


Article Figures & Data
Figures
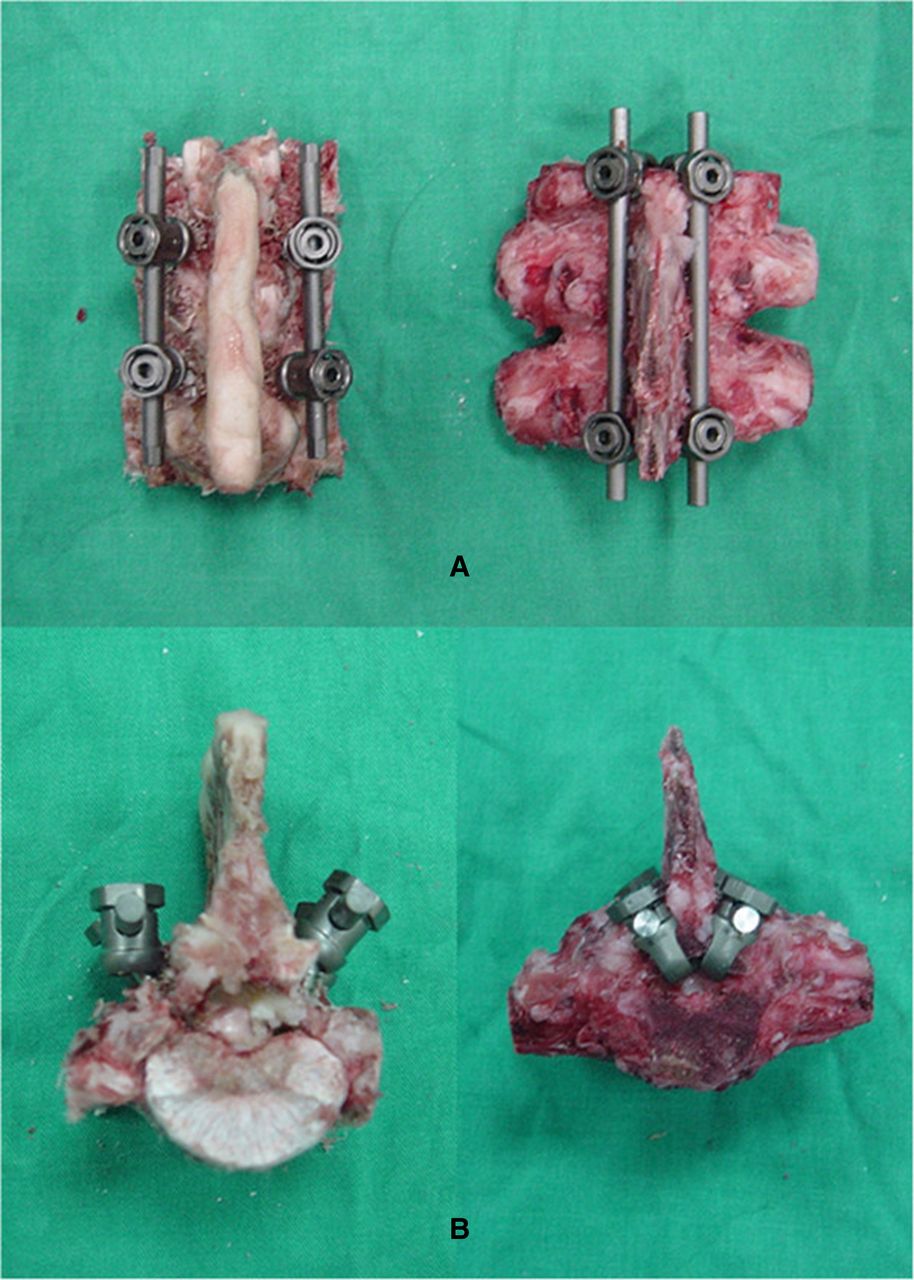
- Figure 1
Posterior (A) and superior (B) views of porcine spinal constructs instrumented with traditional pedicle screws, left, and laminar hooks, right. Source: Reprinted from Figure 4 in Tai et al. Biomechanical comparison of different combinations of hook and screw in one spine motion unit–an experiment in porcine model. BMC Musculoskelet Disord. 2014;15:19743 under Creative Commons CC BY license.
