


Article Figures & Data
Figures
- Figure 1
Webinar moderator (Kai-Uwe Lewandrowski, MD) and presenters who presented on the following topics: Gregory Basil, MD, Assistant Professor of Neurosurgery and Director of Endoscopic Spine Surgery at the University of Miami, Miller School of Medicine, discussed overcoming the steep learning curve associated with spinal endoscopy, emphasizing the importance of education and structured training programs. Brian Kwon, MD, of New England Baptist Hospital and Assistant Clinical Professor of Orthopedic Surgery at Tufts University School of Medicine, presented insights on biportal endoscopic laminectomy/discectomy and endoscopic transforaminal lumbar interbody fusions focusing on the advantages and challenges of these minimally invasive approaches. Xinyu Liu, MD, from Qilu Hospital of Shandong University, presented a comparative analysis of clinical outcomes and muscle invasiveness between unilateral biportal endoscopic decompression and percutaneous endoscopic interlaminar decompression for lumbar spinal stenosis, highlighting differences in recovery and postoperative complications. Last, Gabriel Oswaldo Alonso Cuéllar, DVM, EdM, MSc, from the Latin American Endoscopic Spine Surgeons LESS Invasiva Academy in Bogotá, Colombia, explored the innovative technique of lumbar endoscopic decompression combined with simultaneous interspinous process spacer implantation for the treatment of spinal stenosis, offering insights into long-term outcomes and functional recovery.
- Figure 2
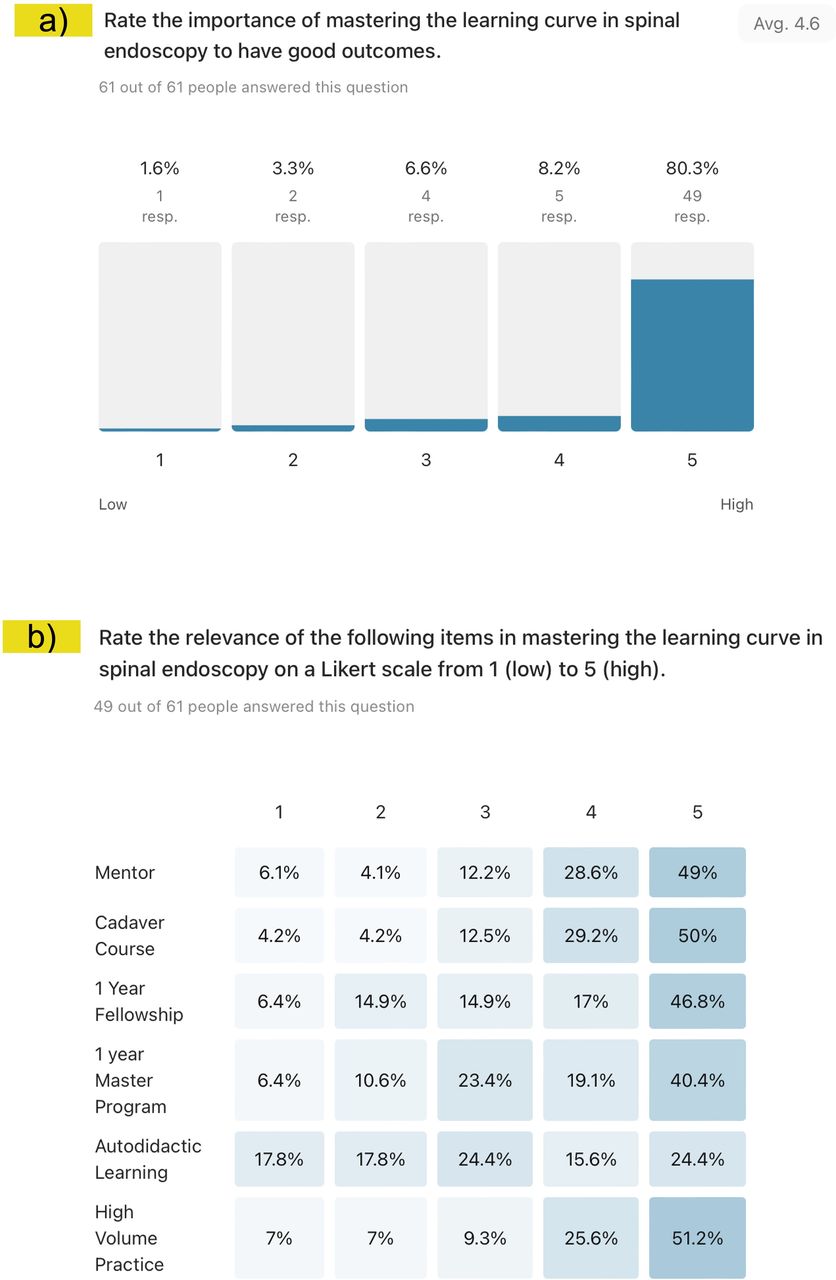
Prewebinar descriptive statistics of the level of importance of the learning curve to master endoscopic spine surgery: (a) 80.3% of surgeons indicated that there is a learning curve to overcome. (b) The percentage breakdown from low- to high-level endorsement is shown within each learning item. Approximately half of the responding surgeons endorsed cadaver courses and high-volume surgical practice as essential elements in overcoming the learning curve. Receiving supervised training during a 1-year fellowship or master’s program was less supported. Autodidactic learning was considered the least appropriate.
