


Article Figures & Data
Figures
- Figure 1
Left to right: Webinar moderator was Kai-Uwe Lewandrowski, MD; Faculty who presented on the following topics were as follows: (1) Kenyu Ito, MD, Aichi Spine Institute, Japan, presented “Percutaneous Full Endoscopic Lumbar Interbody Fusion.” (2) Choll Kim, MD, PhD, Excel Spine Center UCSD, San Diego, California, USA, presented ”The Benefit of Simultaneous Multiportal Endoscopic Approaches and Articulating Instruments.” (3) Brian Kwon, MD, New England Baptist Hospital, Boston, Massachusetts, USA, presented “Biportal Endoscopic Treatment of Lumbar Facet Cysts.” (4) John Ongulade, DO, Department of Neurological Surgery, Washington University School of Medicine, St. Louis, Missouri, USA presented, “Managing Low-Grade Spondylolisthesis With Endoscopic Spine Surgery.”
- Figure 2
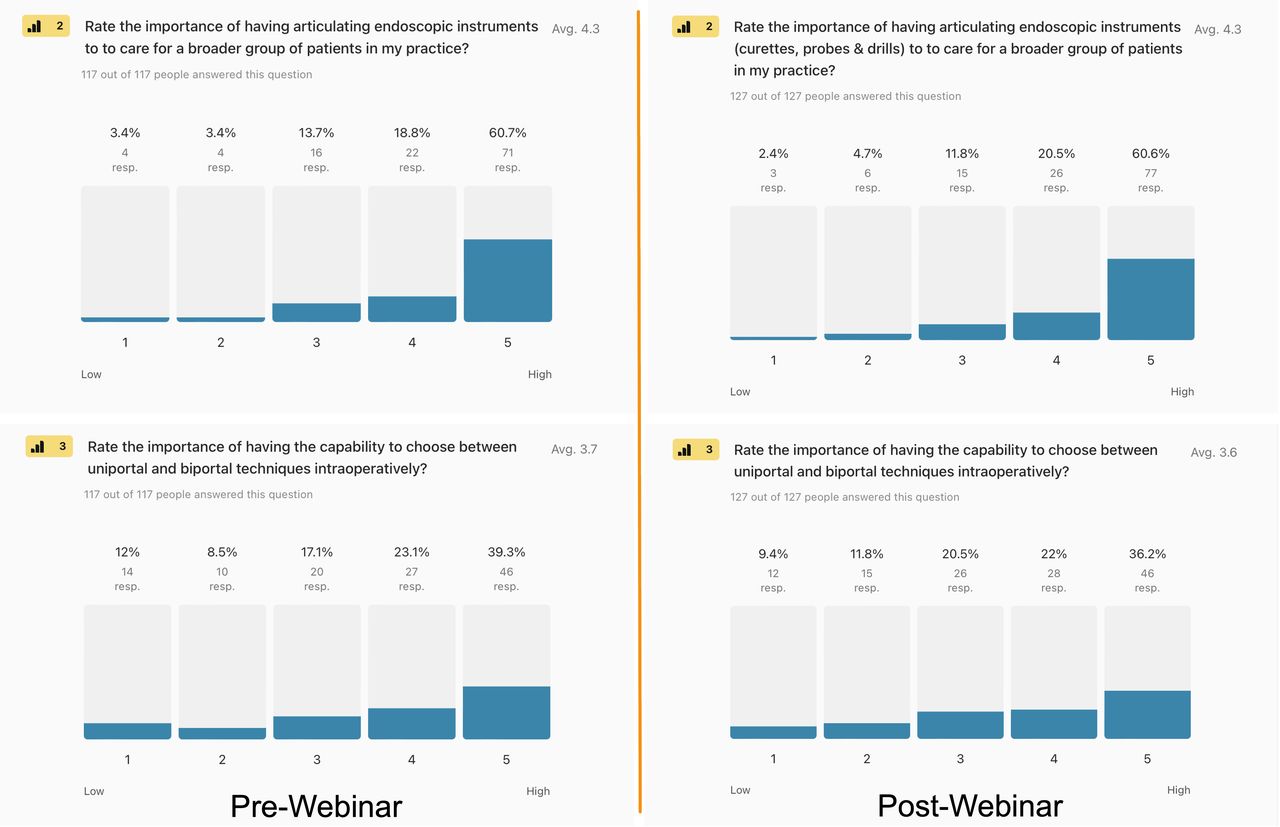
Pre- and postwebinar descriptive statistics of the level of importance of having articulating instruments to perform complex endoscopic decompression spine surgery: (2) 79.4% of surgeons gave it the highest endorsement selecting options 4 and 5 on a Likert scale from 1 to 5 before the webinar vs 81.4% after the webinar. (3) Similarly, 62.4% of prewebinar and 58.2% of postwebinar respondents thought that switching between uniportal and biportal techniques during the same operation was advantageous.
