


Article Figures & Data
Figures
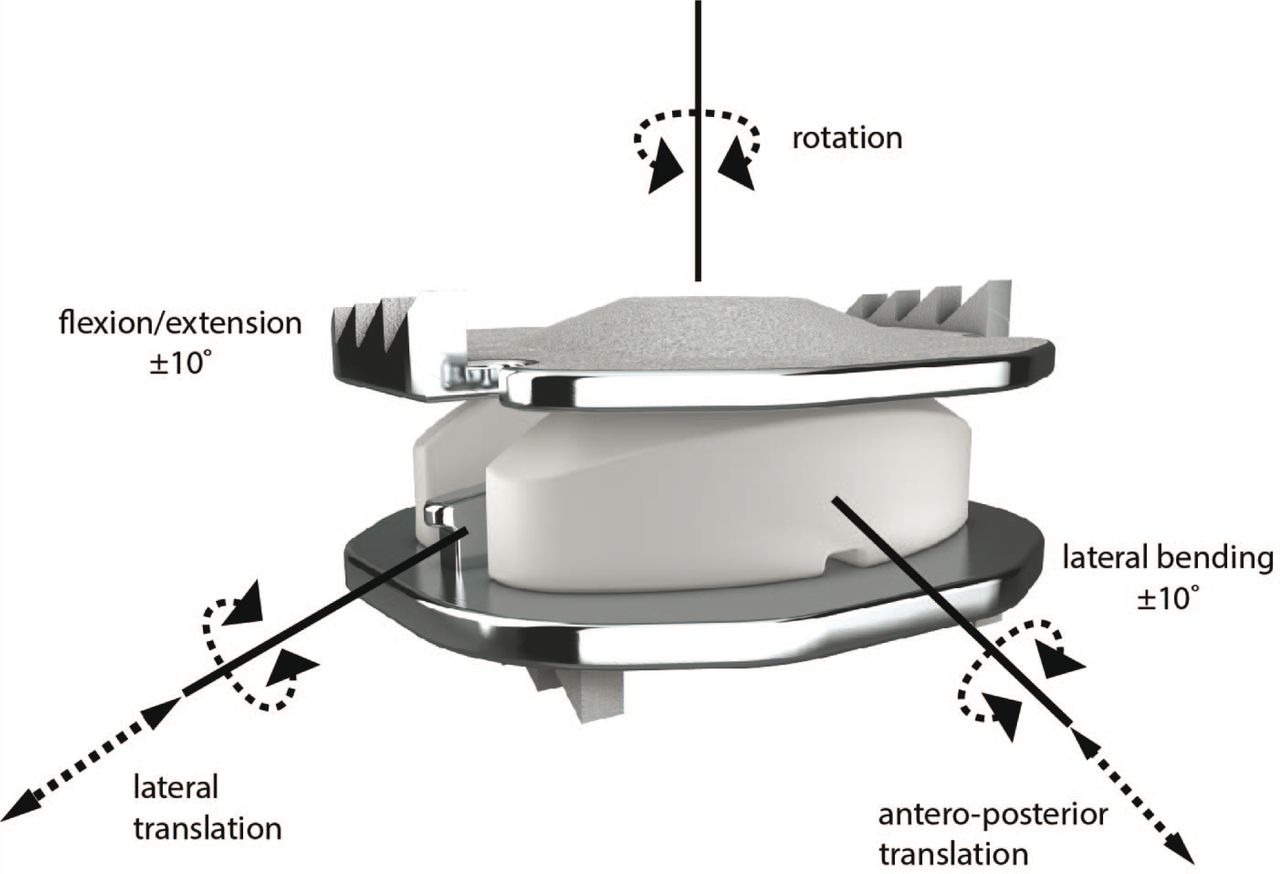
- Fig. 1
Mobi-C Artificial Cervical Disc (LDR Medical; Troyes, France). Allows for five independent degrees of freedom.
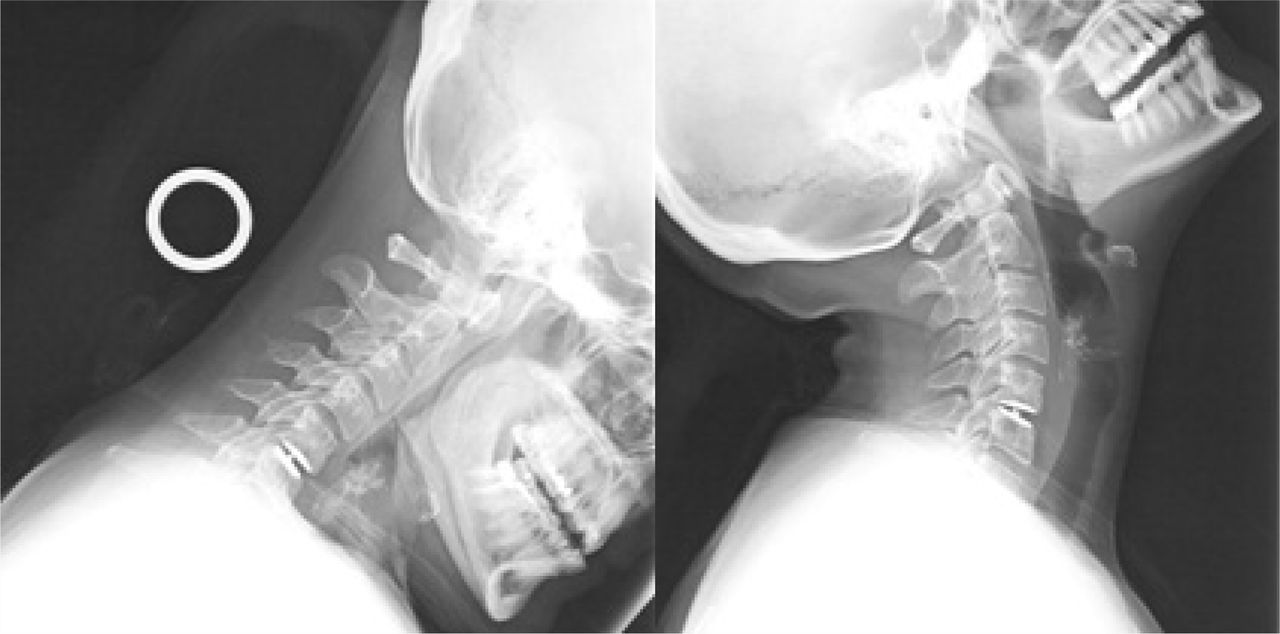
- Fig. 2
TDR device in proper placement. Lateral flexion and extension x-rays of the TDR at 24 months.
