


Abstract
Background Amniotic membrane tissue has been thought to potentiate healing in many soft tissue conditions. Specifically, recent studies have shown its therapeutic potential for treatment in the setting of spinal pathologies. The purpose of this study is to thoroughly review the existing scientific literature and evidence concerning the clinical use of amniotic membrane–derived biologic agents on postoperative outcomes following spinal surgery.
Methods A systematic review was conducted following preferred reporting items for systematic reviews and meta-analyses guidelines using PubMed, Embase, and Cochrane databases up to December 2020 to identify animal and clinical studies examining the therapeutic potential for amniotic membrane tissue in the setting of spinal pathologies (including disc herniation, prevention of epidural fibrosis, and spinal fusion). Studies were broken down into 2 categories: experimental model type and the type of amnion product being analyzed.
Results A total of 12 studies (4 clinical studies and 8 studies utilizing animal models) met inclusion criteria. Additionally, the major types of amnion product were divided into cryopreserved/freeze-dried amniotic membrane, human amniotic fluid, human amniotic membrane, cross-linked amniotic membrane, and amnion-derived epithelial cells. While heterogeneity of study design precludes definitive specific results reporting, most studies showed positive benefits on healing/outcomes with amniotic augmentation. Specifically, amnion products have shown promising effects in reducing epidural adhesions and scar tissue after spine surgery, improving spinal fusion rate and postoperative pain scores, and promoting better functional outcomes after spine surgery.
Conclusions A review of the limited number of reported studies revealed a wide variety of amniotic membrane preparations, treatment regimens, and indications, which limit definitive conclusions. To date, while there is no definitive clinical proof that amniotic tissues enhance tissue repair or regeneration, the aggregate results demonstrate promising basic science and outcomes potential in spinal surgery. Further study is warranted to determine whether this application is appropriate in the clinical setting.
Clinical Relevance This systematic review provides a summary of the existing literature regarding the use of amniotic membrane preparations, treatment regimens, and indications within spinal surgery. With the growing popularity and utilization of biologic agents such as amniotic membrane-derived products in orthopedic and neurologic surgery, this systematic review gives physicians a concise summary on the outcomes and indications associated with amniotic membrane products.
Level of Evidence 4.
- amniotic membrane
- chorionic membrane
- umbilical cord
- epidural injection
- microdiscectomy
- intervertebral disc
- disc herniation
- epidural fibrosis
- spinal dysraphism
Introduction
The use of biologic agents in orthopedic and spine surgery remains an area of continued growth and interest.1 Biologic agents such as platelet-derived growth factor, bone marrow aspirate (BMA) concentrate, platelet-rich plasma, demineralized bone matrix, and bone morphogenic proteins have all been used with varying success in an effort to reduce inflammation, stimulate angiogenesis, and ultimately induce healing after orthopedic and spine procedures.2–8 A common source for many of these agents is mesenchymal stem cells (MSC). Recently, the use of MSCs and their growth factors in orthopedics and spinal surgery has increased in popularity as MSC-derived products have become more widely available, in addition to promising research study results.9–19
MSCs and their associated growth factors can be isolated from a variety of tissue types including placental tissue, bone marrow, synovial tissue, and adipose tissue.20–24 However, placental tissue has gained favor as a source of abundant MSCs in addition to some of the other regenerative factors mentioned above.25 The human placenta is made up of several membranes and tissue that surround the developing fetus and provide sustenance and protection. The umbilical cord, amnion, and chorion are of particular importance in regard to their use as a potential source of MSCs and associated growth factors; however, the focus of the present analysis will be amniotic-derived cell-free products.
The amnion is a placental tissue that originates from trophoblasts and envelopes the developing fetus.26 The amnion has an epithelial cell layer and a mesenchymal cell layer that are both sources of MSCs. Amniotic epithelial cells are known to manufacture hepatocyte growth factor, epidermal growth factor, keratinocyte growth factor, and fibroblast growth factor, which are strong promoters of epithelization, tenocyte proliferation, and neural differentiation.1,27,28 They also inhibit the local immune response and possess the unique ability to differentiate into cells of all 3 germ lines.29,30 In clinical practice, it is the amnion-derived growth factors, such as those mentioned above, that are potentially beneficial in promoting healing and decreasing fibrosis. The vast majority of amnion products in the United States are “cell free,” meaning the MSCs themselves are excluded in favor of the growth factors they produce. Similarly, embryonic-derived mesenchymal stromal cells have the capacity to stimulate angiogenesis and suppress local innate and adaptive immune responses via the production of a variety of growth factors that are isolated for use in clinical applications.1,29 Notably, the unique qualities of amnion-derived epithelial and mesenchymal cells have exhibited strong osteogenic and chondrogenic differentiation, especially when compared with other sources of MSCs.31
Despite the emerging research and prevalent marketing/promotion of amnion-derived products in spine surgery, there exists a paucity in the literature to fully support their clinical use. As the use of amnion-derived products in spine surgery gains momentum, the outcomes of their use in animal and human models are of particular importance. Therefore, the purpose of this study is to thoroughly review the existing scientific literature and evidence concerning the clinical use of amniotic membrane–derived biologic agents on postoperative outcomes following spinal surgery.
