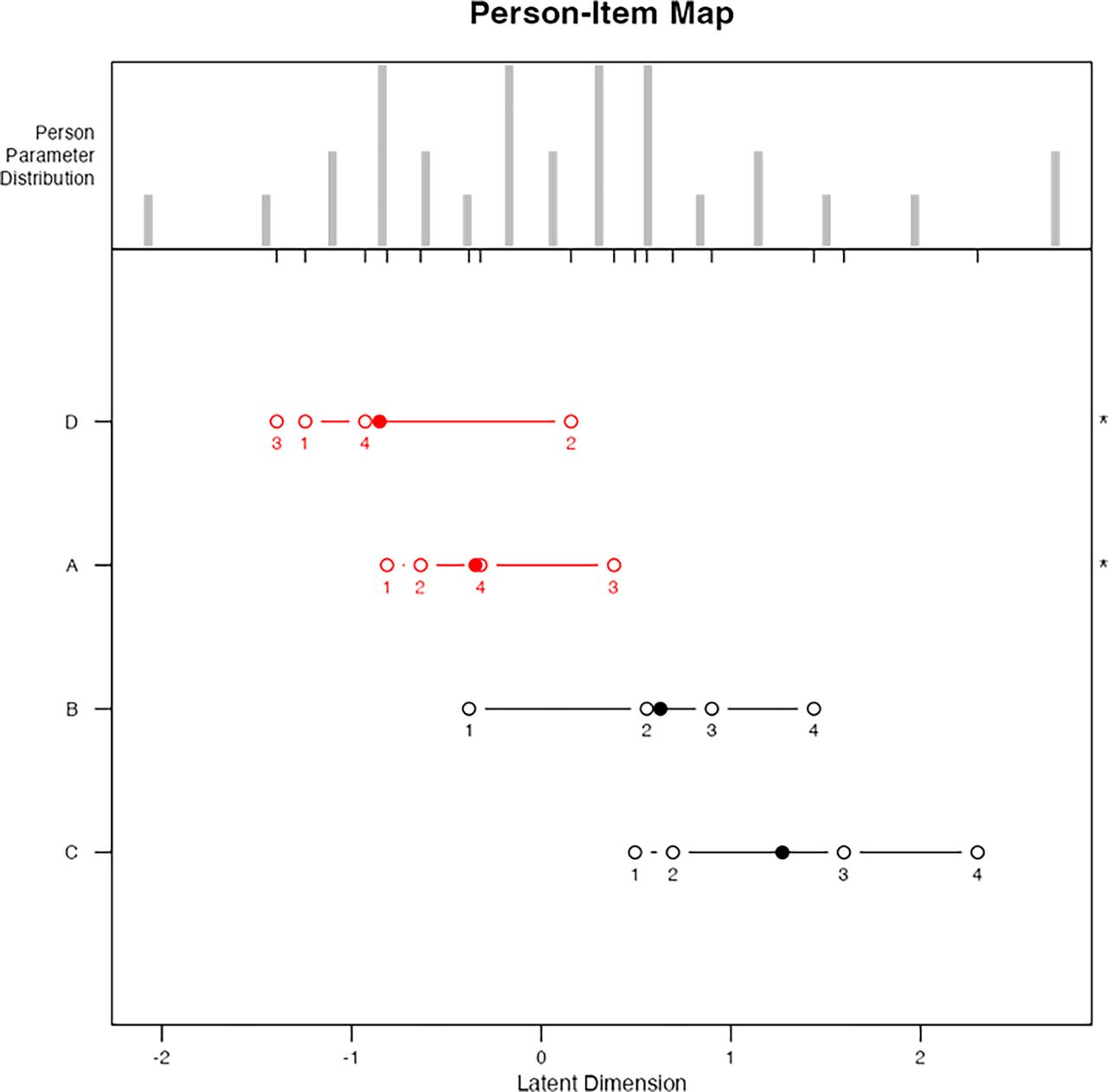
The person-item map of prewebinar survey responses shows the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Contrary to the descriptive statistical analysis (Figure 2), the most challenging item to agree on was item D “patient feedback during endoscopic spine surgery” with the mean logit location (1) shifted to the left. The mean logit location for item A (uniportal transforaminal discectomy/foraminotomy), item B (transforaminal full-endoscopic interbody fusion for hard disc herniation), and item C (endoscopic standalone lumbar interbody fusion) were more shifted to the right of the plot, therefore showing more intense partial agreement for these items. The person-item maps also illustrate that items were reasonably well distributed. However, some surgeons could not be measured as reliably as the majority by this set of items, indicating the test items were either too intense or not intense enough for them (item D; logit location 1 to the left). The analysis also showed disordered thresholds of endorsement for the 4 test items, suggesting that surgeons had difficulty consistently discriminating between response categories ranging from strongly disagree, disagree, agree, to strongly agree—a problem observed when there are too many response options not measuring the opinions. All 4 of the item topics before being presented during the webinar were disordered and are shown in red. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum, suggesting a poor fit to the Rasch model with statistically significant difference between the observed values and the values predicted by the model.