- Figure 3
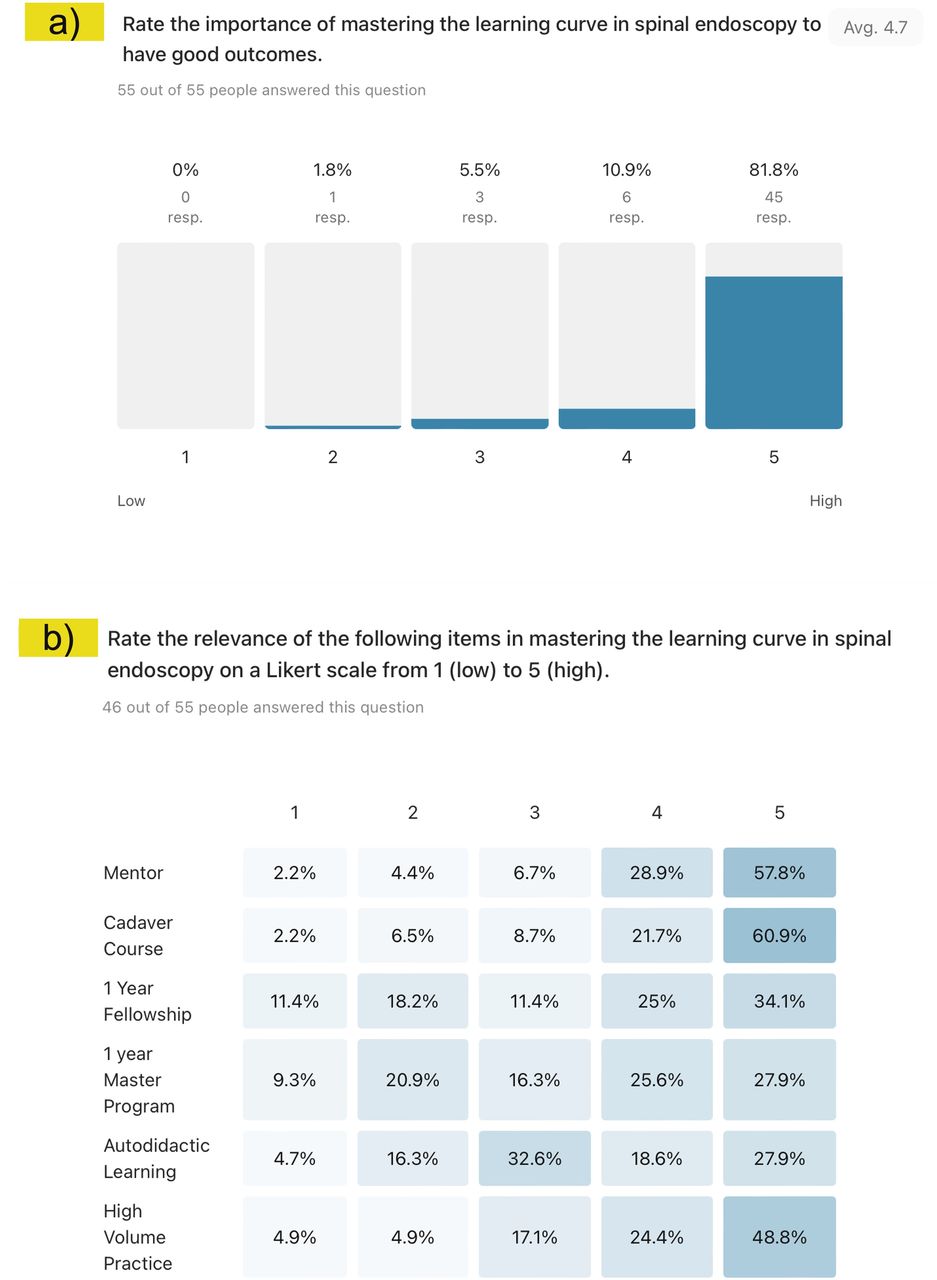
Postwebinar descriptive statistics of the level of importance of the learning curve to master endoscopic spine surgery: (a) 81.8% of surgeons indicated that there is a learning curve to overcome. (b)The percentage breakdown from low- to high-level endorsement is shown within each learning item. More than half of respondents strongly endorsed cadaver courses (60.9%) and having a mentor (57.8%) in overcoming the learning curve. A high-volume surgical practice (48.8%) was also seen as essential in overcoming the learning curve. Receiving supervised training during a 1-year fellowship (34.1%) or master’s (27.9%) program was less supported. Autodidactic learning (27.9%) also lacked high-level support.
