


Article Figures & Data
Figures
- Figure 1
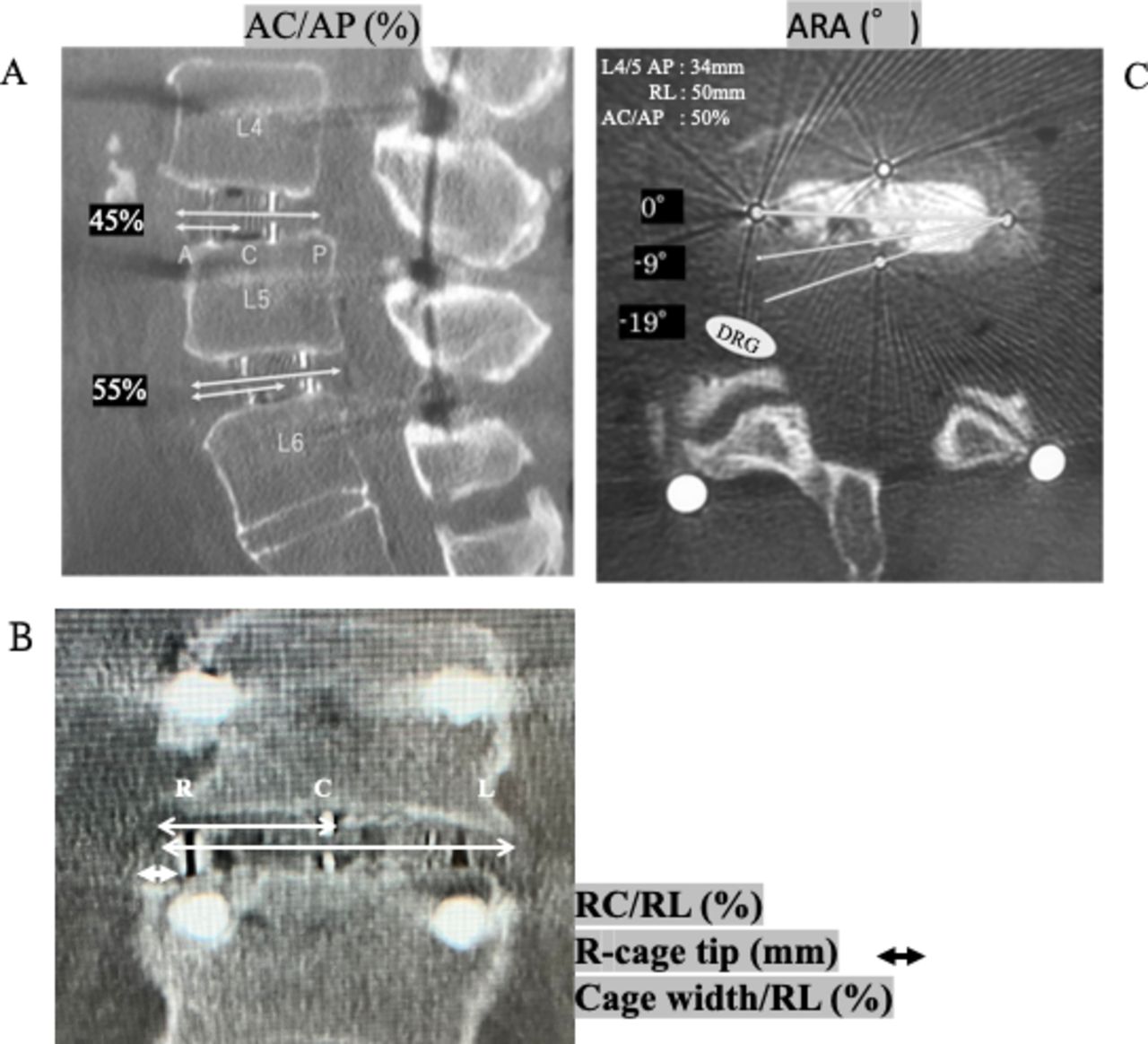
(A) The sagittal center of the cage (AC/AP value, %). (B) The coronal center of the cage (RC/RL value, %) and the distance between the cage tip and the right endplate edge (R-cage tip, mm). (C) The ARA (a posterior rotation from the transverse axis of the disc was expressed as "-") are measured on the MPR-CT images. The oblique lumbar interbody fusion cage (50 × 18 mm) is inserted orthogonally to the transverse axis (ARA: 0°) at 50% from the AC/AP at L4/5 (AP: 35 mm, RL: 50 mm). Three white lines indicate 0°, 9°, and 19° of posterior rotation (ARA: 0°, −9°, and −19°). A white oval indicates the right L5 exiting nerve root. Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; AP, anteroposterior; ARA, axial rotation angle;MPR-CT, multi-planar reconstruction computed tomography; RC/RL, right endplate edge-cage center/right-left endplate edge; RL, lateral (right-left).