- Figure 6
The person-item map of postwebinar survey responses shows the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x-axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Contrary to the descriptive statistical analysis (Figure 3), after the webinar, the most challenging item to agree on was still item D, patient feedback during endoscopic spine surgery, with the mean logit location being out of order (3, 1, 4, and 2) and item A (uniportal transforaminal discectomy/foraminotomy) with the mean logit location also out of order (1, 2, 4, and 3), suggesting that surgeons had difficulty consistently discriminating between response categories—a problem observed when there are too many response options not measuring the opinions. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum suggesting a poor fit to the Rasch model with statistically significant difference between the observed values and the values predicted by the model. Contrary to the descriptive statistics, which suggested item B (transforaminal full-endoscopic interbody fusion for hard disc herniation) and item C (endoscopic standalone lumbar interbody fusion) were controversial, these items were shifted more to the right of the plot, therefore showing more intense partial agreement and endorsement for these items. The clinical evidence presented in these item presentations during the webinar was more convincing to the webinar participants. The person-item maps on top of the graph also illustrate that items were reasonably well distributed.
- Figure 7
Category probability curves (CPCs) are shown for test items uniportal transforaminal discectomy/foraminotomy and endoscopic standalone lumbar interbody fusion. They visually depict the relationship between the probability of a particular category being chosen and the respondent surgeon’s stance generated for each category. After the webinar, disordered sequencing was converted to ordered sequencing of the thresholds (crossover between CPCs of 2 neighboring categories having an equal likelihood of selection), which were graphically demonstrated for the endoscopic standalone lumbar interbody fusion. As a result of what participants learned during the webinar about the endoscopic standalone fusion technique and its associated clinical outcomes, response data conformed to the Rasch model, suggesting endorsement without significant confounding factors. However, the portion of surgeons with low confidence in this procedure (Category 1) and who could not be convinced otherwise remained the same. The response threshold sequencing remained disordered for uniportal transforaminal discectomy/foraminotomy, suggesting that for surgeons located anywhere along the response continuum, and especially for those surgeons located at the maximum value for this category, disagreeing with the item (ie, selecting category strongly disagree) is never the most probable response. Confounding factors not captured by the survey were likely present.
- Figure 8
Two examples of outlier-sensitive means statistics (outfit analysis) based on the conventional sum of squared standardized residuals, which is more sensitive to unexpected observations, are shown. Surgeon prewebinar (a and c) compared with postwebinar (b and d) endorsement responses showed greater outfit (0.840 prewebinar vs 1.042 postwebinar) from the model predicted by the Rasch analysis for item A (uniportal transforaminal discectomy/foraminotomy) after the webinar, suggesting the presence of confounding factors affecting responses on item A that were not convincingly resolved in the presentation. The outfit analysis for item B (transforaminal full-endoscopic interbody fusion for hard disc herniation) showed greater outfit (0.532 prewebinar vs 0.727 postwebinar) after the webinar as well. Postwebinar responses fit the Rasch model well. Outfit data between 0.6 and 1.4 indicate good fit of the Rasch model.