- Figure 4
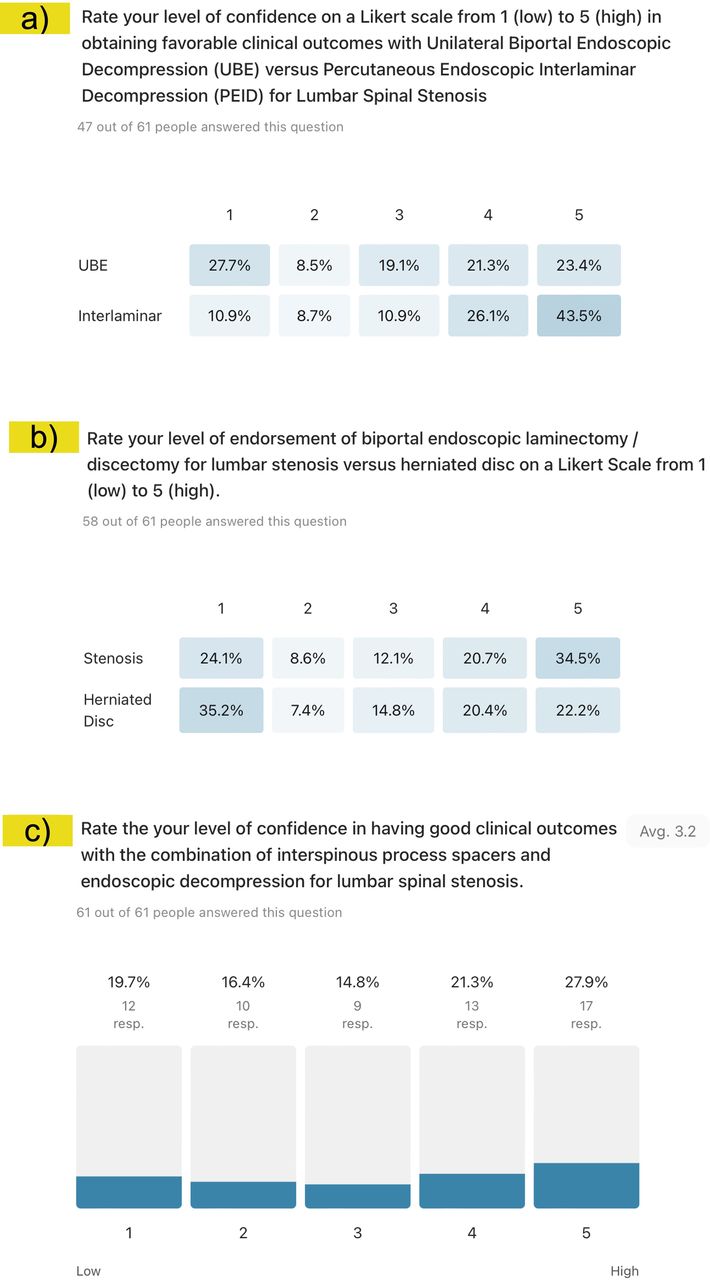
Prewebinar descriptive statistics of level of confidence in achieving favorable clinical outcomes with (a) lateral canal decompression done either with unilateral biportal endoscopic (UBE) decompression or with percutaneous endoscopic interlaminar decompression, (b) UBE decompression for either central canal stenosis or herniated disc, and (c) transforaminal endoscopic decompression and simultaneous placement of an interspinous process spacer (ISP). Prewebinar survey responses showed higher-level endorsements for the interlaminar lateral canal decompression (43.5%; a). The highest endorsement for the UBE central canal decompression for stenosis was 34.5%, and the highest disapproval for herniated discs was 35.2% (b). Only 27.9% of surgeons gave a high-level endorsement for the combination of transforaminal endoscopic decompression with simultaneous placement of an ISP, with nearly equal levels of endorsement throughout the other categories (c).
- Figure 5
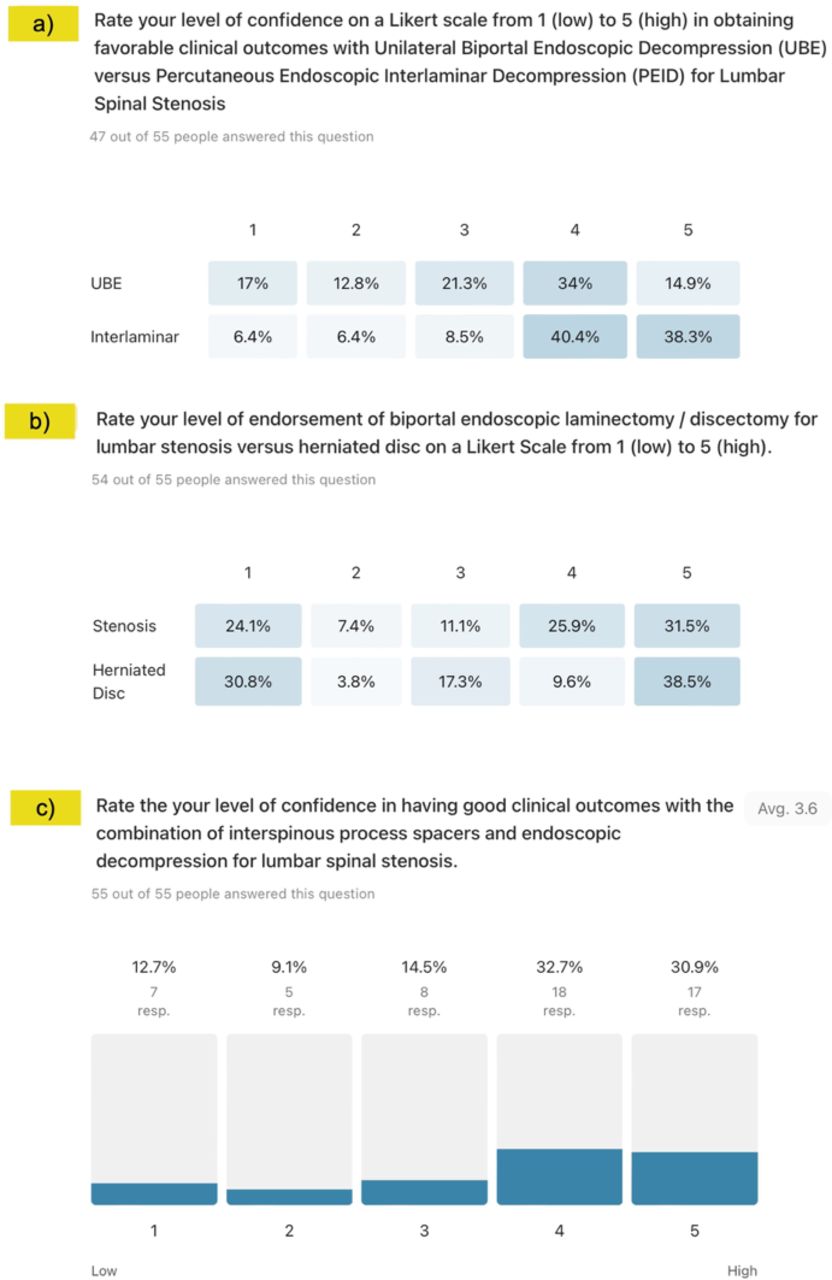
Postwebinar descriptive statistics of level of confidence in achieving favorable clinical outcomes with (a) lateral canal decompression done either with unilateral biportal endoscopic (UBE) decompression or with percutaneous endoscopic interlaminar decompression, (b) UBE decompression for either central canal stenosis or herniated disc, and (c) transforaminal endoscopic decompression and simultaneous placement of an interspinous process spacer. Postwebinar survey responses showed an endorsement shift to higher-level categories (levels 4 and 5) for the interlaminar lateral canal decompression (78.7%), up from 67.6%, and the UBE lateral canal decompression of 48.9% up from 44.7% (a). There was a minimal response shift