- Figure 2
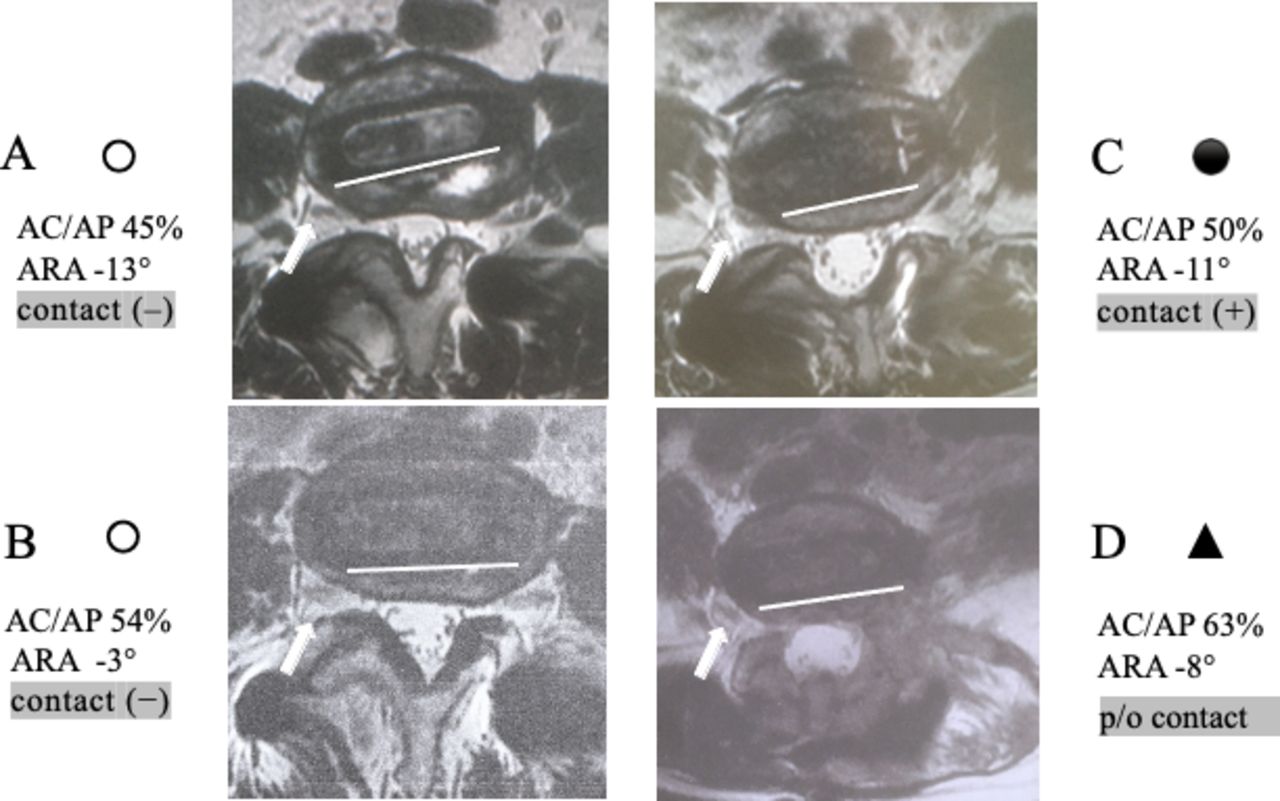
The position of the front (right) tip of the cage and the direction of the posterior edge of the inserted cage were determined on axial magnetic resonance imaging. (A and B) Cases without direct contact between the cage and the opposite exiting nerve (contact [−]: “○”). (C) A case with direct contact between the cage and the opposite nerve (contact [+]: “●”). (D) A case with the possibility of injury to the opposite nerve during intradiscal maneuvers despite no direct contact between the cage and the nerve (the oblique lumbar interbody fusion cage was inserted deeply just in front of the nerve and directed toward the nerve, possibility of contact: “▲”).