- Figure 3
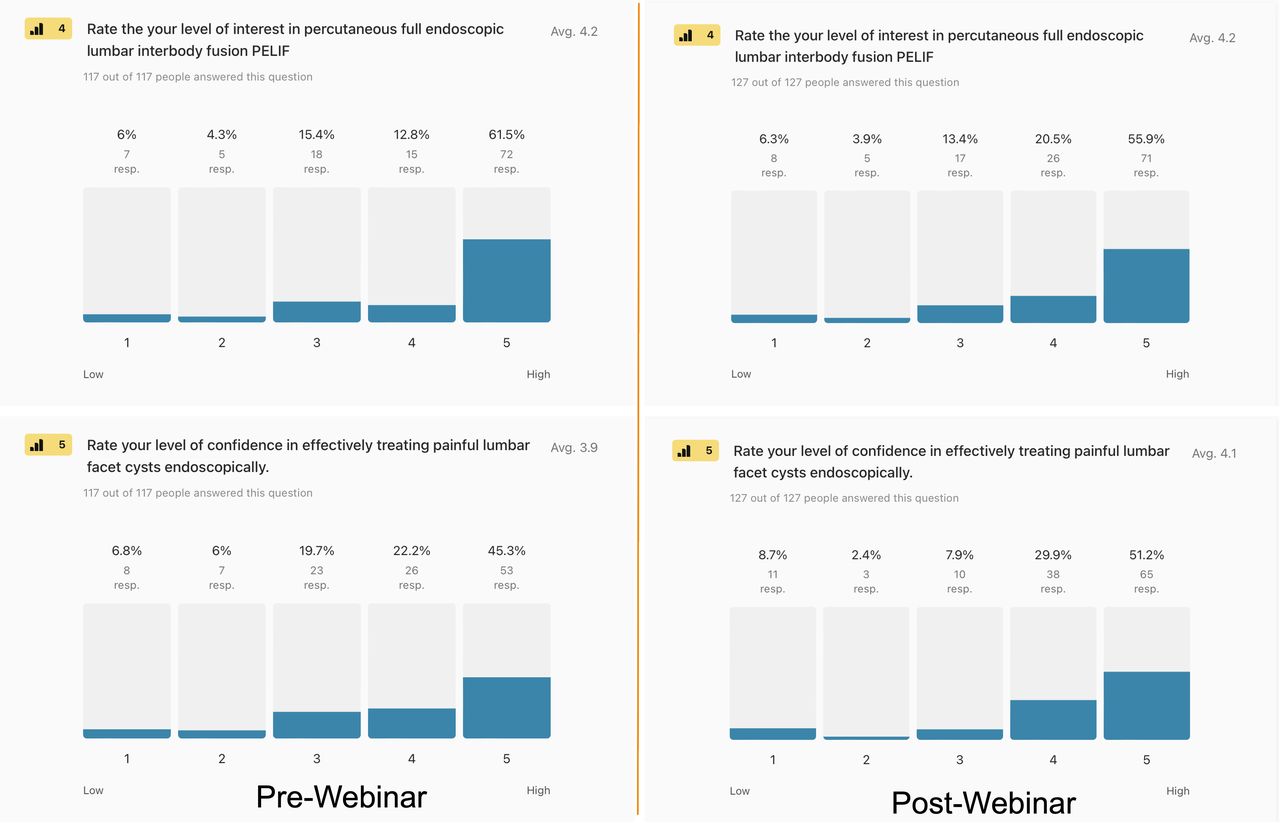
Pre- and postwebinar descriptive statistics of (4) the level of survey respondents’ interest in percutaneous endoscopic lumber interbody fusion (PELIF) at a high level (option 5) was 61.5% and 55.9%, and (5) confidence in effectively treating painful lumbar facet cysts with the endoscopic surgery platform were 45.3% and 51.2%, respectively.
