


Abstract
Background Robotic platforms have increased in sophistication for pedicle screw placement. Here, we review our institutional experience using ExcelsiusGPS to assess the accuracy rate of pedicle screw placement throughout the spine and characterize predictors of placement inaccuracy.
Study Design Retrospective cohort study.
Methods Patients from 2017 to 2022 undergoing spinal fusion surgery with ExelsiusGPS-assisted screw implantation at a single tertiary center were retrospectively identified. Patient demographics, preoperative symptoms, and operative details were collected. Postoperative computed tomography was used to classify screw placement accuracy according to the Gertzbein and Robbins scale (GRS). A stepwise multivariable ordered logistic regression analysis determined independent risk factors for clinically inaccurate screws (GRS C/D/E).
Results One hundred and seventeen patients were included. Mean age was 60.6 ± 13.2 years, with 57% men, 72% white, and mean body mass index of 29.9 ± 6.4 kg/m2. Seven hundred and twenty-eight screws were placed, predominantly in the thoracic (29.5%) and lumbar (52.6%) regions. Accuracy classification indicated 670 GRS A, 31 GRS B, 22 GRS C, 4 GRS D, and 1 GRS E screws. The clinically acceptable screw placement rate (GRS A/B) was 96%. Male gender (odds ratio [OR]: 2.12, P = 0.03), revision surgery (OR: 2.43, P = 0.02), and thoracic level screw insertion (OR: 2.33, P = 0.01) were independently associated with inaccurate screw placement and explained 8.7% of the variability seen. Of the 728 screws placed, 3 required revision after postoperative imaging revealed loosening or pedicle breach.
Conclusion ExcelsiusGPS-assisted screw insertion has high placement accuracy and low revision rates. Identification of predictors of inaccuracy illustrates that similar variables, such as placement in the thoracic spine and revision surgery status, apply to both freehand and robotic screw placement.
Clinical Relevance Robotic spine surgery is an accurate, reliable tool that can improve patient outcomes. Factors like male gender, thoracic screw placement, and revision surgery status are associated with lower screw placement accuracy, and these factors should inform surgical decision-making when using robotic assistance.
Level of Evidence 4.
Introduction
Novel robotic platforms have emerged for spine surgery that incorporate intraoperative navigation to facilitate placement of pedicle screws, which stabilize the bony spine.1 Advances in real-time instrumentation localization, intraoperative imaging, and independent navigation have improved the precision and user efficiency of these platforms.2 Advocates of robotic spine surgery note a reduction in radiation exposure, operational costs, and revision rates compared with freehand pedicle screw placement, arguing that these benefits outweigh potential learning curves and technological difficulties.3 Investigation of the accuracy of pedicle screw placement compared with freehand techniques is of substantial importance given that inaccurate placement can lead to devastating complications including dural lacerations, vascular injury, and compression of neural elements.4
Currently, several robotic platforms are commercially available, and screw placement accuracy rates have been reported to exceed those achieved with traditional modalities.5 Nonetheless, disparities exist in the characterization of precision among these systems. Platforms that were commercialized early, such as the Mazor SpineAssist and Renaissance robots, have been extensively studied, and high accuracy rates have been noted.6 Fewer studies have investigated the ExcelsiusGPS robot (Globus Medical, Inc., Audubon, PA), which received Food and Drug Administration approval in 2017. The ExcelsiusGPS system is notable for its real-time image guidance, 2-source tracking, and use of fiducial arrays and surveillance markers placed on the patient, avoiding the need for interspinous clamps and K-wires.7
Additionally, although high accuracy rates have been reported, risk factors for inaccurate placement using robotic systems are relatively uncharacterized. Identification of risk factors can improve value-based care, patient counseling, and preoperative planning, as well as inform patient selection and procedure workflow decisions for surgeons who lack experience with their robotic platform. In the present study, we sought to determine the pedicle screw placement accuracy of spinal surgeries utilizing the ExcelsiusGPS robot and identify predictors of unsatisfactory screw insertion.