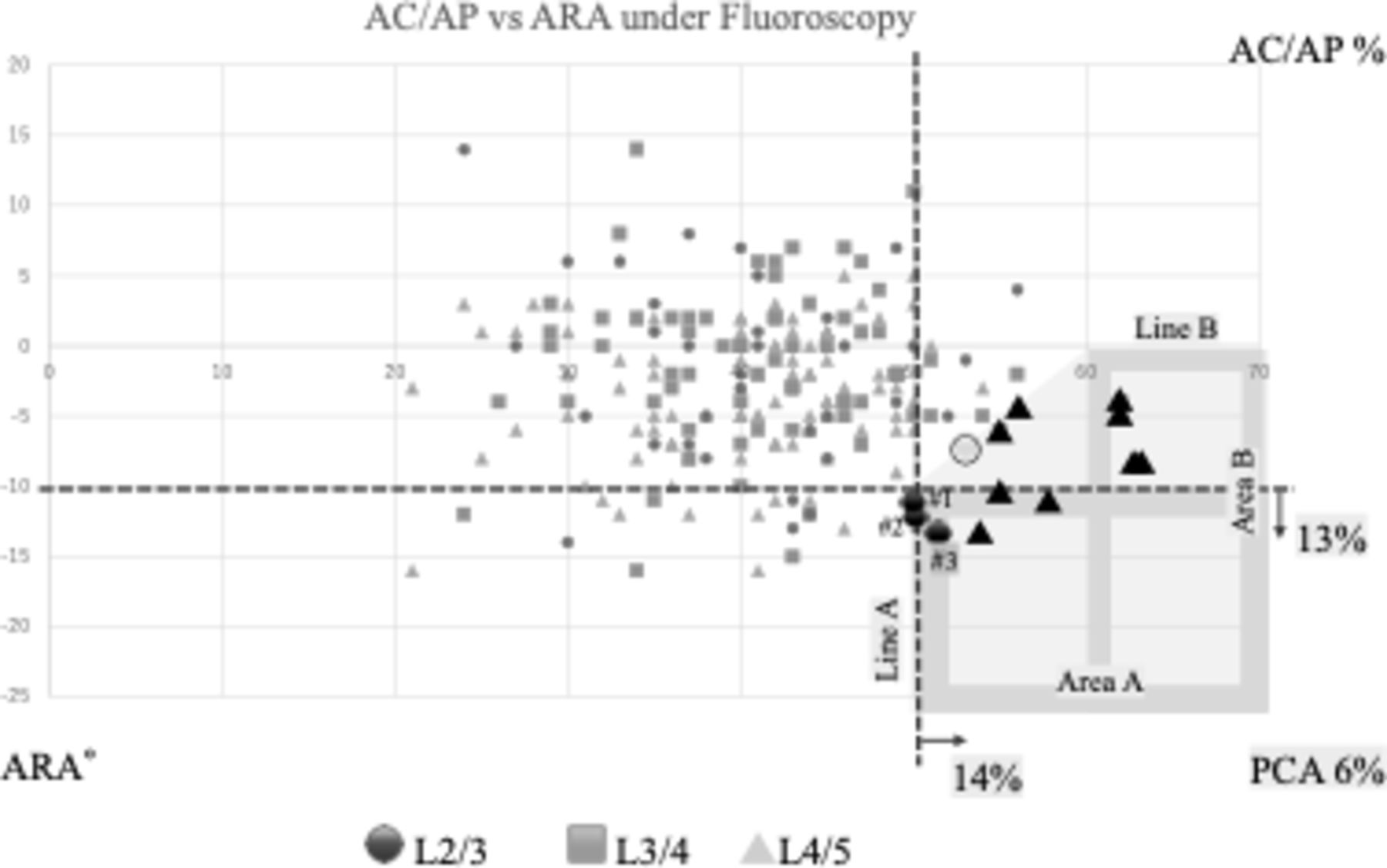
- Figure 3
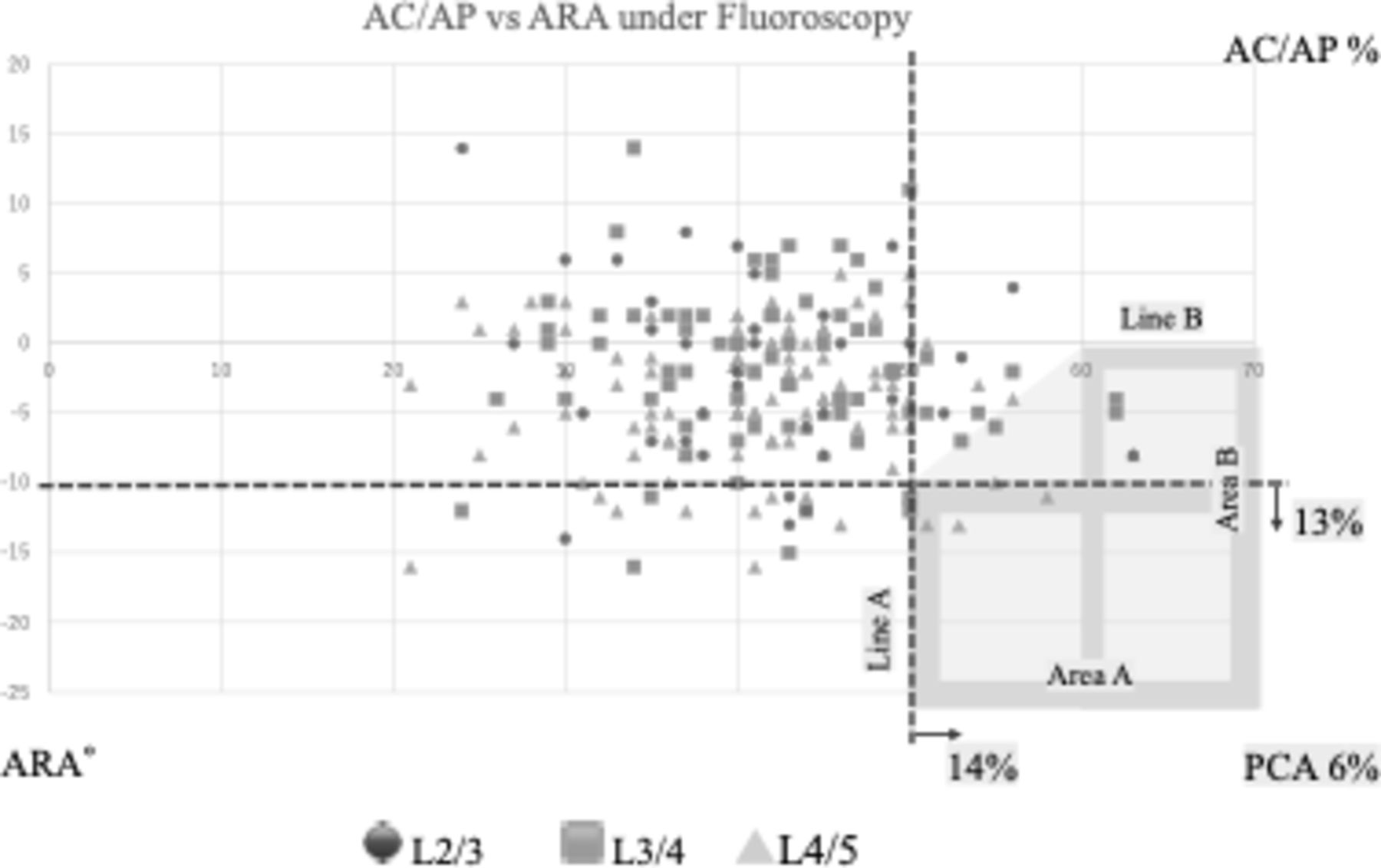
The sagittal center position (AC/AP value, the x-axis) and the axial rotation angle (ARA, the y-axis) of the oblique lumbar interbody fusion cages at L2/3 (n = 35), L3/4 (n = 72), and L4/5 (n = 108, including two L5/6 transitional vertebrae) were plotted on the scatter plot. The right-lower area delineated by lines A and B and a connected line between lines A and B shows a “PCA” (consisting of area A, area B, and a transition area is colored gray). Six percent of the total cages (13/215 cages) were inserted into this area. Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; ARA, axial rotation angle; PCA, potential contact area.