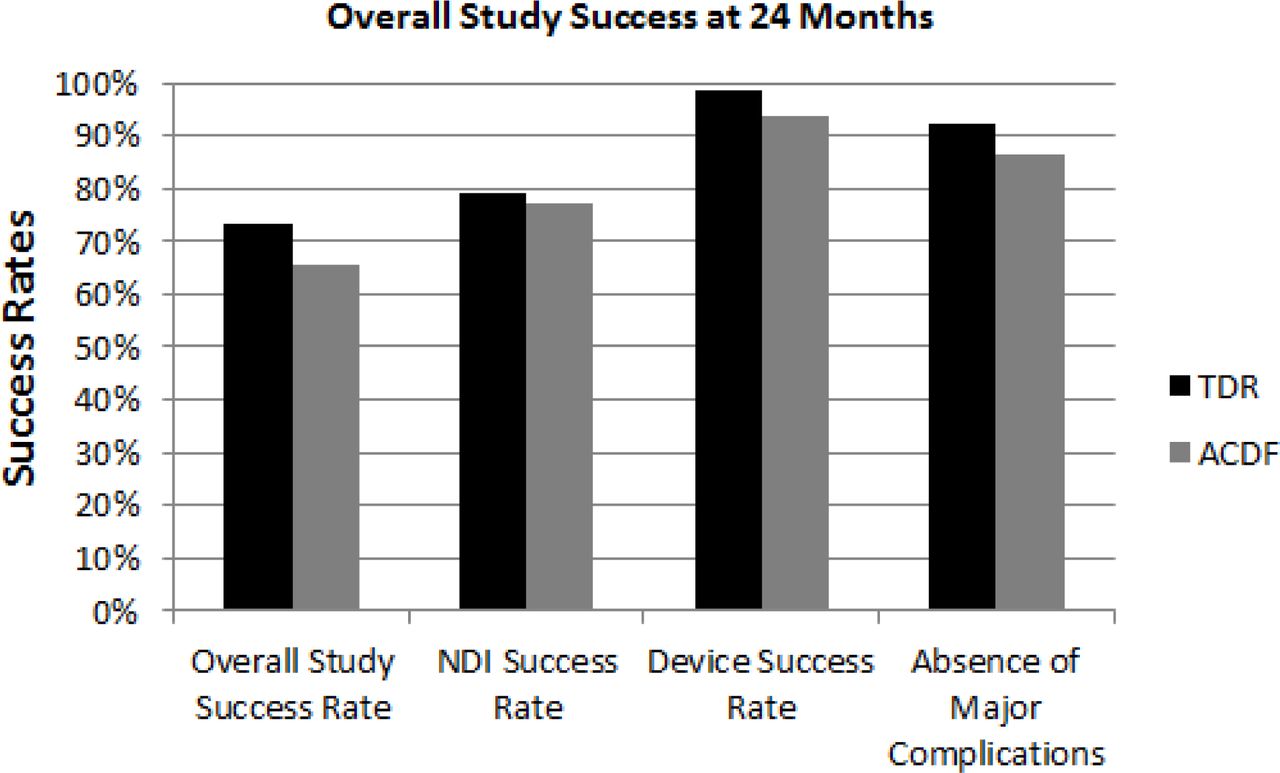
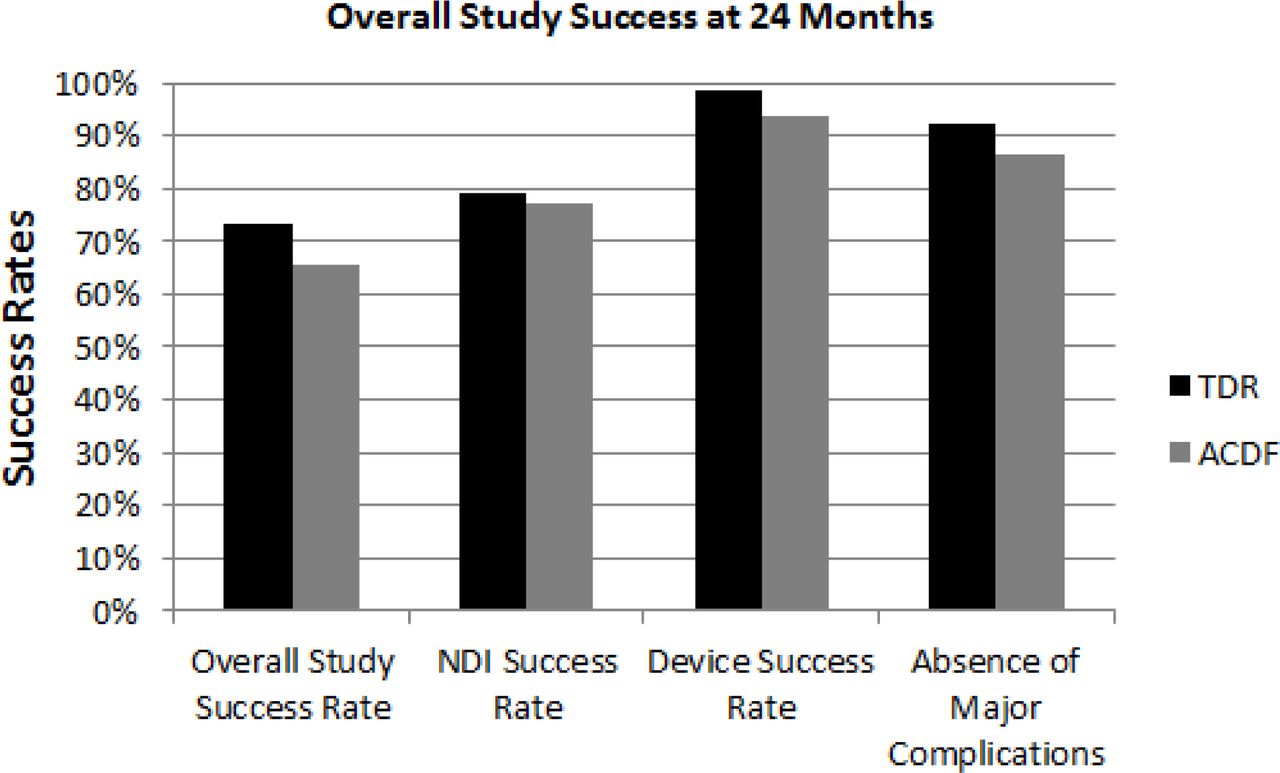
- Fig. 3
Overall Study Success at 24 Months. Bar graph showing over all clinical success rate at 24 months. Also shown are the success rates at 24 months of the components of the composite endpoint: NDI success rate, Device success rate (no need for subsequent surgeries, and the percentage of patients who had no major complications.