for the UBE laminectomy decompression of the central canal for either stenosis or herniated disc (b). There was an endorsement for the combination of transforaminal endoscopic decompression with simultaneous placement of an interspinous process spacer with a high-level endorsement (categories 4 and 5) of 63.6%, up from 49.2% prewebinar (c).
- Figure 6
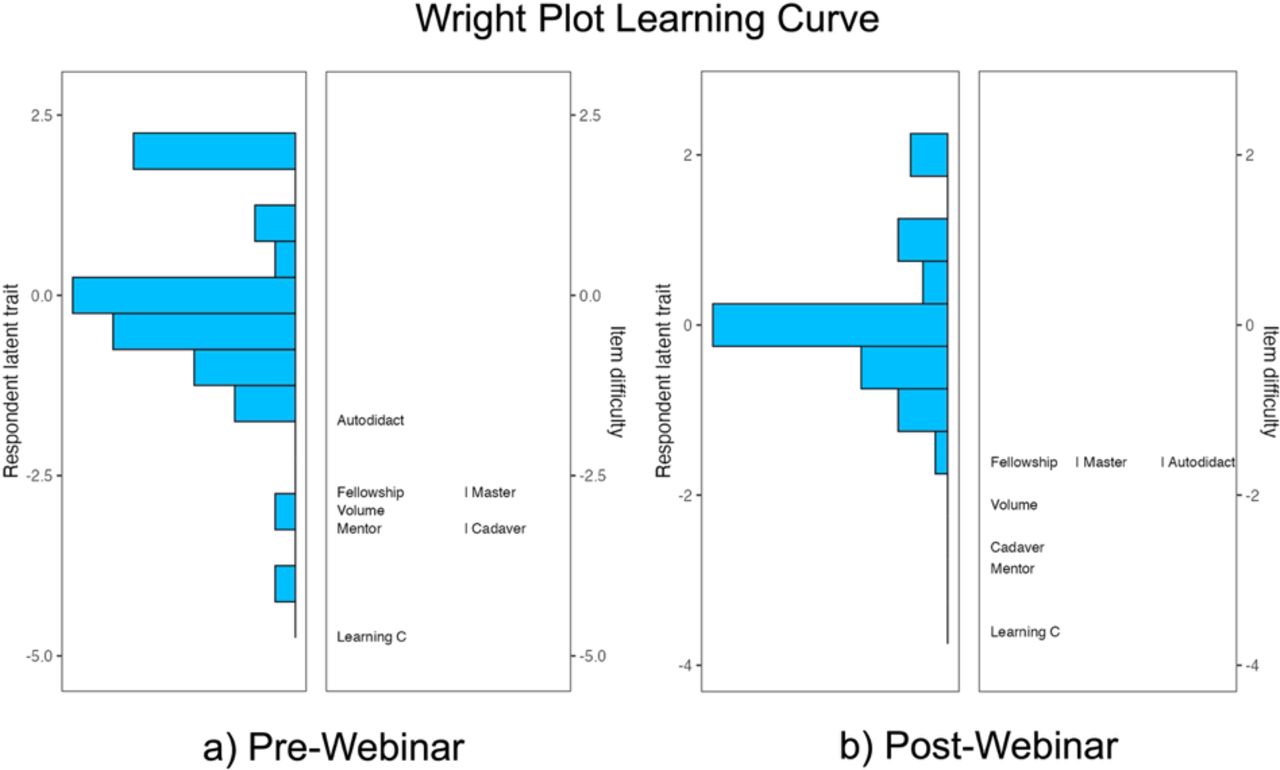
Wright plot obtained in the polytomous Rasch analysis of prewebinar (left panel) and postwebinar (right panel) survey responses regarding the importance of mastering the endoscopy learning curve, which was the easiest item for responding surgeons to agree on. The item response theory polytomous Rasch partial agreement analysis was employed to assess spine surgeons’ level of endorsement of the 6 frequently employed endoscopic spine surgery training methods (test items). On the left side of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability and intensity of partial agreement. The surgeons, represented by horizontal bars at the top, represented the highest level of endorsement. On the right of the Wright plot, the harder-to-agree-on items are listed at the top vs the easier-to-agree-on ones at the bottom. Directly across from 0, those surgeons had a 50% chance of endorsing a test item. There were 4 assessment gaps on the prewebinar survey and 1 on the postwebinar survey. There was some redundancy between prewebinar test items, as shown by the same ranking for fellowship and master program and mentorship and cadaver course. Similar redundancy existed for test items fellowship and master program, as well as autodidactic learning in the postwebinar survey. Cadaver course and mentorship were the most preferred elements in the training of future endoscopic spine surgeons.