- Figure 4
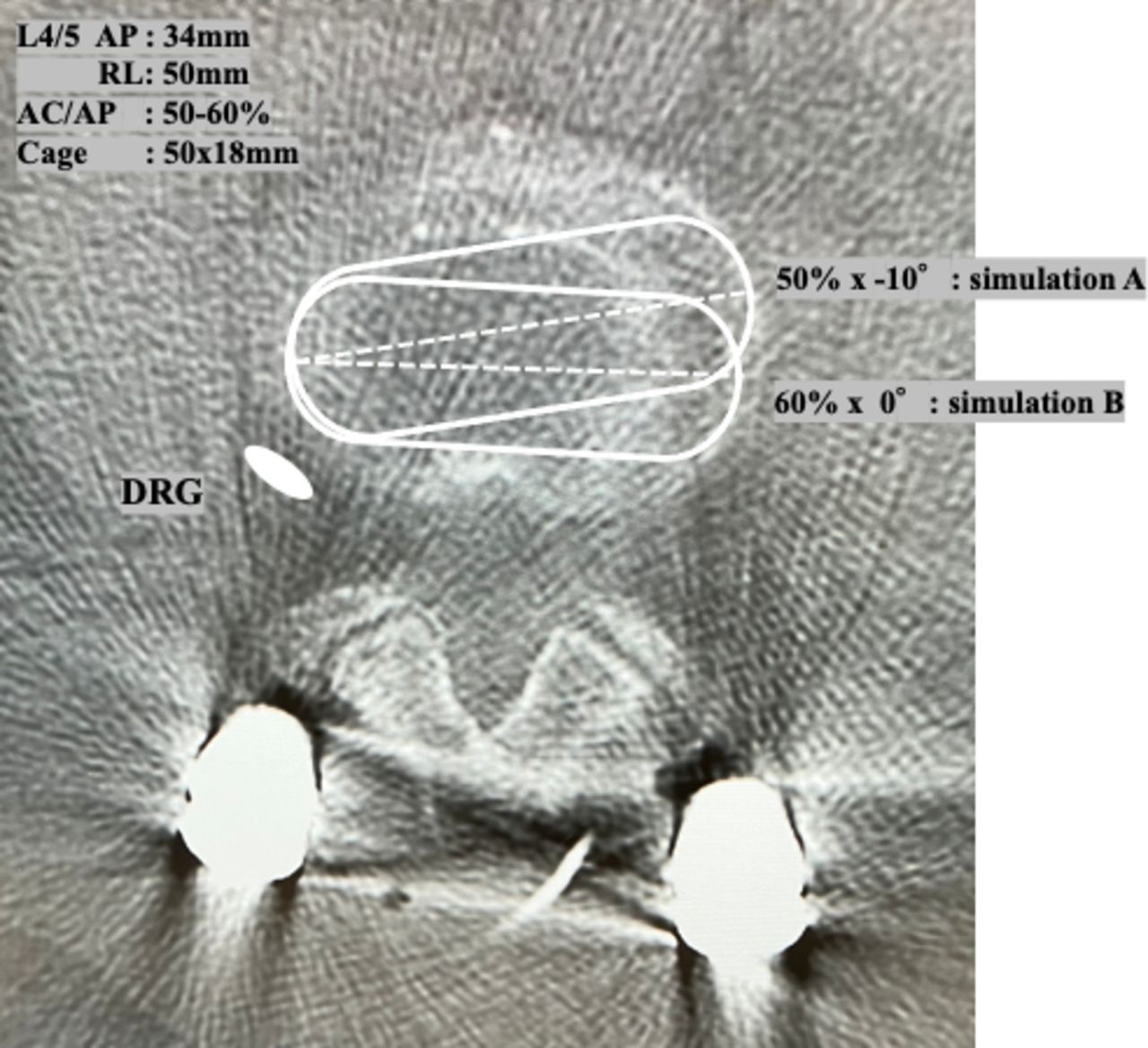
The possibility of contact between the front (right) tip of the oblique lumbar interbody fusion (OLIF) cage and the opposite exiting nerve root was simulated on the axial computed tomography image of the average-sized endplate at L4/5 (AP: 34 mm, RL: 50 mm). Simulation A: Cage insertion in the middle part of the disc space (50% of the AC/AP value) with 10° posterior rotation (axial rotation angle [ARA]: –10°); Simulation B: Cage insertion in the extremely rare part of the disc space (60% of the AC/AP value) without axial rotation (ARA: 0°). In both simulations, the OLIF cage could contact and injure the opposite exiting nerve if inserted deeply. Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; AP, anteroposterior; DRG, dorsal root ganglion; RL, lateral (right-left).
- Figure 5
Postoperative axial magnetic resonance imaging of 13 cages in PCA showed direct contact between the front (right) tip of the inserted cage and the opposite exiting nerve in 3 cages (#1–#3, contact [+]: “●”) and the possibility of contact during intradiscal maneuvers in 9 cages (possibility of contact: “▲”). One cage plotted on the border of the PCA showed no possibility of contact (contact [–]: “○”). Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; ARA, axial rotation angle; PCA, potential contact area.