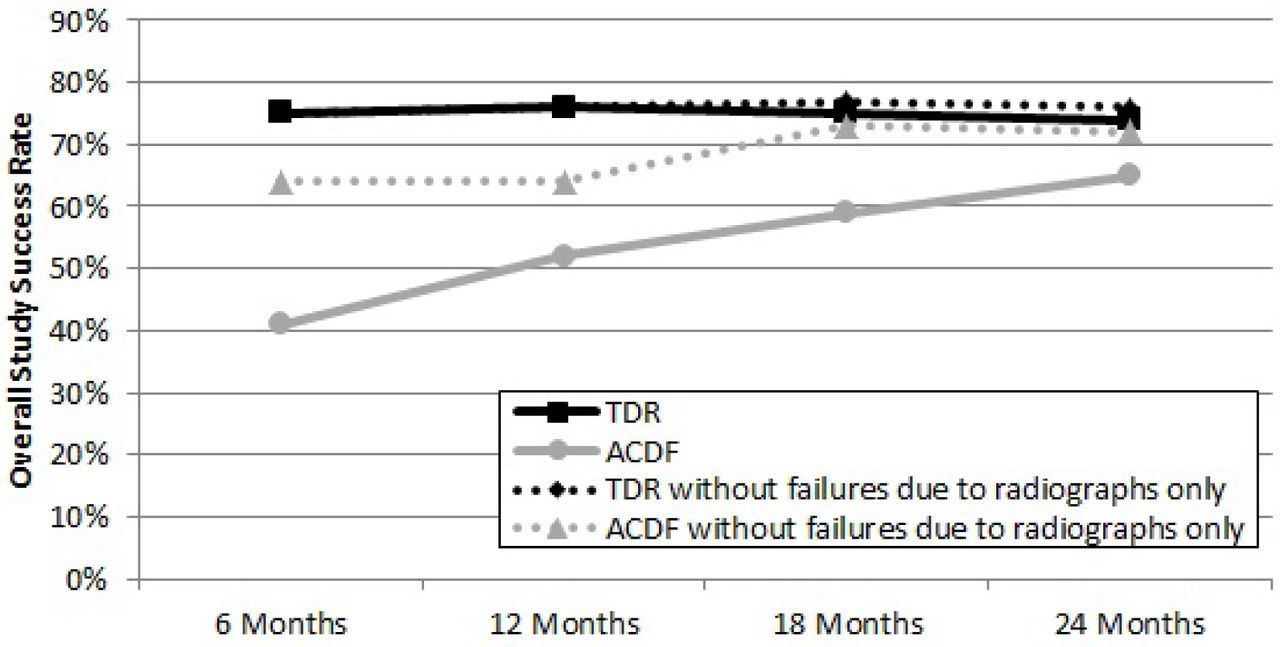
- Fig. 4
Overall Study Success Rates by Time point. Success rates are shown for both TDR group and ACDF group both with and without failures due only to radiographic major complications. Non-inferiority is demonstrated at each time point for both TDR compared to ACDF in both cases.