- Figure 4
Pre- and postwebinar descriptive statistics as combined percentages of high-level endorsement options 4 and 5 of survey respondents’ (6) likelihood of recommending an endoscopic decompression for spinal stenosis-related symptoms in patients with low-grade lumbar spondylolisthesis (73.4% vs 70.1%), and (7) the confidence in transforaminal endoscopic surgery successfully treating posterolateral herniated disc (76.1% vs 73%), central HNP (60.6% vs 52.2%), lateral canal stenosis (57.7% vs 65.5%), central canal stenosis (32.9% vs 26.6%), facet cysts (49% vs 44.1%), and far-migrated HNP (49.5% vs 53.3%). Abbreviation: HNP, herniated nucleus pulposus.
- Figure 5
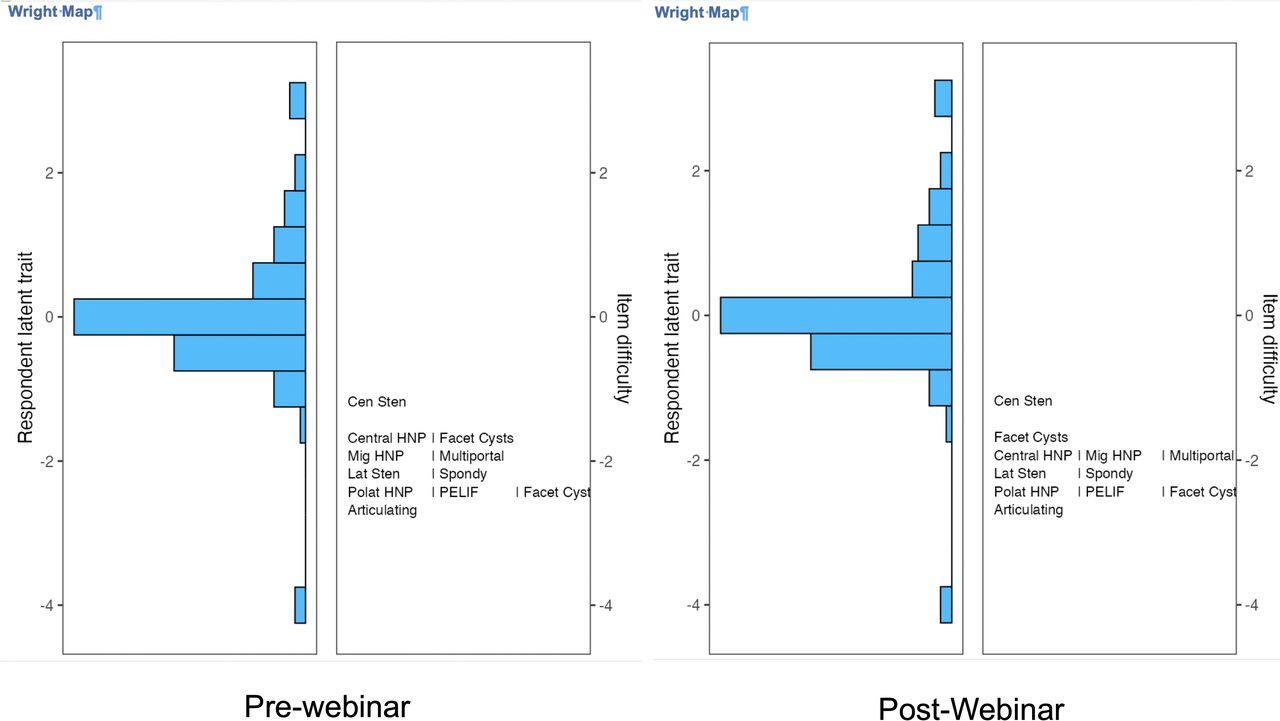
The item response theory polytomous Rasch partial agreement analysis was employed to obtain Wright plots of prewebinar (left panel) and postwebinar (right panel) survey responses regarding the importance of having articulating instruments, the ability to perform simultaneous uniportal transforaminal and biportal endoscopic surgery, the level of endorsement of percutaneous endoscopic lumbar interbody fusion (PELIF), and endoscopic treatment of low-grade spondylolisthesis (Spondy) lumbar facet joint cysts. In addition, surgeons were asked to rate the confidence in successfully treating central and lateral canal stenosis, central herniated nucleus pulposus (HNP), posterolateral HNP, migrated (Mig) HNP, and facet cysts with the transforaminal approach. On the left side of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability and intensity of partial agreement. The surgeons, represented by horizontal bars at the top, represented