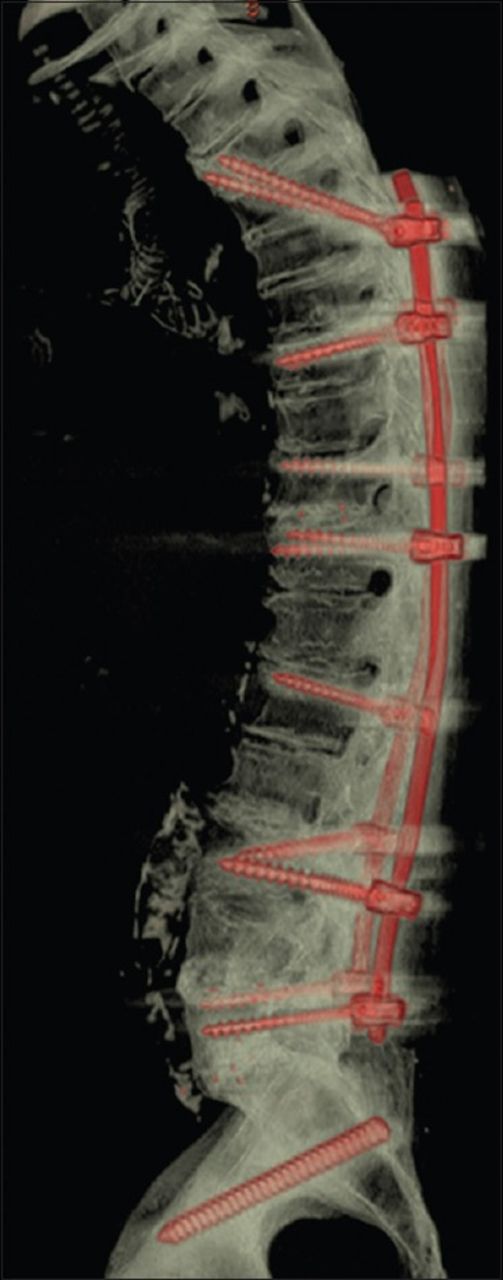
- Figure 2
Three-dimensional reconstruction demonstrating a multilevel stabilization screw construct. Source: Reprinted from Figure 3 in Sandquist et al. Preventing proximal junctional failure in long segmental instrumented cases of adult degenerative scoliosis using a multilevel stabilization screw technique. Surg Neurol Int. 2015;6:11235 under Creative Commons license CC BY.