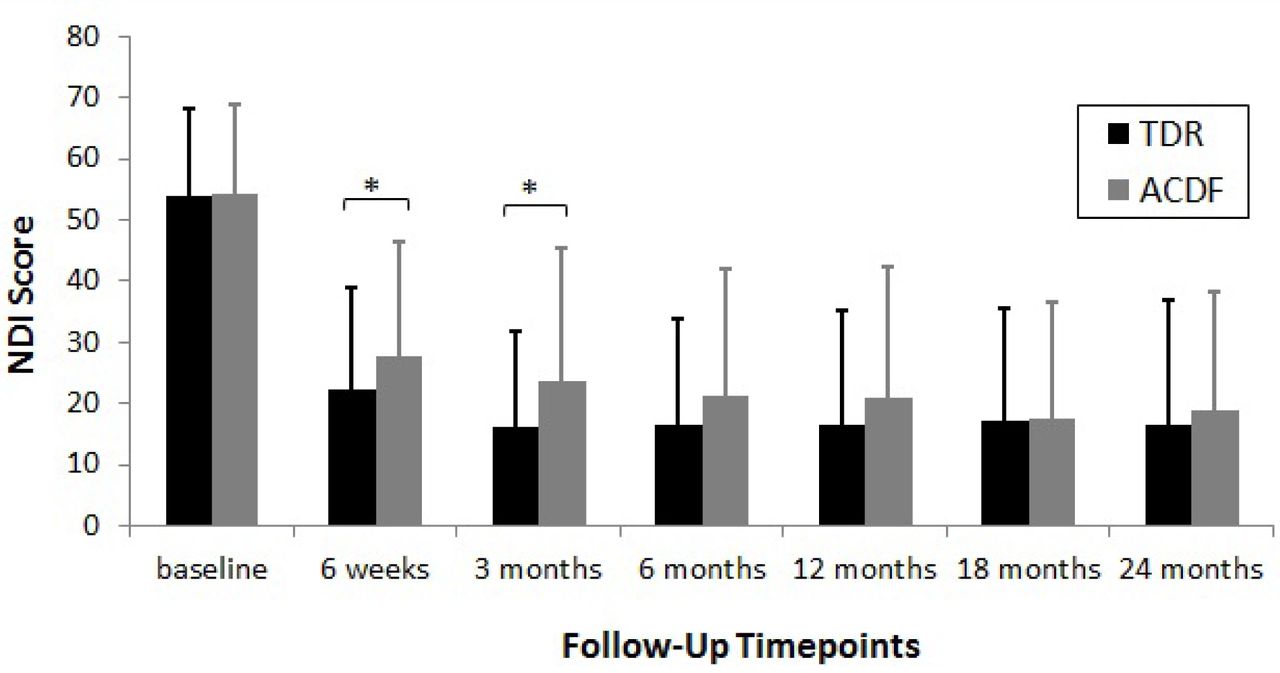
- Fig. 5
Mean NDI Score by Time point. NDI scores were collected at each visit. Error bars represent standard deviations. NDI scores for both treatment groups were significantly different from baseline at all time points (p < 0.05) * Denotes significant difference determined using unpaired t-test to compare the change from baseline between the two treatments (p < 0.05).