the highest level of endorsement. On the right of the Wright plot, the harder-to-agree-on items are listed at the top vs the easier-to-agree-on ones at the bottom. Directly across from 0, those surgeons had a 50% chance of endorsing a test item. There were 2 assessment gaps on the prewebinar survey and 1 on the postwebinar survey. The largest gap was created by disagreements on the need for articulating instruments. There was some redundancy between prewebinar test items, as shown by the same ranking for transforaminal treatments of various pathologies. However, endoscopic decompression of central stenosis was considered the hardest. Abbreviations: Can Sten, canal stenosis; Polat, posterolateral.
- Figure 6
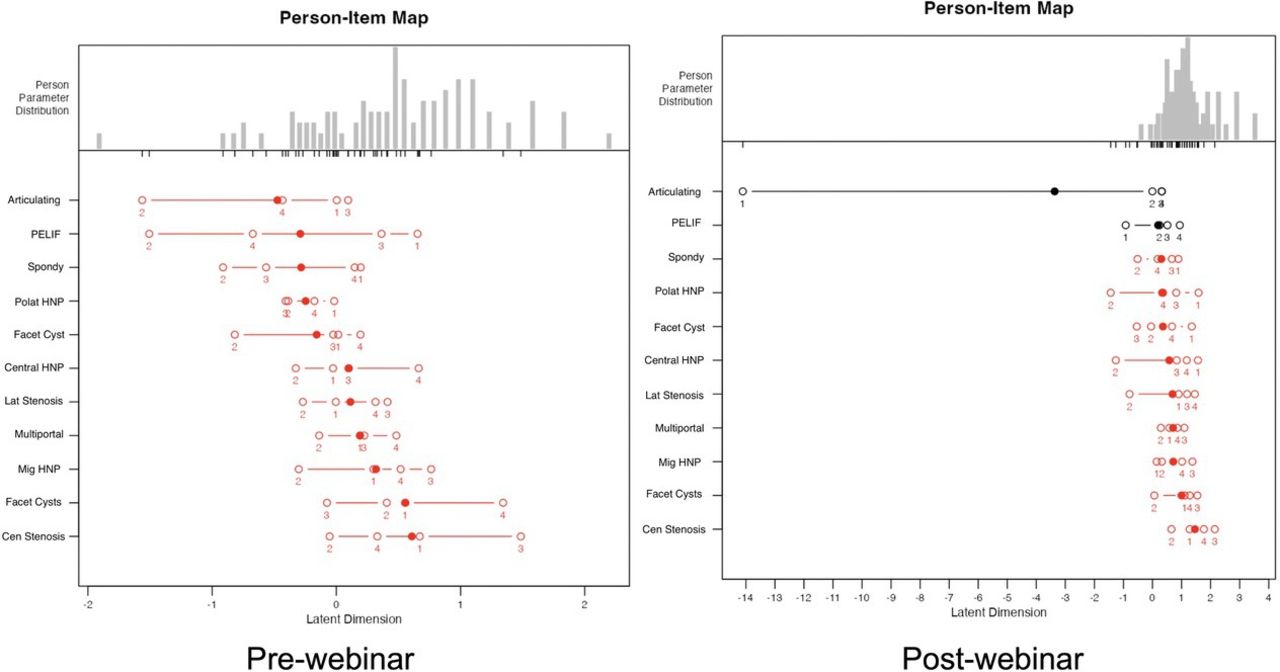
The person-item map of prewebinar (a) and postwebinar (b) survey responses show the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x-axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Disordered items are shown in red, and ordered ones are in black. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum, suggesting a poor fit to the Rasch model without any statistically significant difference between the observed values and the values predicted by the model. In comparison to descriptive statistics (Figures 1–3), the most high-intensity items in the prewebinar survey with median log-odds greater than 0 were the pathologies commonly treated with the transforaminal approach, including facet cysts, migrated disc herniations, and lateral and central canal stenosis. The multiportal approach strategy also received a higher than 0 median log odd. Posterolateral disc herniations, percutaneous