


Abstract
Background The increase in total disc replacement procedures performed over the last 5 years has increased the occurrence of patients presenting with postoperative iatrogenic deformity requiring revision surgery. Proposed salvage treatments include device retrieval followed by anterior lumbar interbody fusion or posterior fusion. We propose a novel approach for the correction of disc tilt after total disc replacement using a posterior dynamic stabilization system.
Methods Pedicle screws can be inserted either in an open manner or percutaneously by standard techniques under fluoroscopy. The collapsed side is expanded, and the convex side is compressed. Universal spacers are placed bilaterally, with the spacer on the collapsed side being taller by 6 mm. Cords are threaded through the spacers and pulled into place with the tensioning instrument. Extra tension is applied to the convex side, and the wound is closed by standard techniques.
Results Three patients presenting with tilted total disc replacement devices underwent corrective surgery with posterior dynamic stabilization. Radiographs confirmed correction of deformity in all cases.
Conclusions/Level of Evidence This technical note presents a novel indication for posterior dynamic stabilization and describes its surgical application to the correction of disc tilt after total disc replacement. This is level V evidence.
The number of total disc replacement (TDR) procedures performed in the United States has rapidly increased since the Food and Drug Administration's first TDR device approval in October 2004.1–3 TDR procedures compromise the anterior longitudinal ligament, annulus fibrosis, and sometimes, the posterior longitudinal ligament. This may result in rotational instability and disc tilting, especially in the lumbar spine, which is very dependent on these structures for stability.4–6
The increasing frequency of patients presenting with iatrogenic deformity is yielding more revision surgeries.5 Currently proposed revision techniques include TDR device retrieval followed by anterior lumbar interbody fusion or posterolateral fusion.4 Although some patients are opposed to these options, motion-preserving salvage procedures after TDR are scarcely mentioned in the literature.7, 8 In this technical note, however, we present a novel, potentially motion-preserving technique for the correction of disc tilt after TDR using posterior dynamic stabilization (PDS).
Materials and methods
Patient positioning and surgical exposure
The patient was placed prone on a Jackson spine table, and care was taken to avoid any pressure on the abdominal cavity to avoid excessive bleeding. The hip was placed in slight extension to maximize lumbar lordosis. Fluoroscopy was used to identify the surgico-anatomic landmarks and to define the site of incision. The pedicles were then approached through either a single midline incision or 2 paraspinal incisions. For the patient who preferred a mini-open paraspinal approach, biplane fluoroscopy was used. Electromyography was used for neurologic monitoring.
The midline incision was made over the spinous processes of the vertebrae such that the incision was 1 segment longer proximally and distally than the planned operative level. The midline incision is used if bone decompression is indicated. We prefer the paraspinal approach, which involves 2 surgical incisions about 3.5 cm lateral from the midline (L4-S1).9 The dorsal fascia is then opened, and entry to the pedicles is gained through the plane between the multifidus and longissimus muscles.10
Pedicle screw placement
The pedicle screws were inserted lateral to the facets by standard techniques. We used the cephalad tip of the accessory process as an entry point. The screws were placed close to the endplate and directed inward to maximize purchase, and we used the largest screws possible to heighten stability. All procedures were performed under fluoroscopic guidance. In the mini-open approach, cannulated screws were inserted over guidewires by use of biplane fluoroscopy. We also electrodiagnostically confirmed the correct placement of the pedicle screws.
Placement of universal spacers and cord
We first addressed the collapsed side of the TDR device and then proceeded with installation of a Dynesys system (Zimmer Spine, Warsaw, Indiana). We placed the pedicle distance gauge between screw heads and applied the maximum distraction force allowed by the gauge. The distance on the collapsed side was then measured. We added 3 mm to this distance to determine universal spacer height for the collapsed side, whereas 3 mm was subtracted to determine universal spacer height for the contralateral side. The collapsed-side universal spacer was threaded with polyethylene-terephthalate cord, and the tensioning instrument was used to pull the device into place. The same procedure was repeated on the contralateral side, although more tension was applied for compression.
Closure
The hardware and retractors were removed, and the fascia and skin were closed by use of standard techniques.