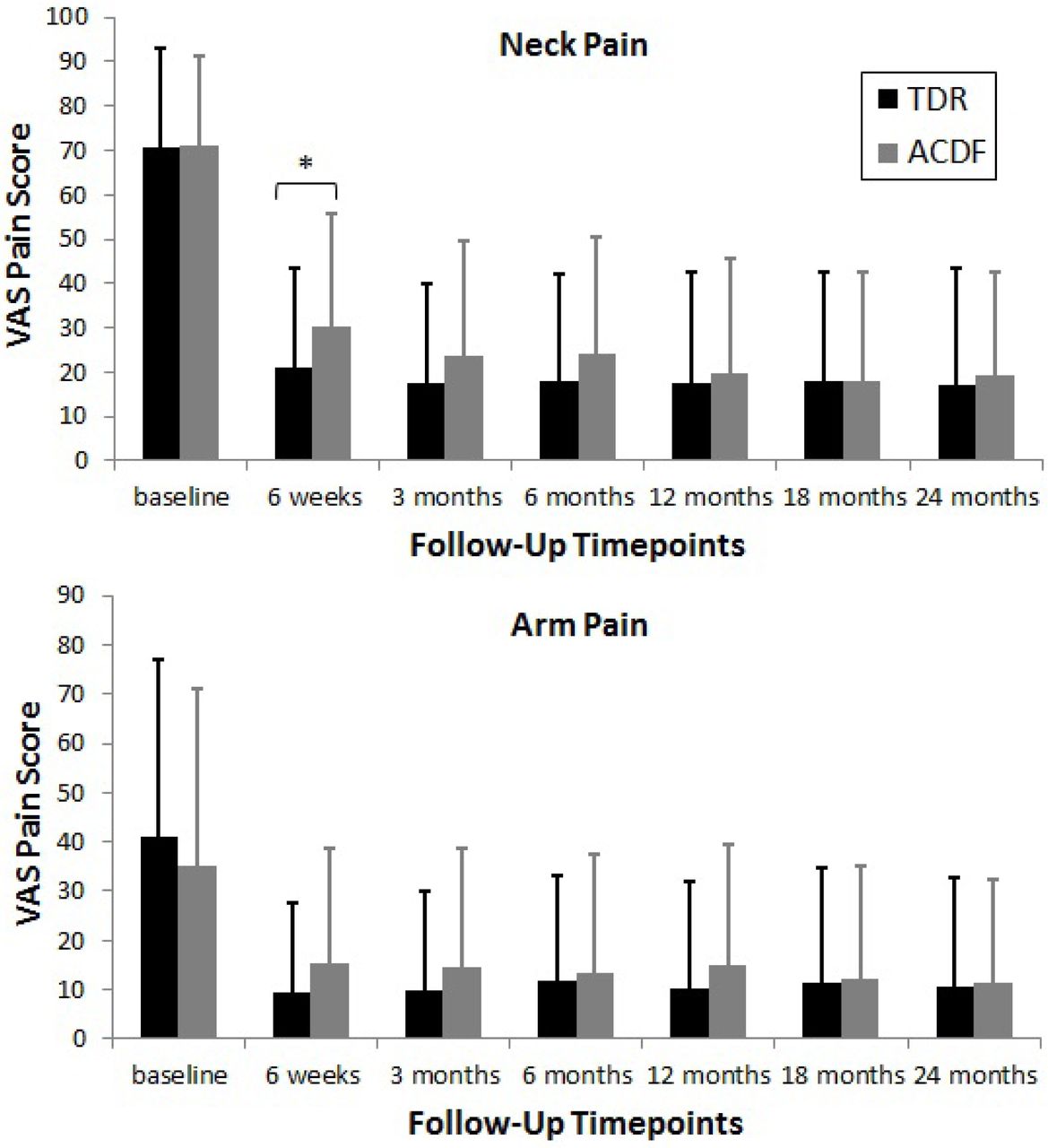
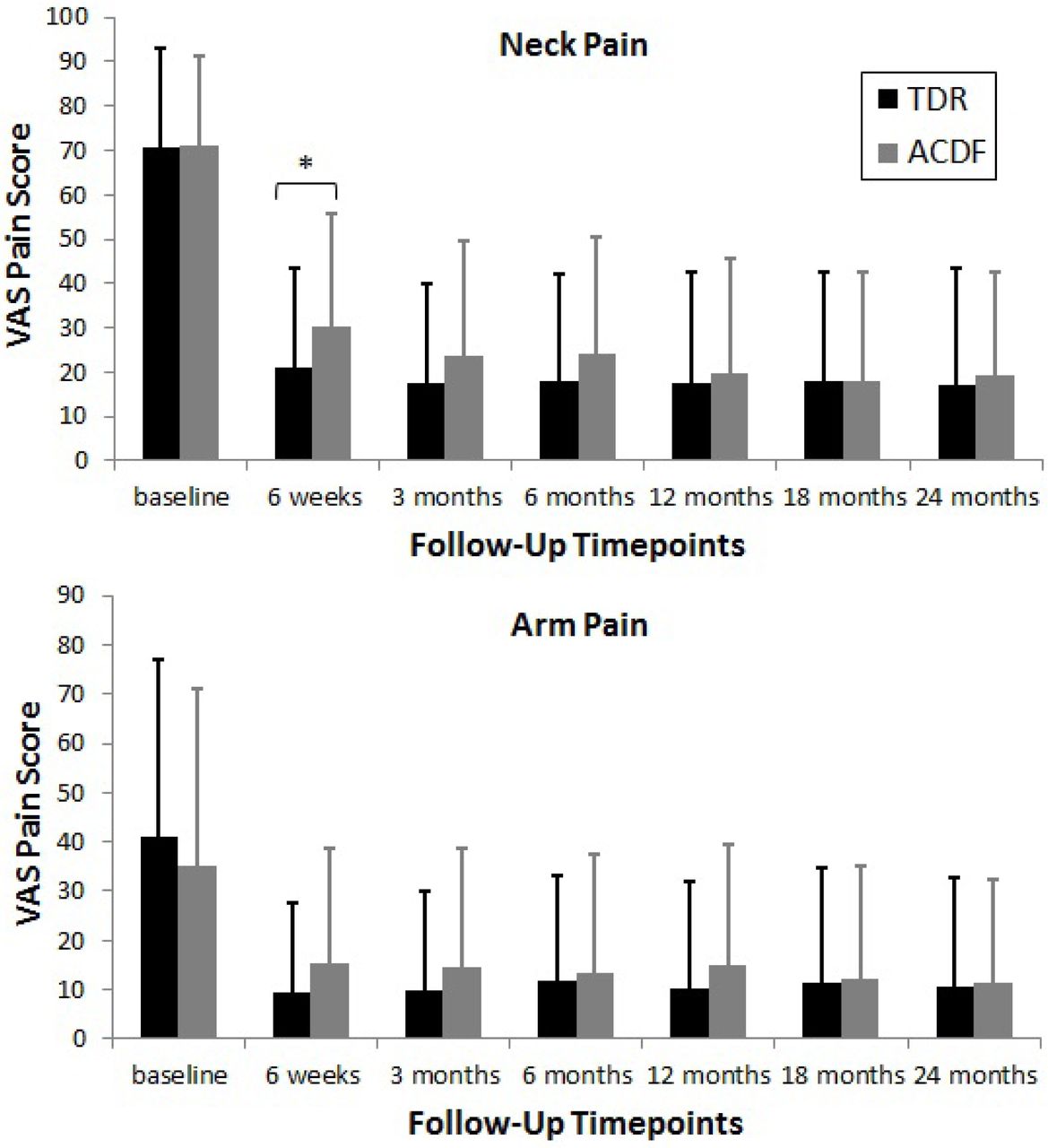
- Fig. 6
Mean VAS scores by Time point. VAS pain scores were collected at each follow-up visit. Error bars represent standard deviations. VAS scores for both treatment groups were significantly different from baseline at all time points (p < 0.05) * Denotes significant difference determined using unpaired t-test to compare the change from baseline between the two treatments (p < 0.05).