- Figure 9
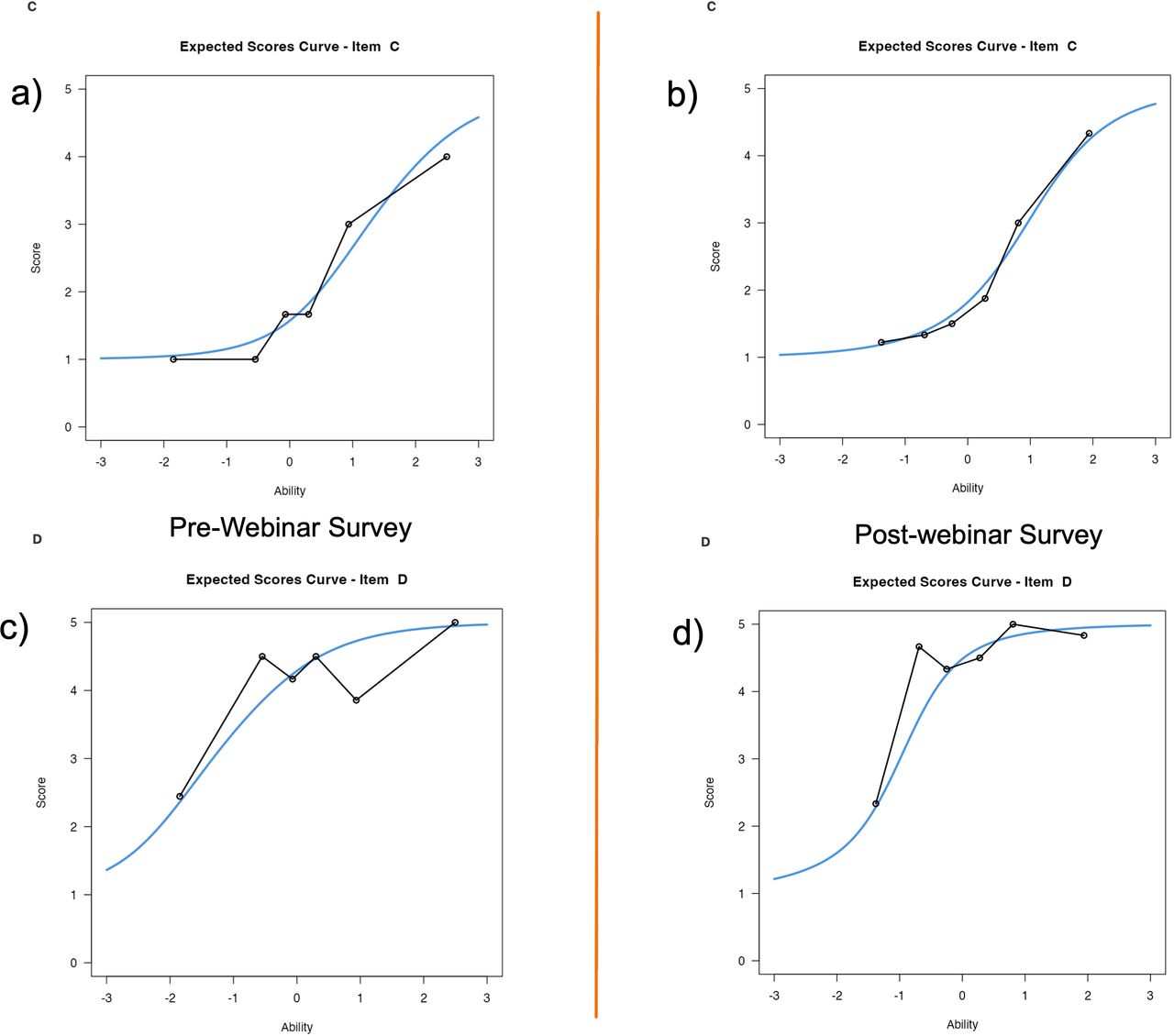
Two examples of outlier-sensitive means statistics (outfit analysis) based on the conventional sum of squared standardized residuals, which is more sensitive to unexpected observations, are shown. Surgeon prewebinar (a and c) compared with postwebinar (b and d) endorsement responses showed similar outfit (0.721 prewebinar vs 0.793 postwebinar) from the model and better graphic fit predicted by the Rasch analysis for item C (endoscopic standalone lumbar interbody fusion) after the webinar, suggesting that the presentation was able to resolve many confounding factors affecting responses on item C. The outfit analysis for item D (patient feedback during endoscopic spine surgery) showed lesser outfit (1.878 prewebinar vs 1.390 postwebinar) after the webinar, indicating that the presentation on item D was convincing and resulted in responses that followed the Rasch model better. Outfit data between 0.6 and 1.4 indicate good fit of the Rasch model.









In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.