endoscopic lumbar interbody fusion with endoscopically placed cages and posterior supplemental pedicle screw fixation (PELIF), low-grade spondylolisthesis (Spondy), and the need for articulating instruments during endoscopic treatment of more complex spinal pathologies, and UBE facet joint cyst treatment received log-odds of less than 0 suggesting these items were low intensity. All prewebinar test items had disorderly log odds. The postwebinar analysis showed an endorsement boost for all test items with increased median log odds above 0 except “articulating instruments,” highlighting the high impact of the webinar-based education. However, postwebinar analysis showed orderly item response configuration for articulating instruments and endoscopic treatment of Spondy. Abbreviations: Cen, central; HNP, herniated nucleus pulposus; Lat, lateral; Mig, migrated; Polat, posterolateral; Sten, stenosis.
- Figure 7
Item characteristic curves generated from prewebinar survey responses to multiportal treatment for complex lumbar spinal pathologies as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.0236 and a P value of 0.878 (Table 3) compared with postwebinar DIF detection of 1.607 and a P value of 0.448 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.
- Figure 8
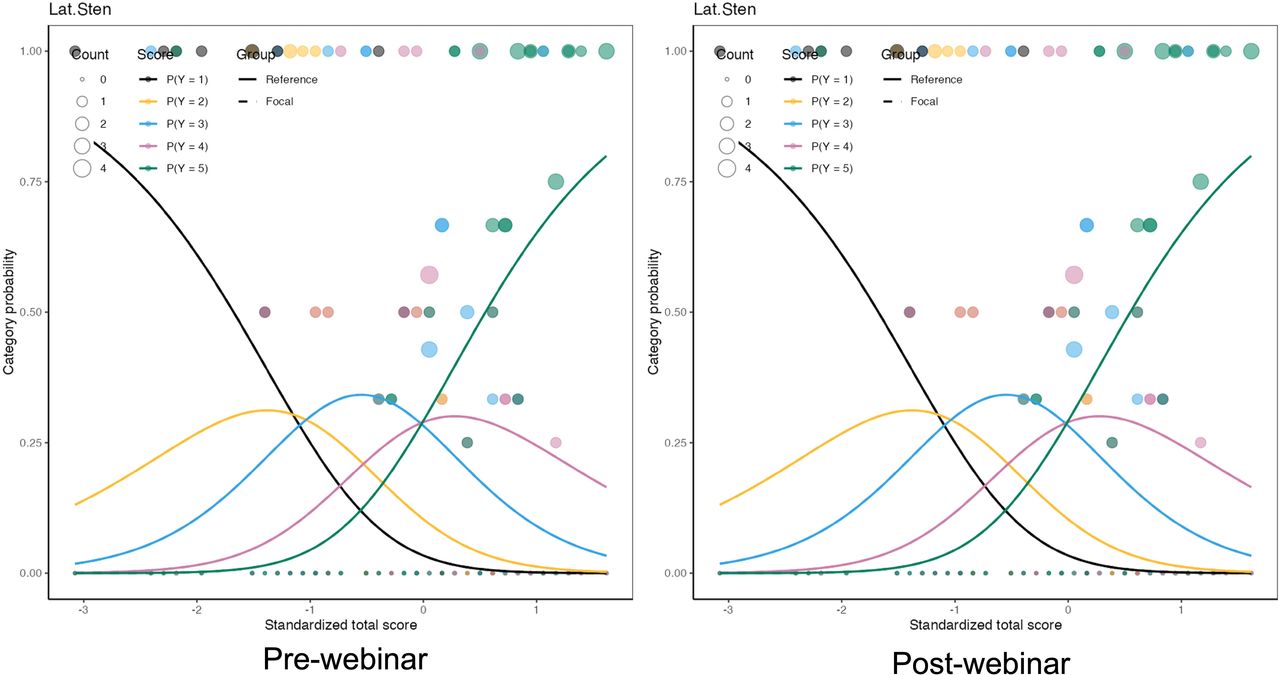
Item characteristic curves generated from prewebinar survey responses “Lateral Canal Stenosis” (Lat. Sten.) as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.3394 and a P value of 0.560 (Table 3) compared with postwebinar DIF detection of 0.198 and a P value of 0.906 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.