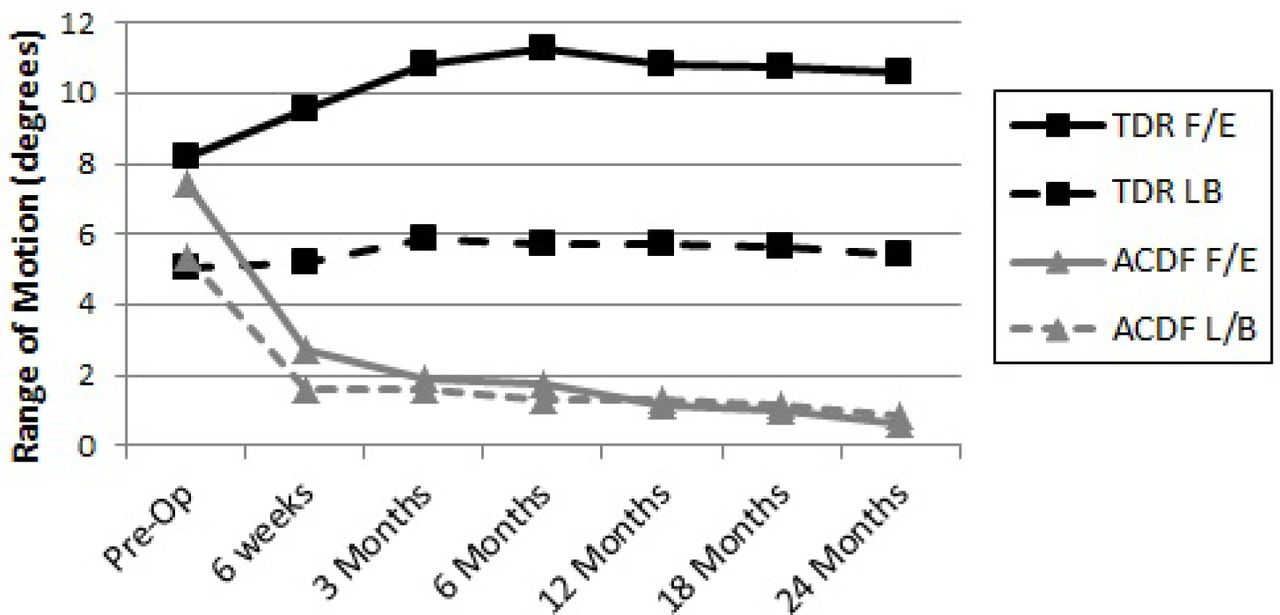
- Fig. 7
Range of Motion by Time point. Line graph demonstrating range of motion at the treated segment in Flexion/Extension (F/E) and Right/Left Lateral Bending (LB)
- Fig. 8
Mean SF-12 PCS and MCS scores by Time point. SF-12 physical component score (PCS) and mental health component score (MCS) were collected at baseline, 6, 12, 18, and 24 months. Error bars represent standard deviations. SF-12 scores for both treatment groups were significantly different from baseline at all time points (p < 0.05) * Denotes significant difference determined using unpaired t-test to compare the change from baseline between the two treatments (p < 0.05).