Materials and Methods
Surgical System and Procedure
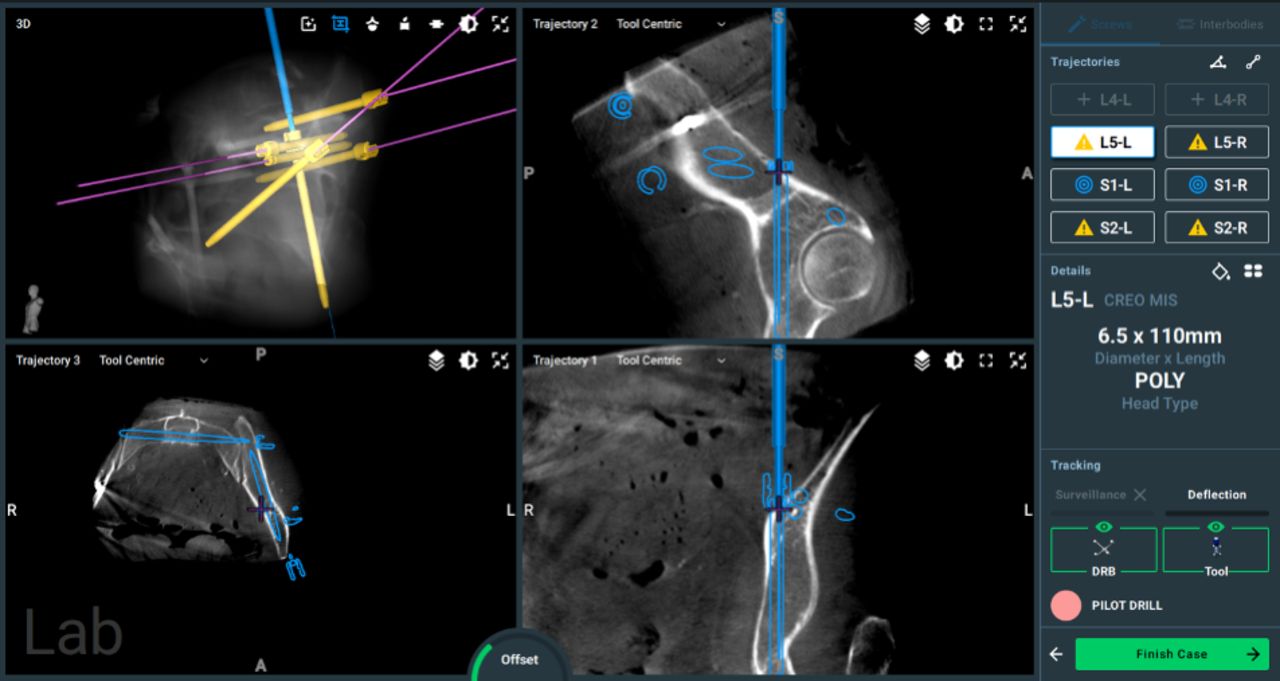
Preoperative computed tomography (CT) images are obtained and aligned with reference markers placed along the bony spine and surgical field. Intraoperative radiographs are obtained and registered to the preoperative imaging. Screw insertion trajectory is planned on the robot, allowing for manipulation of screw dimensions and entry points (Figure 1). Following registration of tools, the appropriate incision and dissection are carried out, and the robotic arm positions itself over the relevant spinal level for screw insertion based on the planned trajectory. Intraoperative monitoring occurs throughout the procedure to facilitate real-time anatomy and screw placement visualization.

Preoperative pedicle screw trajectory planning at L5 using the ExcelsiusGPS software. The upper left quadrant contains a visual representation of the screw’s placement. The remaining quadrants show the screw’s position from 3 planes of view.
Study Design
The medical records of all patients undergoing pedicle screw insertion with robotic guidance from October 2017 to March 2022 at a single tertiary care institution were retrospectively reviewed. All surgeries were performed by 1 of 3 fellowship-trained attending neurosurgeons. Patients lacking postoperative CT imaging were excluded, as postoperative imaging is required to determine screw accuracy. Patient demographics, diagnosis, operative course, and 30-day postoperative complications were collected. Any 30-day complications that existed prior to surgery were excluded. The main outcome examined was the accuracy of screw insertion, as measured by the Gertzbein and Robbins scale (GRS): A, completely within the pedicle; B, breach <2 mm; C, breach ≥2 mm and <4 mm; D, breach ≥4 mm and <6 mm; E, breach ≥6 mm (Figure 2). Under the GRS classification, screws are accurate if Grades A or B. Screw accuracy was independently graded by 2 authors (M.B. and K.J.) based on postoperative CT images, and disagreements were resolved by a third author (C.W.L.). This study was approved by the Institutional Review Board at Johns Hopkins University (IRB00265490), and patient consent was not required. Strengthening the Reporting of Observational Studies in Epidemiology guidelines were followed.