- Figure 9
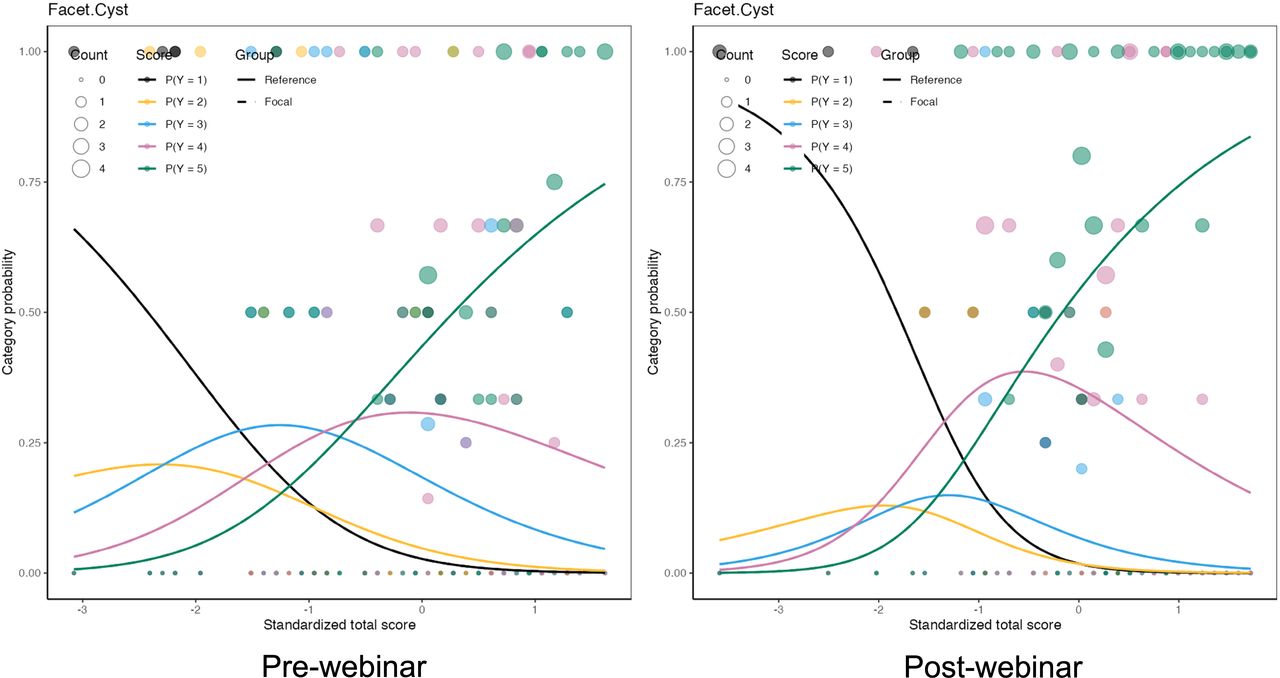
Item characteristic curves generated from prewebinar survey responses unilateral biportal endoscopic facet cyst as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.8608 and a P value of 0.354 (Table 3) compared with postwebinar DIF detection of 1.284 and a P value of 0.526 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.