Results
Case 1
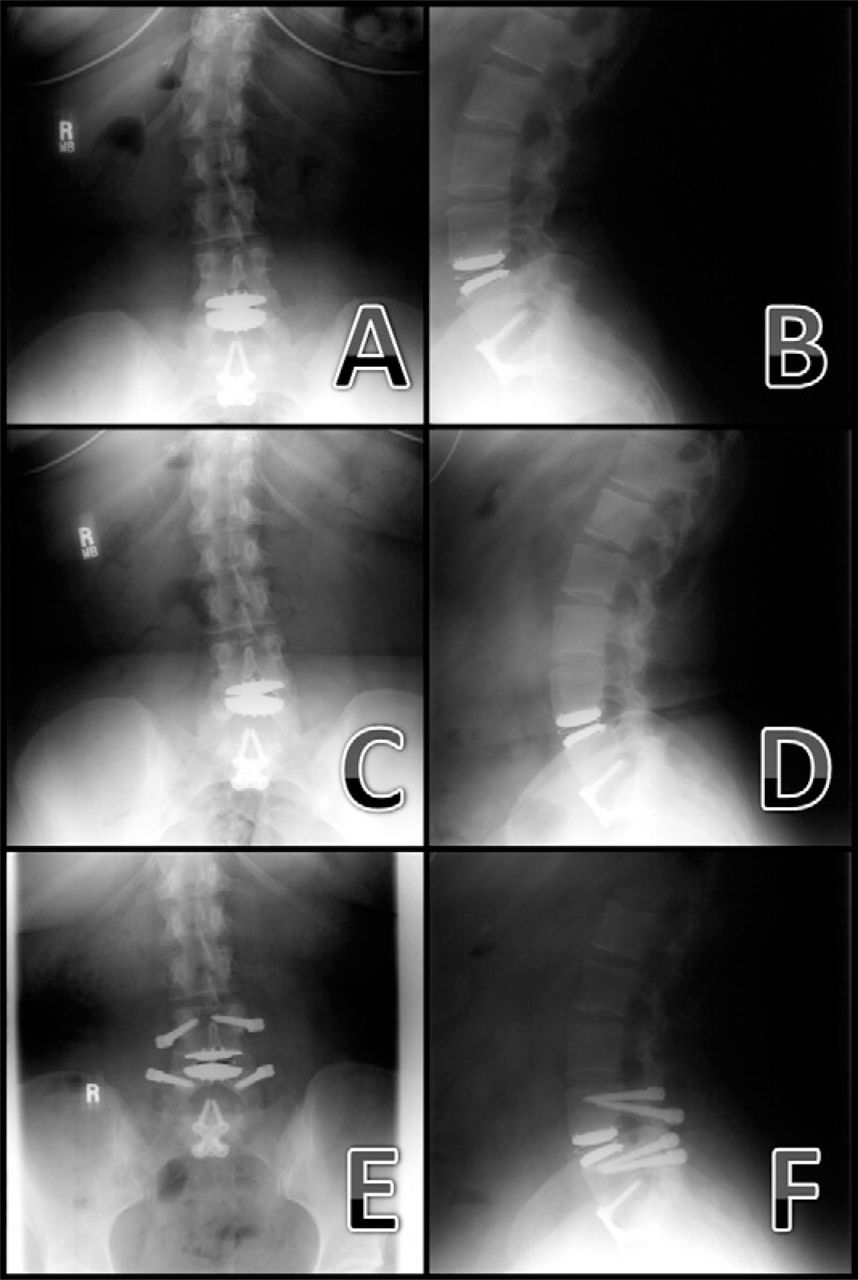
Hybrid surgery with L4-5 TDR and L5-S1 anterior lumbar interbody fusion was performed in a 35-year-old woman with a body mass index (BMI) of 37 kg/m2 (height, 188 cm [6 ft 2 in]; weight, 132 kg [290 lb]). Surgical indications included severe back and leg pain that compromised quality of life. The initial TDR device location was good (Figs. 1A, B), and pain and function improved. Piriformis and greater trochanter pain persisted, which were pre-existent to the surgery. The patient presented 6 months after the TDR procedure with right disc tilt and progressive back and right leg pain as depicted by a visual analog scale (VAS) score of 70 and Oswestry Disability Index (ODI) score of 48 (Figs. 1C, D). Multiple epidural injections were performed for both diagnostic and therapeutic purposes without long-term relief.

Anterior-posterior and lateral standing radiographs in case 1 showing the TDR device in its original position (A and B, respectively); the tilted TDR device (C and D, respectively); and the TDR device after correction with PDS (E and F, respectively).
A Dynesys PDS system was used to correct the disc tilt (Figs. 1E, F). A superficial wound infection occurred postoperatively that resolved with antibiotic treatment. Pain and function improved, and the hardware location was maintained at the 1-year follow-up. Quality of life remains good as indicated by the patient's most recent VAS score of 30 and ODI score of 38.