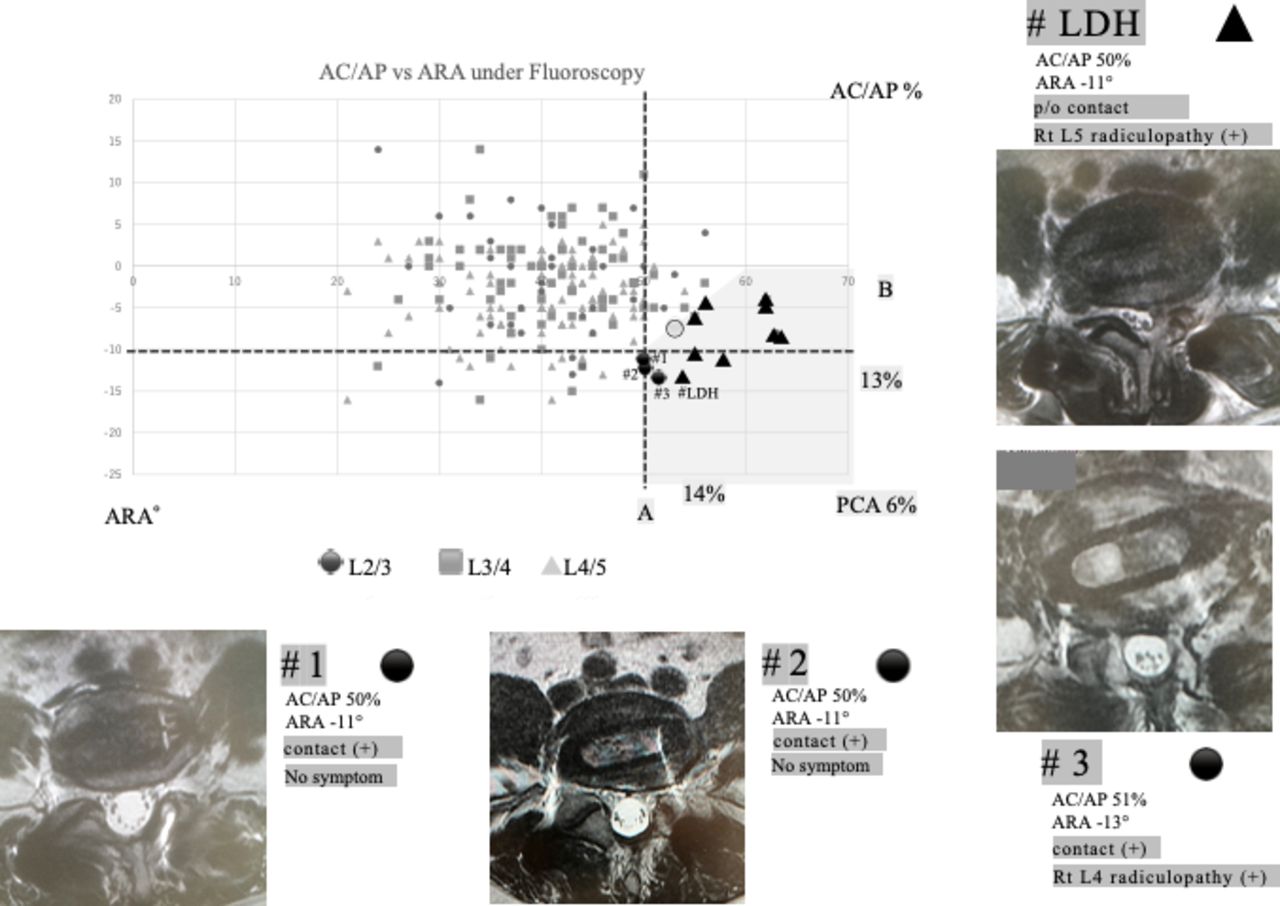
- Figure 6
Postoperative axial magnetic resonance imaging of 3 cages recognized as the contact (+) group and 1 cage causing extruded disc herniation within the PCA on the scatter plot are shown (cases #1–3 and #LDH). Cases #1 and #2 had direct contact between the cages and the opposite exiting nerves but had no symptoms (contact [+]: “●”). Case #3 had direct contact with the opposite nerve and presented with new-onset right L4 radiculopathy after oblique lumbar interbody fusion (OLIF; contact [+]: “●”). Case #LDH had right L5 radiculopathy due to extruded disc herniation induced by OLIF procedures, although there was no direct contact between the cage and the nerve (possibility of contact: “▲”). Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; ARA, axial rotation angle; LDH, lumbar disc herniation; PCA, potential contact area; p/o, possibility of.