Tables
Inclusion criteria Age 18-69 years
Symptomatic cervical degenerative disc disease in only one level between C3-C7 with:
Neck and/or arm pain and/or
Decreased muscle strength and/or
Abnormal sensation and/or abnormal reflexes
Deficit confirmed by imaging (CT, MRI, or X-ray)
NDI score of ≥ 30
Unresponsive to non-operative, conservative treatment for at least 6 weeks or presence of progressive symptoms or signs of nerve root/spinal cord compression despite continued non-operative treatment
No prior surgery at the operative level and no prior cervical fusion procedure at any level
Physically and mentally able and willing to comply with the protocol
Signed informed consent
Willingness to discontinue all use of non-steroidal anti-inflammatory drugs (NSAIDs) from one week before surgery until 3 months after surgery
Exclusion criteria More than one vertebral level requiring treatment/immobile level between C1 and C7 from any cause
Any prior spine surgery at operative level of any prior cervical fusion at any level
Disc height less than 3 mm
T-score less than -1.5 (osteoporosis evaluation)
Paget's disease, osteomalacia, or any other metabolic bone disease other than osteoporosis
Active systemic infection of surgical site or history of or anticipated treatment for systemic infection including HIV/Hepatitis C
Active malignancy: a history of any invasive malignancy (except non-melanoma skin cancer), unless treated with curative intent and there had been no clinical signs or symptoms of the malignancy > 5 years
Marked cervical instability on resting lateral or flexion-extension radiographs
Known allergy to cobalt, chromium, molybdenum, or polyethylene
Segmental angulation of greater than 11° at treatment or adjacent levels
Rheumatoid arthritis, lupus, or other autoimmune disease
Any diseases or conditions that would preclude accurate clinical evaluation
Daily, high-dose oral and/or inhaled steroids or a history of chronic use of high dose steroids
BMI > 40
Use of any other investigational drug or medical device within 30 days prior to surgery
Pending personal litigation relating to spinal injury (worker's compensation not included)
Smoking more than one pack of cigarettes per day
Reported to have mental illness or belonged to a vulnerable population
Patient Group Variable TDR ACDF p value Age (years) 0.5657* N 164 81 Mean (SD) 43.3 (9.2) 44.0 (8.2) Gender n (%) 0.6843** Male 78 (47.6%) 36 (44.4%) Female 86 (52.4%) 45 (55.6%) Ethnicity n (%) 0.6667** Hispanic or Latino 3 (1.8%) 2 (2.5%) Not Hispanic or Latino 161 (98.2%) 79 (97.5%) Race n (%) 0.0710** American Indian 2 (1.2%) 1 (1.2%) Caucasian 152 (92.7%) 69 (85.2%) Asian 3 (1.8%) 1 (1.2%) Black or African American 4 (2.4%) 10 (12.3%) Native Hawaiian/Other Pacific Islander 1 (0.6%) 0 Other 2 (1.2%) 0 BMI 0.8460* Mean (SD) 27.3 (4.4) 27.4 (4.2) Work Status n (%) 0.3264** Being able to work 108 (65.9%) 46 (56.8%) Not being able to work 37 (22.6%) 22 (27.2%) N/A 19 (11.6%) 13 (16.0%) Driving Status n (%) 0.5035** Being able to drive 155 (94.5%) 79 (97.5%) Not being able to drive 8 (4.9%) 2 (2.5%) N/A 1 (0.6%) 0 NDI Mean (SD) 54.0 (14.0) 54.2 (14.6) 0.9290* VAS Neck Pain Mean (SD) 70.8 (22.4) 70.1 (21.5) 0.8354* VAS Left Arm Pain Mean (SD) 46.7 (36.5) 55.3 (37.3) 0.0839* VAS Right Arm Pain Mean (SD) 41.0 (36.2) 34.8 (35.6) 0.2104* SF-12 PCS Mean (SD) 32.5 (5.91) 33.8 (6.36) 0.1055* SF-12 MCS Mean (SD) 42.1 (13.1) 42.2 (10.4) 0.9792* - Table 4
All Treatment Emergent Adverse Events through 24 Months in US IDE Study – All Study Subjects.
Mobi-C ACDF Complication #Patients (% of 179) Total Events #Patients (% of 81) Total Events All Adverse Events 1 170 (95.0%) 1229 75 (92.6%) 688 Anatomy/Technical Difficulty 11 (6.1%) 12 2 (2.5%) 4 Cervical –Study Surgery 4 (2.2%) 4 2 (2.5%) 3 Cervical – Non Study Surgery 5 (2.8%) 6 1 (1.2%) 1 Non-Cervical 2 (1.1%) 2 0 (0.0%) 0 Cancer 4 (2.2%) 5 1 (1.2%) 2 Cardiovascular 20 (11.2%) 26 10 (12.3%) 10 Death 0 0 0 0 Dysphagia/Dysphonia 20 (11.2%) 26 17 (21.0%) 20 Dysphagia 19 (10.6%) 22 15 (18.5%) 17 Dysphonia 3 (1.7%) 4 3 (3.7%) 3 Gastrointestinal 39 (21.8%) 60 15 (18.5%) 37 Heterotopic Ossification 9 (5.0%) 10 4 (4.9%) 4 Cervical - Index Level 5 (2.8%) 5 0 (0.0%) 0 Cervical - Adjacent Level 1 (0.6%) 1 1 (1.2%) 1 Non Cervical 4 (2.2%) 4 3 (3.7%) 3 