- Figure 10
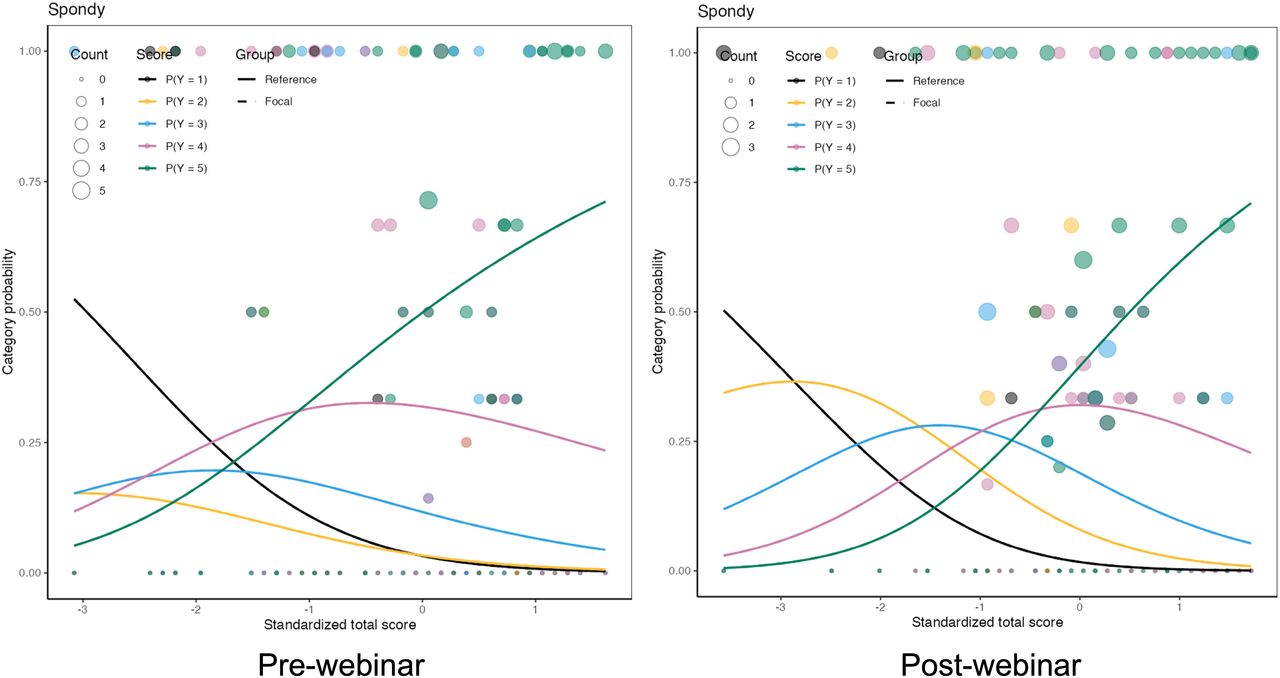
Item characteristic curves generated from prewebinar survey responses regarding Spondy (low grade spondylolisthesis) as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.6184 and a P value of 0.432 (Table 3) compared with postwebinar DIF detection of 8.130 and a P value of 0.017 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.
- Figure 11
The item characteristic curves generated from prewebinar survey responses regarding articulating instruments as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.5462 and a P value of 0.460 (Table 3) compared with postwebinar DIF detection of 11.168 and a P value of 0.004 (Table 4), suggesting significant bias in the merit assessment of “Articulating Instruments” between orthopedic surgeons and neurosurgeons with disorderly responses in the item’s midsection while maintaining good discriminatory fusion between low- and high-level endorsement.
- Figure 12
The item characteristic curves generated from prewebinar survey responses regarding percutaneous endoscopic lumbar interbody fusion (PELIF) as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.8548 and a P value of 0.355 (Table 3) compared with postwebinar DIF detection of 15.485 and a P value of <0.001 (Table 4), suggesting significant bias in the merit assessment of PELIF between orthopedic surgeons and neurosurgeons with disorderly responses in the item’s midsection while maintaining a good discriminatory function between high and low endorsement.












Tables
- Table 1
Prewebinar survey model fit analysis and item statistics of the rating scale model.