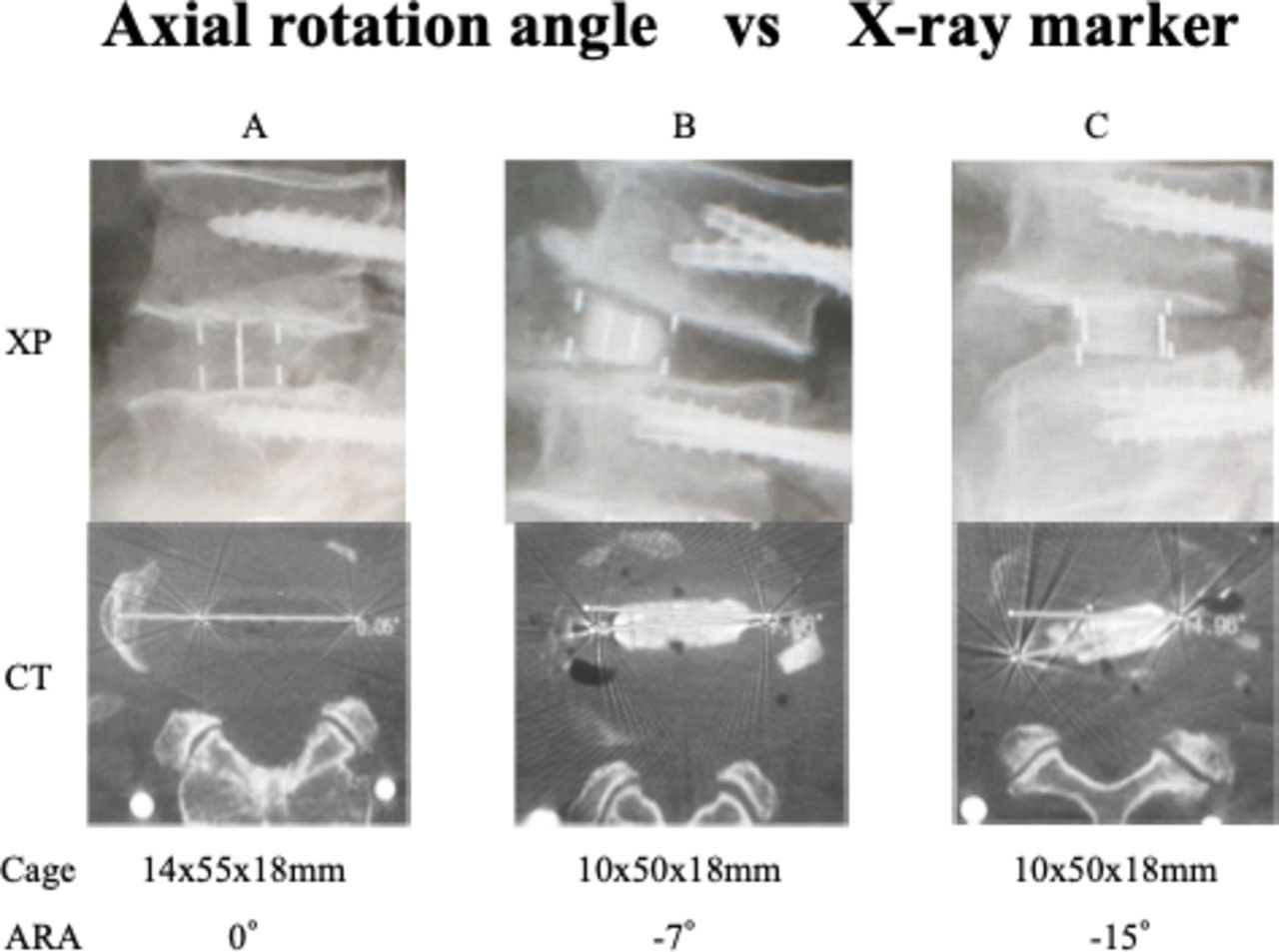
- Figure 7
The positions of 4 x-ray line markers embedded in the polyetheretherketone cage are useful indicators for predicting the ARA of the cage during cage insertion. (A) Three x-ray line markers indicate orthogonal insertion to the transverse axis of the disc (ARA: 0°). (B) Four x-ray line markers spaced every third of the AP diameter of the cage indicate 7° to 9° of axial rotation depending on the cage width (an actual ARA: –7°). (C) Two x-ray line markers indicate 15° to 19° of axial rotation (an actual ARA: –15°). Abbreviations: ARA, axial rotation angle; CT, computed tomography; PCA, potential contact area; XP, x-ray photography.







Tables
Demographic Value Sex, n, men/women 54/76 Age, y, mean ± SD (range) 72 ± 9.2 (44–90) Pathologies, n Degenerative lumbar scoliosis 46 Degenerative spondylolisthesis 42 LCS 40 LCS + VFx 2 No. of fused levels, mean ± SD (range) 1.7 ± 0.8 (1–3) Disk level, n L2/3 35 L3/4 72 L4/5 106 L5/6 2 Cage (Clydesdale PTC; 6° lordotic) Size, mm, mean ± SD (range) 49.8 ± 3.5 (45–55) Height, mm, mean ± SD (range) 10.3 ± 1.2 (8–14) Bone graft materials, n, cages/cases Decalcified bone matrix (Grafton︎) 198/120 Beta-tricalcium phosphate (AFFINOS︎) 17/10 Abbreviations: LCS, lumbar canal stenosis; VFx, vertbral fracture.