Infection 33 (18.4%) 51 20 (24.7%) 28 Superficial Wound – Cervical 6 (3.4%) 7 1 (1.2%) 1 Deep Wound – Cervical 0 0 0 0 Other Wound - Non Study Surgery 1 (0.6%) 1 3 (3.7%) 3 Systemic 8 (4.5%) 9 2 (2.5%) 3 Local 20 (11.2%) 34 18 (22.2%) 21 Malpositioned Implant 2 (1.1%) 2 1 (1.2%) 1 Neck and/or Arm Pain 102 (57.0%) 212 47 (58.0%) 98 Neck Pain 74 (41.3%) 123 37 (45.7%) 56 Arm Pain 46 (25.7%) 76 20 (24.7)% 25 Neck And Arm Pain 9 (5.0%) 13 7 (8.6%) 17 Neurological 121 (67.6%) 401 52 (64.2%) 215 Upper Extremity – Sensory 67 (37.4%) 175 32 (39.5%) 126 Upper Extremity – Motor 26 (14.5%) 43 15 (18.5%) 20 Upper Extremity – Reflex 18 (10.1%) 44 7 (8.6%) 20 Lower Extremity – Sensory 11 (6.1%) 22 2 (2.5%) 3 Lower Extremity – Motor 6 (3.4%) 9 4 (4.9%) 4 Lower Extremity – Reflex 0 (0.0%) 0 1 (1.2%) 1 Upper & Lower Extremity - Sensory 1 ( 0.6%) 1 1 (1.2%) 1 Upper & Lower Extremity – Motor 0 0 0 0 Upper & Lower Extremity - Reflex 0 0 0 0 Neck 41 (22.9%) 51 21 (25.9%) 21 Back 7 (3.9%) 8 2 (2.5%) 2 Spinal Cord Disturbance 0 0 0 0 Gait Disturbance 1 (0.6%) 1 1 (1.2%) 1 Non Specific 6 (3.4%) 6 1 (1.2%) 1 Other* 35 (19.6%) 41 8 (9.9%) 15 Non-Union 0 (0.0%) 0 4 (4.9%) 4 Other** 77 (43.0%) 114 33 (40.7%) 66 Other Pain 102 (57.0%) 226 47 (58.0%) 144 Shoulder 39 (21.8%) 55 21 (25.9%) 31 Back 44 (24.6%) 50 18 ( 22.2%) 30 Torso 5 (2.8%) 7 3 (3.7%) 4 Lower Extremity 26 (14.5%) 40 12 (14.8%) 29 Headache 45 (25.1%) 58 26 (32.1%) 41 Otherr*** 15 (8.4%) 16 8 (9.9%) 9 Respiratory 6 (3.4%) 6 6 (7.4%) 8 Spinal Disorder 6 (3.4%) 7 10 (12.3%) 12 Cervical - Study Surgery 1 (0.6%) 1 2 (2.5%) 2 Cervical - Non Study Surgery 5 (2.8%) 6 3 (3.7%) 3 Non Cervical 0 (0.0%) 0 5 (6.2%) 7 Trauma 47 (26.3%) 70 20 (24.7%) 38 Upper Extremity Nerve Entrapment 8 (4.5%) 9 4 (4.9%) 5 Urogenital 9 (5.0%) 11 9 (11.1%) 12 Vascular Intraop 1 (0.6%) 1 0 (0.0%) 0 Wound Issue - Non-Infection 1 (0.6%) 1 3 (3.7%) 3 Hematoma 1 (0.6%) 1 3 (3.7%) 3 Hematoma Evacuation 0 0 0 0 CSF Leakage 0 0 0 0 M= All Mobi-C Subjects; F = All ACDF Subjects
↵1 Sum of all treatment emergent adverse events experienced in the study for each treatment group.
↵* Neurological Other includes Neurological events not appropriately defined elsewhere in the Neurological category. This includes amnesia, convulsion, facial neurologic events (dysaesthesia, hypoaesthesia), unexplained loss of consciousness, ‘other’ nerve compression, Parkinson's disease, and stroke.
↵** Other includes events not appropriately defined elsewhere. This includes adverse drug reactions, allergies, anemia, anxiety, arthritis, attention deficit disorder, benign neoplasm, blood & lymphatic system disorders, complications from other medical procedures, congenital defects, dehydration, dermatitis, diabetes, dizziness, ear/eye disorders, endocrine disorders, fatigue, feeling hot, fever, gout, high/low cholesterol, immune system disorders, injury/poisoning, lupus, menopause, miscarriage, muscle atrophy, nutritional disorders, obesity, osteoarthritis, osteoporosis, other inflammation, other medical procedures, plantar fasciitis, polyps, pregnancy, psychiatric disorders, rotator cuff syndrome, skin disorders, sinus infection, social issues, sleep disorders, swelling, tendonitis, thyroid conditions, vascular disorders, and weight gain/loss.
↵*** Other Pain Other includes events not appropriately defined elsewhere. This includes facial pain, fibromyalgia, muscle soreness, chronic pain, nerve pain and arthritis.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Four-Level Cervical Disc Arthroplasty
- Cervical Disc Arthroplasty vs Anterior Cervical Discectomy and Fusion at 10 Years: Results From a Prospective, Randomized Clinical Trial at 3 Sites
- Cervical Disc Arthroplasty vs Anterior Cervical Discectomy and Fusion at 10 Years: Results From a Prospective, Randomized Clinical Trial at 3 Sites
- 2021 Position Statement From the International Society for the Advancement of Spine Surgery on Cervical and Lumbar Disc Replacement
- Adjacent Segment Pathology After Treatment With Cervical Disc Arthroplasty or Anterior Cervical Discectomy and Fusion, Part 1: Radiographic Results at 7-Year Follow-Up
- Adjacent Segment Pathology After Treatment With Cervical Disc Arthroplasty or Anterior Cervical Discectomy and Fusion, Part 2: Clinical Results at 7-Year Follow-Up