Methods
This systematic review was conducted using preferred reporting items for systematic reviews and meta-analyses guidelines. Two independent reviewers conducted the initial literature search in December 2020 using PubMed, Embase, and Cochrane Central Register of Controlled Trials databases. A broad-based search was conducted to ensure no studies were missed using the following search terms: “‘amnion and spine’ or ‘amniotic and spine’.” All searches were conducted from database inception to the time of search (December 2020). Studies were included in the systematic review if they reported clinical, biological, biomechanical, patient-reported outcomes, or radiographic findings of human or animal studies examining the effect of amniotic membrane after spinal surgery. Only full-text manuscripts written in the English language were included, and no level of evidence restrictions were imposed. Technique articles, review articles, letters to the editor, and conference abstracts or studies not published in the English language were excluded.
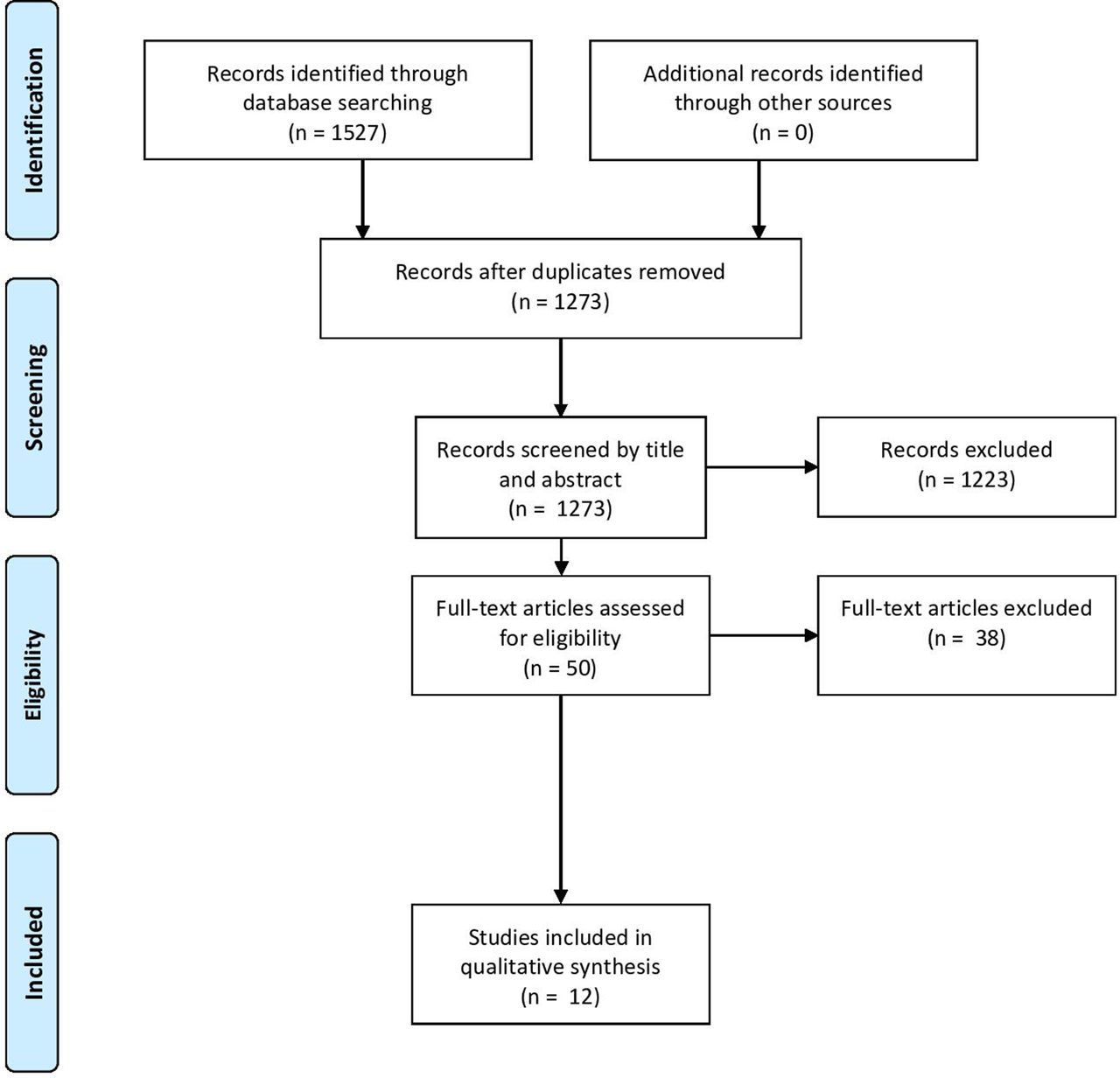
The search results were reviewed independently by 2 authors to select studies for inclusion in the review. After removal of duplicates, the initial keyword literature search produced a total of 1273 references. Fifty studies were identified for inclusion from the literature search based on appropriateness of title and abstract content and were related to the application of amniotic tissue for the treatment of disc pathology or prevention of scar tissue formation after spinal interventions. These 50 studies then underwent full-text review to confirm appropriateness for inclusion. The reference list and text of each latter manuscript were cross-referenced to identify any additional studies related to the study topic not previously found. Following full-text review and cross-referencing, 12 studies met all criteria for inclusion and were included in the review.32–43 After each step of the review process, any disagreement on inclusion of a study was resolved by discussion between the 2 reviewers. If consensus could not be reached, then inclusion was decided by a third reviewer. A flow diagram outlining the selection process is found in the Figure.

Preferred reporting items for systematic reviews and meta-analyses flowchart outlining the literature review and selection process.