Demographic L2/3 L3/4 L4/5/6 All Disc Levels P No. of cages 35 72 108
(106: L4/5;
2: L5/6)215 AC/AP, mean ± SD (range) 41.1% ± 8.3%
(24%–63%)42.2% ± 7.8%
(24%–62%)41.2% ± 7.7%
(21%–63%)41.5% NS among 3 levels ≥50% 14.3% 16.7% 10.2% 13% NS among 3 levels ≥60% 2.9% 2.8% 0.9% 1.9% ARA, mean ± SD (range), ° 1.7 ± 6.6(−14 to 14) 1-.9 ± 5.8(−16 to 14) -4 ± 4.7*(−16 to 5) −2.9° <0.05 for L4/5/6
vs L2/3, L3/4≤−10° 11.4% 11.1% 13.9% 12.6% NS among 3 levels Cages installed in PCA,a b n/N (%) 1/35 (2.9%) 6/72 (8.3%) 6/108 (5.6%) 13/215 (6%) contact (−) ○ 0/1 1/6 0/6 1/13 p/o contact ▲ 0/1 5/6 4/6 9/13 contact (+) ● 1/1 0/6 2/6 3/13 Symptomatic radiculopathy (+) 0/1 0/6 2/6 2/13 RC/RL value 48.4% ± 3.1% (42.2%–52.4%) R-cage tip, mm −0.5 ± 3.1 (−5 to 7) CW/RL value 93.8% ± 6.1% (78.8%–100%) Abbreviations: AC/AP value, (anterior endplate edge–cage center/anterior–posterior endplate edge) x100 %; ARA, axial rotation angle (°); CW/RL value, cage width/right-left endplate edge x100 %; NS, not significant; PCA, potential contact area; p/o, possibility of; R-cage, right endplate edge-cage; RC/RL, right endplate edge-cage center/right-left endplate edge.
↵a Definitions of PCA: (1) AC/AP value ≥50% and ARA ≤ –10° (area A). (2) AC/AP value ≥60% and ARA ≤ –0° (area B). (3) Transition area between areas A and B,
↵b Contact (–): no chance of contact between the cage and the nerve; p/o contact: the possibility of contact between the cage/tools and the nerve; contact (+): direct contact between the cage and the nerve,
c Analysis of 13 cages in PCA.
Sex n Mean ± SD (Range) AP Diameter, mm RL Diameter, mm AP/RL Ratio, mm L2 endplate (L2/3) Men 10 35.4 ± 2.9 (30–40) 49.2 ± 2.1 (46–53) 0.72 ± 0.06 (0.62–0.8) Women 10 33.4 ± 2.6 (30–38) 46.6 ± 4.6 (40–53) 0.72 ± 0.05 (0.64–0.84) P (men vs women) NS NS NS L3 endplate (L3/4) Men 10 34.7 ± 2.0 (32–37) 50.3 ± 2.2 (47–52) 0.69 ± 0.05 (0.6–0.77) Women 17 33.2 ± 2.7 (30–38) 47.2 ± 4.4 (40–55) 0.70 ± 0.08 (0.62–0.93) P (men vs women) NS <0.05 NS L4 endplate (L4/5) Men 8 33.8 ± 2.3 (32–38) 52.6 ± 2.6 (48–55) 0.64 ± 0.05 (0.58–0.71) Women 19 32.5 ± 2.1 (30–37) 49.2 ± 3.4 (43–58) 0.66 ± 0.04 (0.6–0.73) P (men vs women) NS <0.05 NS L5 endplate (L5/6,L5/S1) Men 28 34.7 ± 2.4 (30–40) 50.6 ± 2.6 (46–55) 0.69 ± 0.01 (0.58–0.8) Women 46 33.0 ± 2.4 (30–38) 47.9 ± 4.1 (40–58) 0.69 ± 0.01 (0.6–0.93) P (men vs women) <0.01 <0.01 NS Total 74 33.6 ± 2.5 (30–40) 48.9 ± 3.9 (40–58) 0.69 ± 0.06 (0.58–0.93) P (disc levels) NS Men: <0.05
Women: NS<0.05 Abbreviations: AP, anteroposterior; NS, not significant; RL, lateral.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.