Case 2
L4-5 TDR was performed in a 30-year-old man with a BMI of 22 kg/m2 (height, 185 cm [6 ft 1 in]; weight, 77 kg [170 lb]). Indications included L4-5 disc degeneration causing pain interfering with quality of life that did not resolve with nonsurgical treatments (VAS score, 70; ODI score, 72). There was significant pain reduction for 8 months, at which point the patient presented with disc tilt on the right side associated with progressive right leg pain (Figs. 2A, B). The patient's VAS score was 80, and ODI score was 34. Multiple injections were performed for both diagnostic and therapeutic purposes. A computed tomography myelogram was obtained to investigate the patient's symptoms. Subsequently, a Dynesys PDS system was used to correct the disc tilt, and there was significant pain reduction postoperatively (Figs. 2C, D). The patient's VAS score was reduced to 40. Follow-up visits over the next 4 years showed that hardware location was maintained and quality of life was good (Figs. 2E, F). The patient returned to work as a custodian, although mild back pain and mild right leg dysesthesia persisted.

Anterior-posterior and lateral standing radiographs in case 2 showing the tilted TDR device (A and B, respectively); the TDR device after correction with PDS (C and D, respectively); and the TDR device 3 years after correction with PDS (E and F, respectively).
Case 3
Hybrid surgery with L4-5 TDR and L5-S1 fusion was performed in a 45-year-old woman with a BMI of 37 kg/m2 (height, 175 cm [5 ft 9 in]; weight, 113 kg [250 lb]) (Figs. 3A, B). Surgical indications included severe back and leg pain that compromised quality of life. The patient did reasonably well after surgery. Approximately 7 months postoperatively, the patient received injections bilaterally at the sacroiliac joints and at the left L4-5 facet joint; however, she reported that these worsened the pain. Radiographs showed mild facet arthropathy and slight tilting of the disc. Thirty months postoperatively, the patient received a spinal stimulator that yielded limited improvement. Back pain with leg pain mainly of the L5 distribution progressively increased over the third postoperative year.

Anterior-posterior and lateral standing radiographs in case 3 showing the TDR device in its original position (A and B, respectively); intraoperative anterior-posterior and lateral radiographs showing disc tilt and the mini-open surgical technique (C and D, respectively); and anterior-posterior and lateral standing radiographs showing the TDR device after correction with PDS (E and F, respectively).
Four years after initial surgery, right leg pain worsened, as did deformity. A computed tomography myelogram was obtained to investigate the patient's symptoms, and administration of an epidural was attempted unsuccessfully. Facet injection and radiofrequency ablation yielded minimal relief. Revision surgery with PDS was then discussed and performed by a mini-open technique (Figs. 3C, D). TDR device tilt was successfully corrected, and the right leg pain resolved after surgery (Figs. 3E, F). Left leg pain that existed before surgery remained postoperatively.
Discussion
PDS systems have become popular for a variety of spinal procedures; however, the various indications for PDS are still being investigated.11–15 Conjunctional application of TDR and PDS has been previously advocated.11 Here, we provide a novel indication for the use of a PDS system in the potentially motion-preserving correction of TDR tilt. The described technique was used to correct TDR tilt in 3 patients. Both patients 1 and 3 had BMIs of 37 kg/m2. As such, the mini-open approach used in patient 3 provided for less blood loss and easier access. Risks associated with this technique are the same as those associated with other posterior spinal approaches.16 It is advantageous compared with anterior salvage approaches because it is less complex overall and it avoids great vessel manipulation. Arthrosis-related complications are also avoided. Three- to four-year follow-up records for our first 2 patients show favorable outcomes with regard to VAS scores, ODI scores, and hardware location. The third patient was a recent case, so postoperative VAS and ODI scores were unavailable.
We selected the Dynesys system for TDR tilt correction among various modern PDS systems including other pedicle screw– based systems, interspinous spacers, and facet replacement systems.13, 15, 17–19 Currently, in the United States, facet replacement systems and some interspinous spacers are only available in Food and Drug Administration–monitored Investigational Device Exemption studies. Because all of our patients had prior surgery, they were not eligible for treatment within these studies. In addition, interspinous spacers are not adequate for the correction of TDR tilt. A pedicle screw– based system is needed to correct TDR tilt by expanding the collapsed side of the vertebral level relative to the contralateral side. Of the pedicle screw– based systems available, the Dynesys system was selected because it had the longest track record and because it allowed us to both expand the collapsed side and compress the contralateral side through manipulation of universal spacer height and cord tension.11, 13
Conclusion
This technical note presents a novel indication for PDS and describes a potentially motion-preserving means of correcting disc tilt after TDR.
Acknowledgments
The authors thank Elisabeth Clarke, Kathleen Elias, and Mary Kolb for all of their administrative help.
- © 2011 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.