The 12 studies were subsequently divided based on study design to allow for simplified organization and improved comparison between similar studies. The 2 main categories were experimental model type and the type of amnion product being analyzed. Within the experimental model type category, subcategories were human models, rat models, sheep model, rabbit model, and dog model. Additionally, the major types of amnion product could be divided into cryopreserved/freeze-dried amniotic membrane (cAM/FAM), human amniotic fluid (HAF), human amniotic membrane (HAM), cross-linked amniotic membrane (CAM), and amnion-derived epithelial cells (AECs).
For all selected studies, the full text was accessed and thoroughly reviewed. The study design, experimental model, tissue type being experimented with, study objective, study methods, and main results for each article were all recorded and summarized in Table 1. The level of evidence was also collected for each article according to the Journal of Bone and Joint Surgery Levels of Evidence classification.44 Given the heterogeneity of the included studies, no calculable aggregate data or meta-analyses are presented in this review.
Summary of literature review for amniotic membrane–derived biologic agents on postoperative outcomes following spinal surgery.
Results
A total of 12 studies published between 2009 and 2020 met all previously outlined inclusion and exclusion criteria and were included in the systematic review.32–43 Regarding levels of evidence, 2 studies were level I, 7 were level II, 1 was level III, and 2 were level IV. Four studies used human models,32,37,41,43 and 8 studies used animal models.33–36,38–40,42 Of the animal models, 4 used rat models,33,34,38,40 2 sheep models,35,36 1 dog model,42 and 1 rabbit model.39 Regarding amniotic product type, 5 studies utilized either cAM or FAM,32,34,37,41,42 4 utilized HAF,33,38–40 4 utilized HAM,35,38,39,43 1 utilized CAM,42 and 1 utilized AEC.36 Two studies analyzed both HAF and HAM in the same study, while another study analyzed both FAM and CAM. Study characteristics and major methodology and results are summarized in Table 1.
Animal Model
Bone Healing
Two studies assessed the effects of amnion products on bone healing.36,40 Goldschlager et al36 used AEC and mesenchymal precursor cells (MPCs), while Oner et al40 utilized HAF.