- Figure 7
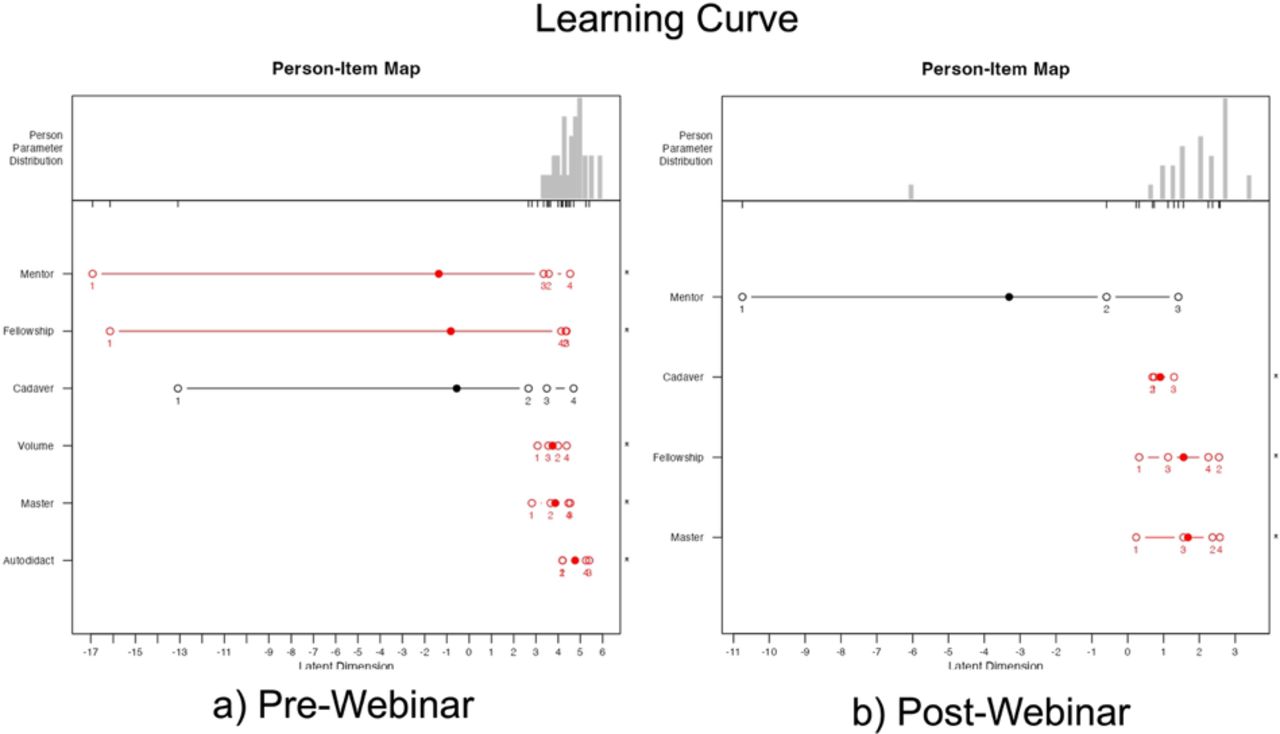
The person-item map of prewebinar (a) and postwebinar (b) survey responses shows the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Disordered items are shown in red and ordered ones in black. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum, suggesting a poor fit to the Rasch model without any statistically significant difference between the observed values and the values predicted by the model. In comparison to prewebinar descriptive statistics (Figure 1), the most high-intensity items were “autodidactic learning style,” “surgical master program in endoscopic spine surgery,” and having a “high volume practice” with the mean logit location shifted to the left. Because these items were out of order, some surgeons could not be measured as reliably as the majority by this set of items, indicating the test items were either too intense or not intense enough for them. The analysis also showed disordered thresholds of endorsement for the 5 of 6 test items. With the exception of “attending a cadaver course,” all test items were out of order (logits shown in red) in the prewebinar survey suggesting that surgeons had difficulty consistently discriminating between response categories ranging from strongly disagree (1), disagree (2), agree (3), and strongly agree (4)—a problem observed when there are too many response options not measuring the opinions. In the prewebinar survey, the mean logit locations for items “1-year fellowship” and “mentorship” were more shifted to the left of the plot and had an out of order (logits shown in red) wider spread, therefore showing less intense partial agreement for these items. Response analysis from the postwebinar survey for items “surgical master program in endoscopic spine surgery,” “attending a cadaver course,” “1-year fellowship,” and “mentorship” showed that the webinar shifted participants’ perceptions of the importance of having a mentor. This item solicited the highest in-order intensity response. In summary, the Rasch analysis of incoming pre- and postwebinar responses suggested that most surgeons considered having a mentor and attending cadaver courses as the most effective way to master the learning curve in endoscopic spine surgery. The person-item maps also illustrates that items were reasonably well distributed.