Tables
First Author (Year) Study Type Quality Assessment No. of Patients Treatment for ASD Patient Age, y, Mean ± SD Minimum Follow-up (mo) Technique/Factor Investigated Results Association With PJK Incidence Buell (2021)23 Retrospective cohort Good 560 Long sacropelvic fusion 63 ± 9 24 UT vs LT UIV No difference in reoperation rates for PJK between UT group (9.8%) and LT group (8.6%) (P = 0.81) None Burks (2019)24 Retrospective case series Fair 36 Hybrid MIS-open surgical fusion, in which ≥2 most rostral levels were instrumented percutaneously 65 ± 11 12 Muscle-sparing technique at the proximal end PJK rate, 22% (n = 8); similar to reported rates; no reoperations for PJK/PJF No control for comparison; similar to reported literature rates Cazzulino (2021)25 Retrospective cohort Fair 39 Fusion using a soft-landing technique 61 ± 10 None specified; mean follow-up 26 months TPH Radiographic PJK in 16/39 patients at last follow-up; 4 patients met criteria for PJF with revision; 3 cases of compression fracture at the UIV or UIV+1 No control for comparison; similar to reported literature rates Cho (2013)26 Retrospective cohort Good 51 Posterior fusion; assigned to cohorts based on UIV location in relation to UEV and HV 68 ± 6 in the adjacent segment disease group, 63 ± 6 in the control 24 Selection of UIV PJK in 5 patients, 2 requiring fusion extensions/all had UIV below UEV; junctional kyphotic angles were not different between any groups Lower incidence of PJK with higher UIV Daniels (2019)27 Retrospective cohort Good 303 Posterior instrumentation 63 ± 9 24 UT vs LT UIV Lower PJK rate in UT compared with LT fusions (OR, 0.49; 95% CI, 0.24–0.99); no difference in PJF (OR, 0.54; 95% CI, 0.24–1.2) Lower incidence of PJK with higher UIV Ha (2013)28 Retrospective cohort Good 89 Various, treated 2007 to 2009 64 ± 7 (LT); 64 ± 11 (UT) 24 UT vs LT UIV PJK in 29 patients (23 in LT, 6 in UT, P = 0.61); 8 revision surgeries for PJK in LT group and 2 in UT group (P = 0.68); higher incidence of compression fracture in LT group (16/23, 70%), higher incidence of subluxation in UT group (3/6, 50%) (P = 0.014) None Hassanzadeh (2013)21 Retrospective cohort Good 47 Long (≥5 levels) spinal fusion, 2004 to 2009 46 (TPH); 51 (PS) 24 TPH PJK in 8/27 patients in PS group compared with none in the TPH group (P = 0.02) between immediate postoperative and final follow-up; 2/8 underwent revision surgery; mean PJA was 6.4° ± 10° in the TPH group and 22° ± 14° in PS group (P < 0.001) Lower incidence of PJK with TPH Kaufmann (2022)29 Prospective cohort Good 76 Posterior instrumentation and fusion of ≥3 levels; 2009 to 2017 at 1 center 64 ± 9 (MLSS); 55 ± 20 (control) 12 MLSS vs standard PS PJF in 10% of MLSS group, 31% of control (P = 0.02); less kyphosis in MLSS group (5.2° ± 6.3° compared with control 1.3° ± 5.3°, P = 0.01) Lower incidence of PJK with MLSS Kim (2014)9 Retrospective cohort Good 198 Long ( >5 levels) fusion, from a multicenter database 61 (UT); 62 (LT) 24 UT vs LT UIV No difference in PJK angle at 1- and 2-year follow-up (UT 14° vs LT 14° at 1 year; 17° vs 19° at 2 years); 5 patients underwent a revision for PJK (3 in UT group and 2 in LT group) (P = 0.45) None Kim (2007)30 Retrospective cohort Good 125 Instrumentation and fusion 52 ± 11 (T9-10); 57 ± 12 (T11-12); 62 ± 12 (L1-2) 24 UIV location (T9-10, T11-12, or L1-2) PJK in 51% in T0-10 group, 55% in T11-12 group, 36 % in L1-2 (P = 0.2) at final follow-up; 1 revision for PJK in T11-12 group and 3 in L1-2 group (P = 0.27); final change in PJA was not different between all groups (P = 0.46) None Lafage (2017)31 Case-control Good 252 Posterior fusion and instrumentation 61 ± 10 24 UT vs LT UIV PJK in 49 % of UT UIV group vs 64 % of LT/TL group (P = 0.02); smaller UIV inclination between PJK and non-PJK groups when stratified into both UT (P = 0.005) and LT/TL (P < 0.001) groups Lower incidence of PJK with higher UIV Line (2020)32 Retrospective cohort Good 625 Long (≥5 levels) spinal fusion 62 ± NA 12 No proximal fixation augmentation vs various augmentation options, including TPH PJF in 20% of no implant group, 11% of the implant group; 115 in TPH group, 7% rate of PJF (lowest of all augmentation), but 8.7% underwent surgical revision because of discrepancies in the definition for PJF used in the study (P < 0.05 for aforementioned rates of PJK) Lower risk of PJK with TPH Matsumura (2018)33 Retrospective cohort Fair 39 Corrective surgery performed, 2009 to 2013 67 ± NA 24 TPH PJK in 18% of TPH group vs 27% in PS group (P = 0.47); change in PJA greater in PS group (19°) than TPH group (5°) (P = 0.04) Lower incidence of PJK with TPH O’Shaughnessy (2012)34 Retrospective cohort Good 58 Fusion including the sacrum, treated 2002 to 2006 55 ± 9 (UT); 56 ± 8 (LT) 24 UT vs LT UIV PJK in 18% of LT group, 10% of UT group (P = 0.476); surgical PJK 2.6% in LT group, 0 in UT group (P > 0.99); no other differences in complications between groups None Sandquist (2015)35 Prospective cohort Good 15 Posterior instrumentation and fusion of ≥3 levels, 2009 to 2012 (subset from a study by Kaufmann et al) 66 ± NA 12 MLSS vs standard PS Mean change in PJA was 4.0° (range, –0.92 to 9.13); no cases of PJK or PJF were recorded Lower incidence of PJK with MLSS Scheer (2015)36 Retrospective cohort Good 165 PSO, from a multicenter database 60 ± 11 (UT); 60 ± 11 (LT) 24 UT vs LT/TL UIV PJK in 52% of UT group, 48% of LT/TL group (P = 0.85); 11 PJK cases requiring revision, 9/11 in TL/LT group and 2/11 in UT group (P = 0.03) No significant association with PJK incidence, higher incidence of PJF with lower UIV Tsutsui (2022)37 Retrospective cohort Good 53 Fusion from pelvis to T9 or T10 73 ± 4 (TPH); 72 ± 4 (PS) 12 TPH Higher incidence of PJK in TPH group (36%) vs PS group (8%) (P = 0.01); in TPH group, PJK caused in all cases by UIV or adjacent segment fracture with hook dislodgement Higher incidence of PJK with TPH Wang (2017)38 Retrospective cohort Good 242 Posterior fusion and instrumentation of ≥4 levels, from 2004 to 2014 59 ± 6 (PAS); 60 ± 6 (MAS) None; mean follow-up 25 ± 4 months PAS vs MAS at UIV PJK in 26/117 (22%) in MAS group, 30/125 (24) in PAS group (P = 0.73); greater change in PJA in PJK subgroup (2.9° vs 1.7°) (P = 0.03) None Yoshida (2020)39 Case-control Good 113 Surgery for degenerative spinal disorders, including both ASD (n = 45) and non-ASD patients (n = 68) 67 ± 8 (ASD); 57 ± 20 (non-ASD) 12 UIV to C2 plumb line distance PJK in 10/45 ASD patients; sub-analysis of PJK vs non-PJK patients showed significantly greater distances from UIV to both C7 and C2 plumb lines on standing and sitting radiographs for PJK group; on logistic regression analysis, UIV to C2 distance was found to be significantly associated with PJK (OR 1.2; 95% CI 1.0–1.3) UIV farther from C2 plumb line associated with a higher incidence of PJK Abbreviations: ASD, adult spinal deformity; CI, confidence interval;HV, horizontal vertebra; LT, lower thoracic;MAS, monoaxial screw; MIS, minimally invasive surgery; MLSS, multilevel stabilization screw; NA, not available; OR, odds ratio;PAS, polyaxial screw; PJA, proximal junctional angle; PJF, proximal junctional failure; PJK, proximal junctional kyphosis; PS, pedicle screw(s);PSO, pedicle subtraction osteotomy; TL, thoracolumbar; TPH, transverse process hooks; UEV, upper-end vertebra; UIV, upper instrumented vertebra; UT, upper thoracic.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.