Goldschlager et al36 sought to compare the allogenic MPCs with AECs in promoting osteogenesis following anterior cervical discectomy. The investigation utilized 29 sheep divided into 5 groups receiving the following treatments: Fidji interbody cage (Abbott Spine, Bordeaux, France) packed with iliac crest autograph alone, hydroxyapatite-tricalcium phosphate (HA-TCP) Mastergraft granules (Medtronic, Fridley, Minnesota) alone, HA-TCP with 5 million MPCs, HA-TCP with 5 million AECs, and a group of age-matched nonoperative controls. The investigators found that there was significantly more fusion in the MPC group as compared with the 3 other experimental groups (P = 0.01). The MPC group found that 5 of the 6 sheep had continuous bony bridging at 3 months compared with 0 out of the 5 sheep in the AEC-treated group.36 Similarly, Oner et al40 reported rats receiving demineralized bone matrix combined with HAF had significantly better results in both radiologic and histologic evaluation of vertebral fusion results when compared with demineralized bone matrix alone following an L4-L6 spinal fusion 8 weeks after surgery (radiologic: P = 0.003; histologic: P < 0.001).
Inhibition of Scar Formation
A total of 5 studies assessed the formation of scar tissue following spinal procedures in animal models.33–35,38,42 Of these studies, 2 utilized HAF,33,38 2 utilized FAM,34,42 2 utilized HAM,35,38 and 1 utilized CAM.42
Bolat et al33 reported that all experimental groups (mitomycin-C, sodium hyaluronate, and HAF) had significantly less scar tissue compared with the control group 4 weeks after an L5 total laminectomy. Choi et al34 indicated that rats receiving FAM after laminectomy had significantly less scar tissue and a decrease in the tenacity of scar tissue when compared with the control group that did not receive FAM postlaminectomy (P < 0.05).
Cunningham et al35 evaluated the effects of dual-layer chorion-free amnion patch derived from HAM following lumbar laminectomy (at L3 and L5) in 12 sheep with 2 groups: control and amnion. The sheep served as their own control as the 2 laminectomy sites for each sheep were randomly assigned to the control or amnion group. The investigators found that at both 4 and 10 weeks postlaminectomy, there was a significant decrease in the amount of fibroblast infiltration (P < 0.05 for both 4 and 10 weeks). Additionally, at 10 weeks, tissue tenacity in the amnion-treated group was significantly less than the control (P < 0.05).35
Tao and Fan42 incorporated the use of 24 canine subjects that underwent laminectomy at L1, L3, L5, and L7. Experimental groups included: FAM, CAM, autologous-free fat, and a no treatment control. The study found that the CAM group experienced significantly lower scar burden (CAM vs autologous-free fat: P = 0.71; CAM vs control: P < 0.01) and epidural fibrosis and adhesion (CAM vs autologous-free fat: P = 0.36; CAM vs control: P < 0.01) when compared with the control group but not the autologous-free fat group. CAM was found to degrade more slowly when compared with FAM, which allowed an earlier infiltration by scar tissue. Additionally, the FAM, CAM, and no treatment groups all showed equivalent postlaminectomy bone growth.
In contrast, Kara et al38 found that rats undergoing laminectomy at 2 levels (L1 and L4) saw no significant difference between the HAF-treated rats, the HAM-treated rats, and the control group in terms of prevention of epidural scar tissue formation (HAF vs control: P = 0.718; HAM vs control: P = 0.400; HAF vs HAM: P = 0.140).
Disc Height
A single study by Luo et al39 utilized a rabbit experimental model to determine whether amniotic suspension allograft increases the intervertebral disc height and morphology after disc degeneration. Specifically, this study used amniotic suspension allograft derived from both particulated HAM and HAF. This analysis incorporated the use of 12 rabbits that underwent disc puncture and were then injected with amniotic suspension, sham control, or were untreated 4 weeks later. The rabbits were assessed over 12 weeks. Major findings showed that injection of amniotic suspension allograft derived from HAM and HAF had significant improvements in disc height and morphology when compared with the control and untreated groups (P = 0.043 for each).