- Figure 8
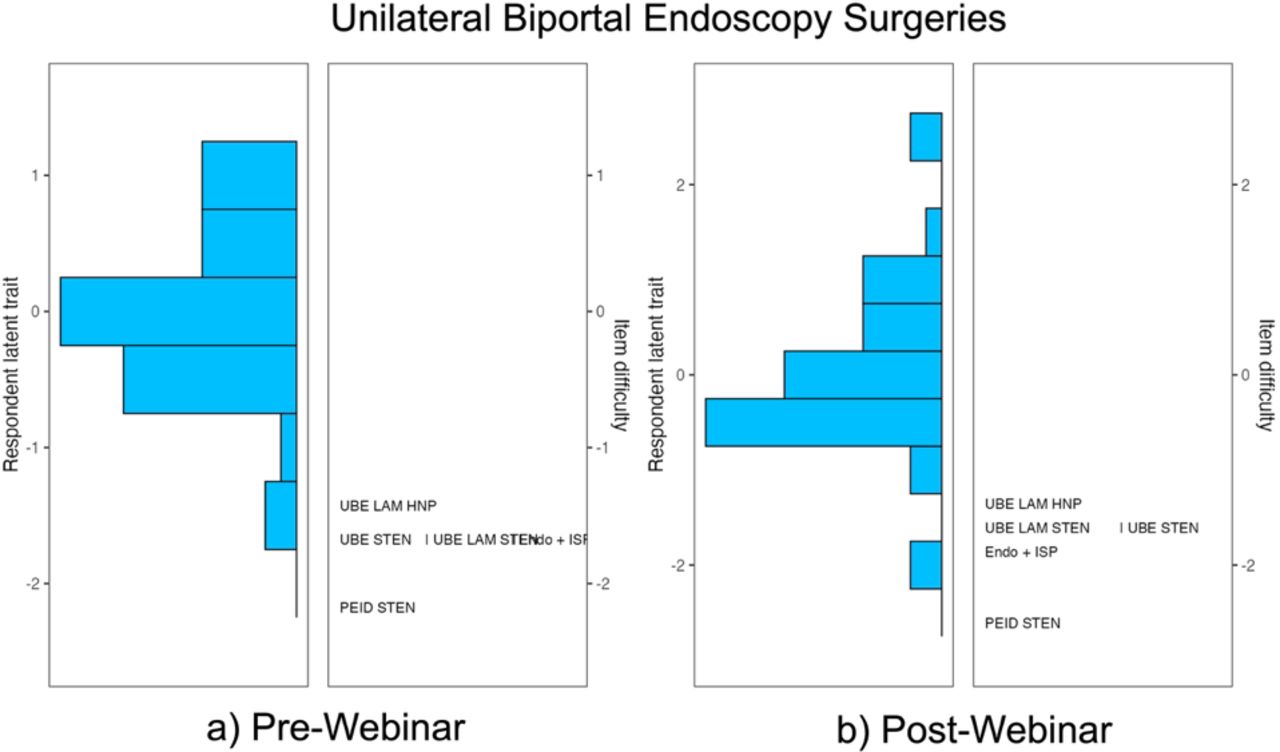
Wright plot obtained in the polytomous Rasch analysis of prewebinar (left panel) and postwebinar (right panel) survey responses. The item response theory polytomous Rasch partial agreement analysis was employed to assess spine surgeons’ level of endorsement of the 5 procedures (test items) presented during the webinar: (a) unilateral biportal endoscopic (UBE) laminectomy for central stenosis (UBE LAM STEN), (b) UBE laminectomy for herniated disc (UBE LAM HNP), (c) UBE decompression for lateral canal stenosis (UBE STEN), (d) percutaneous interlaminar endoscopic decompression for lateral canal stenosis (PEID, and (e) transforaminal endoscopic decompression with simultaneous interspinous process spacer for lateral canal stenosis (Endo + ISP). On the left side of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability or this study experience-based endorsements. The surgeons, represented by horizontal bars at the top, indicated a higher level of endorsement for the individual test components of endoscopic spinal surgery (positive logits) than those on the bottom (negative logits). On the right, the higher-level endorsement items are listed at the top vs the more controversial ones on the bottom. Directly across from 0, those surgeons had a 50% chance of endorsing a test item. One logit above suggests an approximately 25% chance that the test item was endorsed vs one logit below suggesting an approximately 75% chance of endorsement. There were no assessment gaps in the prewebinar survey but 2 in the postwebinar survey. Prewebinar survey analysis showed the log-ranking for UBE STEN, UBE LAM STEN, and Endo + ISP with similar locations in the Wright plot, suggesting that there was some redundancy between test items, and surgeons had difficulty discriminating them based on the survey questions. In the postwebinar survey, the items UBE LAM HNP, UBE LAM STEN, and UBE STEN were the most challenging to agree on. After the webinar, surgeons agreed more readily with the information presented on test item Endo + ISP. The item PEID was the easiest to agree on both before and after the webinar, suggesting wide acceptance of PEID among endoscopic spine surgeons in the treatment of lateral canal stenosis and HNP.