Procedure Measure SE Measure Infita Outfitb Transforaminal posterolateral HNP −2.44 0.1126 1.207 1.576 Transforaminal central HNP −1.77 0.0904 1.480 1.752 Transforaminal lateral stenosis −2.35 0.1081 1.105 1.036 UBE treatment of facet cysts −2.12 0.0994 0.995 1.035 Transforaminal migrated HNP −2.30 0.1061 1.197 1.302 PELIF −2.28 0.1052 0.881 0.785 Transforaminal facet cyst treatment −1.85 0.0919 0.786 0.747 Low-grade spondylolisthesis −1.82 0.0914 0.883 0.868 Transforaminal central stenosis −1.31 0.0865 0.854 0.855 Multiportal technique −1.46 0.0868 0.740 0.684 Articulating instruments −1.62 0.0881 0.873 0.905 Scale Person Reliability MADaQ3 P 0.776 0.212 <0.001 - Table 2
Postwebinar survey model fit analysis and item statistics of the rating scale model.
Procedure Measure SE Measure Infita Outfitb Transforaminal posterolateral HNP −2.39 0.1059 0.939 0.881 Transforaminal central HNP −1.81 0.0902 0.930 0.991 Transforaminal lateral stenosis −2.09 0.0960 0.777 0.713 UBE treatment of facet cysts −1.58 0.0879 0.853 0.820 Transforaminal migrated HNP −1.91 0.0919 0.725 0.762 PELIF −2.45 0.1082 1.375 1.329 Transforaminal facet cyst treatment −2.49 0.1097 1.144 1.049 Low-grade spondylolisthesis −2.21 0.0996 1.069 1.224 Transforaminal central stenosis −1.14 0.0890 0.819 0.800 Multiportal technique −1.88 0.0914 1.448 1.489 Articulating instruments −2.63 0.1161 1.030 1.033 Scale Person Reliability MADaQ3 P 0.811 0.180 <0.001 - Table 3
Prewebinar survey DIF detection procedure for ordinal data based on adjacent category logit model.
Survey Item Statistic P Adjusted P Articulating instruments 0.5462 0.460 0.723 Multiportal technique 0.0236 0.878 0.878 PELIF 0.8548 0.355 0.723 Facet cyst 0.8608 0.354 0.723 Low-grade spondylolisthesis 0.6184 0.432 0.723 Transforaminal posterolateral HNP 0.9112 0.340 0.723 Transforaminal central HNP 1.6761 0.195 0.723 Transforaminal lateral stenosis 0.3394 0.560 0.770 Transforaminal central stenosis 0.0741 0.785 0.878 Transforaminal facet cyst treatment 0.0458 0.831 0.878 Transforaminal migrated HNP 1.0136 0.314 0.723 Abbreviations: DIF, differential item functioning; HNP, herniated nucleus pulposus; PELIF, percutaneous endoscopic lumbar interbody fusion.
Note. DIF likelihood ratio statistics are estimated by using difNLR and difORD functions. Adjusted P values calculated by the likelihood ratio test using multiple comparisons.
- Table 4
Postwebinar survey DIF detection procedure for ordinal data based on adjacent category logit model.
Survey Item Statistic P Adjusted P Articulating instruments 11.168 0.004 0.021 Multiportal technique 1.607 0.448 0.616 PELIF 15.485 <0.001 0.005 Facet cyst 1.284 0.526 0.643 Low-grade spondylolisthesis 8.130 0.017 0.063 Transforaminal posterolateral HNP 0.836 0.658 0.724 Transforaminal central HNP 3.209 0.201 0.442 Transforaminal lateral stenosis 0.198 0.906 0.906 Transforaminal central stenosis 1.647 0.439 0.616 Transforaminal facet cyst treatment 3.901 0.142 0.391 Transforaminal migrated HNP 2.635 0.268 0.491 Abbreviations: DIF, differential item functioning; HNP, herniated nucleus pulposus; PELIF, percutaneous endoscopic lumbar interbody fusion.
Note. DIF likelihood ratio statistics are estimated by using difNLR and difORD functions. Adjusted P values calculated by the likelihood ratio test using multiple comparison.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.