Human Studies
Disc Herniation
Both Anderson et al32 and Kamson and Smith37 investigated the use of cAM/amniotic-derived products with similar outcomes. Specifically, Anderson et al found that when 80 patients were randomized to either a cAM group or control group following elective lumbar microdiscectomy, the cAM group experienced significantly greater functional outcomes and fewer recurrent herniations at 2 years postsurgery (P = 0.05 at 6 weeks and P = 0.02 at 24 months).32 Similarly, Kamson and Smith found that when 269 patients were randomized to receive either amniotic membrane, BMA, both, or no treatment during lumbar decompression, patients had significant decreases in pain. Patients receiving either BMA or amniotic membrane had significantly decreased mean visual analog scale measured back pain at 2 weeks (3.98 vs 5.01, P = 0.011), 2 months (3.22 vs 3.93, P = 0.04), 9 months (2.38 vs 4.11, P = 0.004), and 12 months (2.23 vs 3.58, P = 0.011).37 Moreover, mean visual analog scale measured leg pain had significant improvements for patients at 2 weeks (3.55 vs 4.77, P = 0.002), 6 months (2.34 vs 3.37, P = 0.026), and 9 months (2.18 vs 3.57, P = 0.01).37 There were no reportable complications noted intraoperatively in the 269 patients. Two patients experienced a reherniation (1 in the control group and 1 in the amnion group). The BMA only and both BMA and amniotic membrane groups experienced no reherniations.
Spinal Epidural Fibrosis/Scar Formation
Subach and Copay41 and Walker et al43 investigated the use of dehydrated human amnion/chorion membrane and HAM on the degree of fibrosis/scar tissue formation after spinal surgery, respectively. Subach and Copay utilized dehydrated human amnion/chorion membrane in 5 patients undergoing transforaminal lumbar interbody fusion and found that 4out of 5 cases had easily detachable fibrotic tissue during epidural re-exploration. Significant improvements in patient outcomes were also noted for back pain (P = 0.007), Oswestry Disability Index (P = 0.0032), and Medical Outcomes Study Questionnaire Short Form 36 (P = 0.0239).41 Additionally, Walker et al43 evaluated the effect of HAM in the prevention of spinal retethering after a detethering procedure in retrospective case series of 14 patients. The investigation found that only 1 patient experienced retethering after receiving a HAM graft in the prior detethering procedure suggesting that HAM grafts are a safe and potentially effective method of preventing microsurgical intradural adhesions.43
Discussion
As presented in this analysis, the few studies that have been conducted in animal models and human patients have shown promising effects in reducing epidural adhesions and scar tissue after spine surgery, improving spinal fusion rate and postoperative pain scores, and promoting better functional outcomes after spine surgery. Amniotic membrane tissue contains many factors that are theoretically optimal to support healing.1 It has historically been used for the treatment of burns and wounds.45 More recently, there is early evidence to support its role in the treatment of a number of musculoskeletal pathologies, including the spine.46 Notwithstanding, clinical research relating to amniotic membrane tissue in spinal surgery remains sparse. However, among the studies included in this analysis, very few complications have been reported suggesting the safety of amnion-derived products incorporated in spine procedures. Moreover, the existing evidence of amnion-derived biologic agents utilized in spine surgery shows promise in both animal and human models. Nevertheless, the current literature surrounding amniotic membrane products in spine surgery is inconclusive in its current state as this published research is mostly level IV evidence, heterogenous, consisting of many different treatment protocols, experimental subjects, and amnion-derived products.
Animal Studies
The evidence presented in this analysis is limited due to the nature of animal studies, which predominated the literature in this field. Eight of the 12 studies included in this analysis utilized animals as experimental models. The animals in these studies included dogs, rabbits, sheep, and rats.
Of these 8 animal studies, 6 showed promising results of amniotic membranes that may eventually translate to clinical practice. The encouraging outcomes included significant reductions in scar tissue and epidural fibrosis following spine surgery,33–35,42 greater disc height and improved morphology after disc degeneration,39 and enhanced posterior spinal fusion rates when combined with allograft.40 Studies by Goldschlager et al36 and Kara et al38 were the only animal studies that showed inconclusive results. Goldschlager et al found that AECs combined with HA/TCP failed to improve spinal fusion rates postlaminectomy.36 This is in contrast to the study by Oner et al that found improved spinal fusion rates when HAF was combined with bone allograft.40 Additionally, Kara et al discovered that HAF and HAM treatment groups showed no significant difference compared with the control in epidural scar formation and mean fibroblast count after undergoing lumbar laminectomy.38
While promising, results in the selected animal model studies came from a wide variety of amniotic products and experimental methodologies with some studies contradicting others, and it is essential to understand these results within their proper context. Animal models present researchers and scientists with a convenient and low-risk option in which to conduct preclinical studies; however, the translation to clinical trials and applicability often faces major barriers. Translation of medical treatments from animals to human subjects often disappoints for a variety of reasons including differing complexity, biology, and physiologic regulation between species.47 While experiments conducted on animal models is a necessity in order to discover effective treatments that can be used in humans, the jump to clinical practice is very wide and often unobtainable. Therefore, the findings from these studies should be interpreted with caution.