Gertzbein and Robbins scale (GRS) classification scores are shown on representative computed tomography images; yellow dotted lines indicate the border of the pedicle, and yellow arrows show the distance from screw to pedicle. (A) Grade A, the screw is located completely within the pedicle. (B) Grade B, the screw is mostly within the pedicle, with a slight <2 mm deviation. (C) Grade C, the screw has a pedicle cortical breach of 2 to 4 mm. (D) Grade D, the screw has a 4 to 6 mm pedicle cortical breach. (E) Grade E, the screw is deviated more than 6 mm from the optimal trajectory.
Statistical Analysis
All data were analyzed using Stata version 17.0 (StataCorp LLC, College Station, Texas). Numerical and continuous data are reported as mean ± SD, while categorical and dichotomous data are reported as proportions. Univariable analyses were performed using the Mann-Whitney U test for continuous variables, Fisher exact tests for dichotomous variables, and χ² tests for categorical and ordinal variables. Variables significant at the P < 0.10 level on univariable analysis were entered into a stepwise multivariable ordered logistic regression model to identify independent predictive factors of clinically inaccurate screw placement. The Brant test was used to confirm the proportional odds/parallel line assumption needed for an ordered logistic model. A P value < 0.05 was considered statistically significant.
Results
A total of 312 patients underwent pedicle screw insertion under robotic guidance from 2017 to 2022, of whom 117 patients were deemed eligible for inclusion in this study due to available postoperative CT images. These patients had a mean age of 60.6 ± 13.2 years (Table 1). More than half of patients (57%) were men, and the main indications for surgery were spondylolisthesis in 56 cases (48%), fracture in 12 cases (10%), spondylosis in 12 cases (10%), and pseudarthrosis in 12 cases (10%).
Demographics and preoperative parameters for 117 patients undergoing robotic spine surgery.
A total of 728 screws were placed in these patients, consisting of 55 (7.6%) in the cervical regions, 215 (30%) in the thoracic regions, 383 (53%) in the lumbar regions, and 75 (10%) in the sacral regions (Table 2). The average number of spinal levels operated on was 3 ± 2 (range 1–11), and 35 procedures (30%) were revision surgeries. The vast majority of cases (97%) used a posterior approach, with a mix of midline (47%) or paramedian (38%) incisions performed.
Operative and postoperative parameters for 117 patients undergoing robotic spine surgery.
The mean estimated blood loss was 363 ± 569 mL, incision-to-extubation time was 222 ± 90.2 minutes, and length of stay was 5.8 ± 7.6 days. Reoperations were performed in 23 (20%) cases, with the main indications being extension of fusion in 6 (5.1%) cases, wound dehiscence in 5 (4.3%) cases, and hardware failure in 4 (3.4%) cases. The complication rate was 11% and included wound infections (5.1%) and cerebrospinal fluid leak (5.1%).
Classification of screws using the GRS system included 670 (92%) screws as GRS A, 31 (4.3%) as GRS B, 22 (3.0%) as GRS C, 4 (0.5%) as GRS D, and 1 (0.1%) as GRS E (Table 3). A total of 701 (96%) screws were deemed clinically acceptable using the conventional metric of a GRS A or B score. Of the 728 screws placed, only 3 (0.4%) required revisions. Two of these screws were revised postoperatively in a patient who experienced numbness and weakness following a T4-ilium fusion surgery for degenerative scoliosis (Table 4). Postoperative imaging in this individual revealed that the right-sided screws at L3 and L5 deviated medially from the optimal trajectory. Another patient underwent a T12 to L2 fusion for an unstable L1 fracture, and the T12 screw was found to have deviated laterally from the optimal trajectory during intraoperative O-arm imaging. This screw was noted and revised immediately with a more medial planned trajectory, ensuring better bony purchase in the posterior spine. All 3 revised screws were graded as GRS A on postoperative imaging.
GRS score and number of screws per vertebral level.
Patients with pedicle screw breach who underwent revision of malpositioned hardware.
Predictors of Accuracy
A stepwise ordered logistic regression model was performed to identify predictors of screw accuracy (Table 5). Univariable analysis showed that predictors of inaccurate screw placement included male gender (P = 0.03), a preoperative diagnosis of spondylolisthesis (P = 0.01) or pseudarthrosis (P = 0.02), revision surgery (P < 0.01), thoracic level (P < 0.01), number of screws placed in the patient (P < 0.01), and incision-to-extubation time (P = 0.03). Independent risk factors associated with inaccurate screw placement identified from the multivariable ordered logistic regression model included male gender (odds ratio [OR]: 2.12, P = 0.03), revision surgery (OR: 2.43, P = 0.02), and thoracic level screw insertion (OR: 2.33, P = 0.01). A Brant test was performed and yielded no significance, confirming that the proportional odds assumption was met. The coefficient of determination (R 2) was low, with a value of 0.087.