- Figure 9
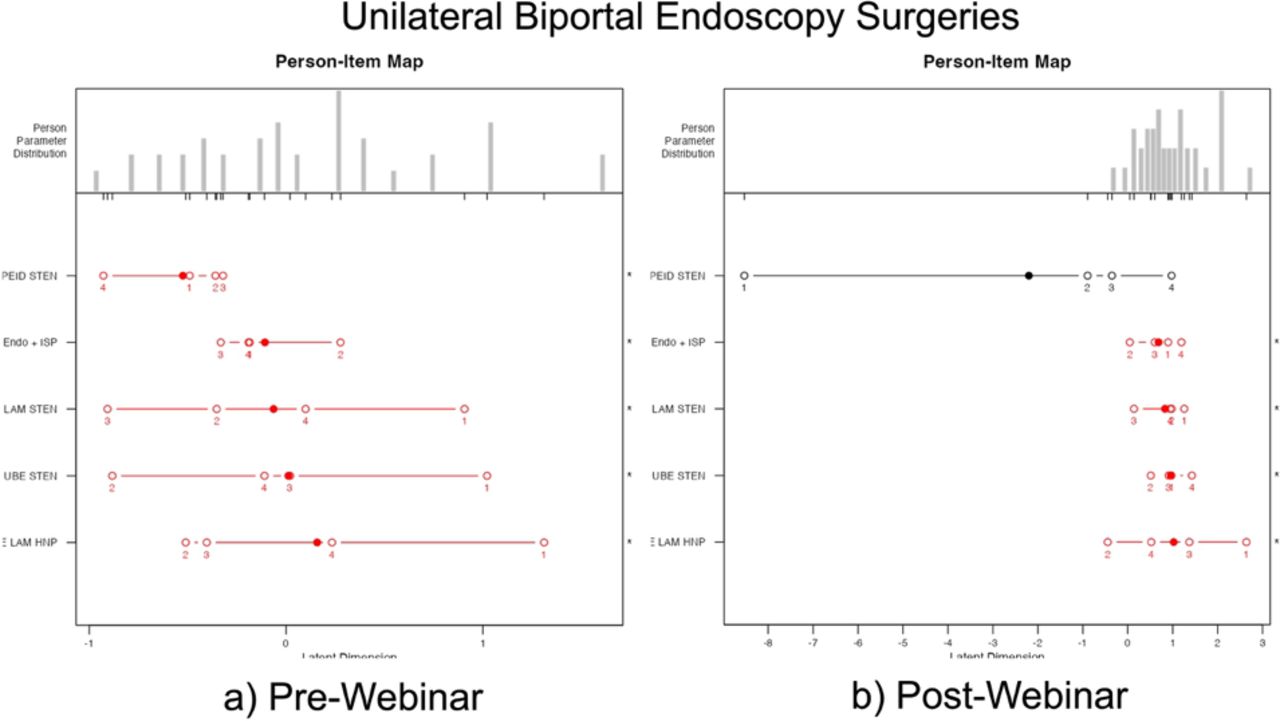
The person-item map of postwebinar survey responses shows the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x axis (labeled “Latent Dimension”). Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Disordered items are shown in red and ordered ones in black. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum suggesting a poor fit to the Rasch model without any statistically significant difference between the observed values and the values predicted by the model suggesting that surgeons had difficulty consistently discriminating between response categories ranging from strongly disagree (1), disagree (2), agree (3), and to strongly agree (4)—a problem observed when there are too many response options not measuring the opinions. In comparison to the descriptive statistical prewebinar analysis (Figure 2), all procedural test items including (a) unilateral biportal endoscopic (UBE) laminectomy for central stenosis (UBE LAM STEN), (b) UBE laminectomy for herniated disc (UBE LAM HNP), (c) UBE decompression for lateral canal stenosis (UBE STEN), (d) percutaneous interlaminar endoscopic decompression for lateral canal stenosis (PEID), and (e) transforaminal endoscopic decompression with simultaneous interspinous process spacer for lateral canal stenosis (Endo + ISP) were challenging to agree upon based on the wide disorderly spread. After the webinar (descriptive statistics shown in Figure 3), the intensity of agreement, still disorderly except for PEID, increased as demonstrated by the logit locations having shifted to the right. The clinical evidence presented in these item presentations during the webinar was convincing to the webinar participants but most noticeably for PEID. The person-item maps on top of the graph also illustrate distribution gaps in the prewebinar analysis and normal distribution in the postwebinar analysis.