Amnion-Derived Products
Another shortfall of the applicability of the studies included in this analysis is the wide variety of amnion-derived products, preparations, dosages, and administration. Amnion products and preparations included cAM, FAM, dehydrated human amnion membrane, HAF, HAM, dual-layer chorion-free amnion patch from HAM, CAM, AECs, and amniotic suspension allograft containing particulated HAM and HAF. This equates to 9 different amnion-derived products or preparations of amnion distributed between 12 total studies. Therefore, drawing a sensible conclusion is made exceedingly difficult as no 2 studies are exactly alike in their most basic methodologies and treatments. Tables 2 and 3 summarize the variety of terms used throughout these heterogenous studies.
Summary of general stem cell terminology frequently used among selected articles.
Summary and unique distinctions of more specific amnion terminology used throughout the selected articles. Additional summary of spine surgery uses among the selected articles.
This inconsistency between studies and the amnion-derived products is only a small example of a much wider issue within the field of commercial tissue allografts. Tissue allografts are regulated by the Food and Drug Administration as a type of product known as “human cells, tissues, and cellular and tissue-based products” (HCT/Ps) as defined in Section 361 of the Public Health Service Act and Title 21 of the Code of Federal Regulations.48 Under the Section 361 classification, HCT/Ps, which includes placenta-derived products such as amniotic membrane, are required to meet only 4 criteria to uphold their classification as HCT/Ps. These criteria are (1) minimal manipulation, (2) homologous use, (3) not combined with drugs or devices, and (4) not reliant on cell metabolic activity as a primary function.25 HCT/Ps also require no premarket approval and have one of the fastest and most direct pathways to commercialization of all medical devices and pharmaceuticals.25 If a product does not meet the above requirements for classification as a HCT/P, they are required to be regulated by the Food and Drug Administration as biological drugs under Section 351 of the Public Health Service Act.25 This pathway to approval is very long and expensive, because it requires manufacturers to obtain a Biologics License Application and complete phase I to III clinical trials.25 Therefore, the vague regulation, minimal HCT/P criteria under Section 361, and lack of oversight in regard to tissue allografts such as amnion-derived products have led to a wide variety of commercial products that make comparisons exceedingly difficult. Table 4 contains a summary of 10 available amnion-derived products commonly used in orthopedic surgery.49 However, this list is likely not comprehensive as amnion-based products are being consistently released, discontinued, and rebranded under different names and formulation. Due to the small number of animal studies examined in this review, with variability of animal model, indications for use, preparation of amniotic tissue, dose, and administration, it is not possible to perform any comparative analysis. More research is needed to fully elucidate these differences.
Summary of 10 commonly utilized amnion-derived biologic agents used in orthopedics.
Human Studies
The 4 human studies in this analysis presented a promising outlook for the use of amnion in spine surgery. Results included improved functional outcomes and decreased risk of herniation following lumbar microdiscectomy,32 decreased pain following lumbar decompression,37 decreased epidural scar formation after transforaminal interbody fusion,41 and decreased retethering rates following an initial detethering procedure.43 These human studies involving amnion-derived cells in spine surgery currently represent a potential therapeutic advancement in spine surgery, but further clinical research in this field is needed to define the safety benefits, indications, and contraindications of amnion-derived cells in spine surgery.
Conclusion
A review of the limited number of reported studies revealed a wide variety of amniotic membrane preparations, treatment regimens, and indications, which limit definitive conclusions. To date, while there is no definitive clinical proof that amniotic tissues enhance tissue repair or regeneration, the aggregate results demonstrate promising basic science and outcomes potential in spinal surgery. Further study is warranted to determine whether this application is appropriate in the clinical setting.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests John M. Tokish discloses that he has received consulting and/or speaking/teaching fees from Arthrex, Inc.; DePuy, A Johnson and Johnson Company; and Mitek. Dr Tokish has also received travel funds from Arthrex, Inc, DePuy Synthes, and Stryker Corporation. Dr Tokish is on the board of directors for JSES and Orthopedics Today and is on the scientific advisory board for the Arthroscopy Association of North America. Matthew T. Neal discloses that he has received consulting fees from Medtronic, Inc and travel funds from Globus Medical, Inc. The remaining authors have nothing to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.