- Figure 10
A sample item characteristic curves generated from prewebinar survey responses for unilateral biportal endoscopic decompression for lateral canal stenosis as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: one for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level, which showed no significant difference between orthopedic (reference group) and neurosurgeons (focal group) with the statistics for DIF detection of 1.177 and a P value of 0.555 (Table 3). There were no displayable differences between orthopedic and neurosurgeons.
- Figure 11
A sample item characteristic curves generated from postwebinar survey responses unilateral biportal endoscopic laminectomy for central stenosis (UBE LAM STEN) as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: one for the reference group (orthopedic surgeons—solid lines) and another for the focal group (neurosurgeons—dashed lines). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level, which showed a significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for DIF detection of 16.2144 and a P value of <0.001 (Table 4), suggesting bias in the test item.











Tables
- Table 1
Prewebinar survey model fit analysis and item statistics of the rating scale model.
Procedure Measure SE Measure Infita Outfitb UBE STEN −1.35 0.114 1.087 1.025 PEID −2.04 0.127 0.989 0.994 UBE LAM STEN −1.74 0.116 0.982 0.915 UBE LAM HNP −1.51 0.113 0.936 0.962 Endo + ISP −1.69 0.115 1.093 1.117 Person Reliability MADaQ3 P Scale 0.526 0.204 0.005 Abbreviations: Endo + ISP, transforaminal endoscopic decompression with simultaneous interspinous process spacer for lateral canal stenosis; MADaQ3, mean of absolute values of centered Q_3 statistic with P value obtained by Holm adjustment; PEID, percutaneous interlaminar endoscopic decompression for lateral canal stenosis; UBE LAM HNP, unilateral biportal endoscopic laminectomy for herniated disc; UBE LAM STEN, unilateral biportal endoscopic laminectomy for central stenosis; UBE STEN, unilateral biportal endoscopic decompression for lateral canal stenosis.
↵a Information-weighted mean square statistic.
↵b Outlier-sensitive mean square statistic.
- Table 2
Postwebinar survey model fit analysis and item statistics of the rating scale model.
Procedure Measure SE Measure Infita Outfitb UBE STEN −1.57 0.131 0.744 0.687 PEID −2.48 0.162 0.868 0.948 UBE LAM STEN −1.69 0.131 0.895 0.813 UBE LAM HNP −1.47 0.131 1.092 1.058 Endo + ISP −1.85 0.134 1.343 1.343 Person Reliability MADaQ3 P Scale 0.655 0.284 <0.001 Abbreviations: Endo + ISP, transforaminal endoscopic decompression with simultaneous interspinous process spacer for lateral canal stenosis; MADaQ3, mean of absolute values of centered Q_3 statistic with P value obtained by Holm adjustment; PEID, percutaneous interlaminar endoscopic decompression for lateral canal stenosis; UBE LAM HNP, unilateral biportal endoscopic laminectomy for herniated disc; UBE LAM STEN, unilateral biportal endoscopic laminectomy for central stenosis; UBE STEN, unilateral biportal endoscopic decompression for lateral canal stenosis.
↵a Information-weighted mean square statistic.
↵b Outlier-sensitive mean square statistic.
- Table 3
Prewebinar survey DIF detection procedure for ordinal data based on adjacent category logit model: likelihood ratio using χ2 analysis.
Procedure Statistica P Adjusted P UBE STEN 1.177 0.555 0.818 PEID 3.651 0.161 0.806 UBE LAM HNP 0.848 0.654 0.818 UBE LAM STEN 0.312 0.856 0.856 Endo + ISP 1.027 0.598 0.818 Abbreviations: DIF, differential item functioning; Endo + ISP, transforaminal endoscopic decompression with simultaneous interspinous process spacer for lateral canal stenosis; PEID STEN, percutaneous interlaminar endoscopic decompression for lateral canal stenosis; UBE LAM HNP, unilateral biportal endoscopic laminectomy for herniated disc; UBE LAM STEN, unilateral biportal endoscopic laminectomy for central stenosis; UBE STEN, unilateral biportal endoscopic decompression for lateral canal stenosis.
Note. The adjusted P values were adjusted by likelihood ratio test using multiple comparison.
↵a DIF likelihood ratio statistics are estimated by using difNLR and difORD function.
- Table 4
Postwebinar survey DIF detection procedure for ordinal data based on adjacent category logit model: likelihood ratio χ2 statistics.
Procedure Statistica P Adjusted P UBE STEN 1.9706 0.373 0.906 PEID 0.0565 0.972 0.972 UBE LAM HNP 0.7903 0.674 0.906 UBE LAM STEN 16.2144 <0.001 0.002 Endo + ISP 0.6434 0.725 0.906 Abbreviations: DIF, differential item functioning; Endo + ISP, transforaminal endoscopic decompression with simultaneous interspinous process spacer for lateral canal stenosis; PEID, percutaneous interlaminar endoscopic decompression for lateral canal stenosis; UBE LAM HNP, unilateral biportal endoscopic laminectomy for herniated disc; UBE LAM STEN, unilateral biportal endoscopic laminectomy for central stenosis; UBE STEN, unilateral biportal endoscopic decompression for lateral canal stenosis.
Note. The adjusted P values were adjusted by likelihood ratio test using multiple comparison.
↵a DIF likelihood ratio statistics are estimated by using difNLR and difORD function.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.