Stepwise multivariate ordinal logistic regression model of preoperative and surgical variables associated with pedicle screw accuracy.
Discussion
Over the past 2 decades, advances in image guidance and spinal navigation have contributed to the development of robotic platforms for spine surgery. The most widespread and well-studied application of robotics in this field is pedicle screw insertion.8 Although both traditional and robot-navigated methods of screw placement report high levels of accuracy, the latter has lower rates of pedicle breaches, shorter hospitalization stays, less radiation exposure, and higher proportions of clinically accurate screw placement.9,10 Nonetheless, there may be variation in accuracy among robotic platforms, especially given the imbalance in published institutional experience between older and newer systems. Furthermore, risk factors for inaccuracy among all robotic platforms are understudied. Therefore, we present our institutional experience with 117 cases of ExcelsiusGPS-assisted pedicle screw placement and analyze the effect of patient and operative factors on accuracy. With the ExcelsiusGPS robotic platform, a 96% screw insertion accuracy rate was observed with a 0.4% screw revision rate among patients with postoperative CT images. We found that male gender, revision surgery status, and screw placement in the thoracic spine are significant independent factors of screw placement accuracy.
Accuracy of pedicle screw placement has been an important and clinically relevant topic for spine surgeons since the inception of this procedure. Several retrospective studies indicate 90% and higher accuracy rates of screw positioning under multiple modalities, with comparative studies indicating slightly higher rates for CT navigation and robotic assistance.5,11 Stealth navigation achieved 99.3% screw placement accuracy in patients with congenital deformity and altered anatomy, while augmented reality surgical navigation has shown 93.1% clinically accurate screw placement.12,13 Our systematic review on the accuracy of pedicle screw placement revealed a 93.1% optimally placed screw rate with a freehand technique. Adding image guidance, however, increased this rate to 95.5%. Using robot assistance lowered the breach rate from 12.1% with freehand to 0.8%.14 The literature indicates that this accuracy varies based on the commercial robotic platform used. Peng and colleagues conducted randomized controlled trials between TiRobot, SpineAssist, and Renaissance systems and found only TiRobot to be superior when compared with conventional freehand surgery.15 A meta-analysis comparing older and newer generation robots indicated that the former has screw placement accuracy rates around 97%, while the latter reaches 99%.6 Reported initial experiences with ExcelsiusGPS indicate similarly high levels of screw placement accuracy with low breach rates.16 Our institutional experience mirrors this work. Two of our first operative cases using ExcelsiusGPS showed the accurate placement of 8 pedicle screws with no postoperative deficits or screw revision needed.17 We further evaluated screw accuracy based on deviation from planned trajectory as well as GRS and showed a 100% clinically acceptable placement rate of 254 screws in 47 patients.18
In the present study, we expanded the sample size and identify a similarly high screw placement accuracy rate and a low overall screw revision rate. Of the 728 screws placed in 117 patients, only 3 screws required revision due to significant pedicle breaches. One of these screws was identified and fixed intraoperatively when O-arm imaging revealed a lateral deviation. Therefore, intraoperative imaging in conjunction with robotic assistance can help improve screw placement by offering continuous validation of instrumentation positioning during the procedure.19
Risk Factors for Screw Malposition
Identification of predictors of adverse outcomes in spine surgery can improve value-based care, patient counseling, and preoperative planning.20 Yi et al measured deviations between planned and actual screw trajectories using the TINAVI system, which is not approved for use in the United States.21 They found that neither cortical bone trajectory nor pedicle screw placement affects accuracy, but right-sided screw placement, larger lamina angles, larger screw diameters, and greater distance from the tracker are risk factors for screw deviation from the preplanned path. Zhang and colleagues compared satisfactory and unsatisfactory screws placed with the Mazor Renaissance robot and found that obesity, osteoporosis, vertebral rotation, and the presence of congenital scoliosis were independent risk factors for inaccuracy.22 A study by Toossi et al on the ExcelsiusGPS system found that patient age, gender, length of construct, screw diameter, and screw length influenced overall accuracy; however, these factors were minor determinants of overall accuracy, similar to our study.23 The low coefficient of determination in our analysis indicates that the risk factors identified in the present study do not account for considerable variation away from the accuracy of the platform.
The only patient factor in our study significantly associated with screw inaccuracy was male gender. Interestingly, Toossi et al found the opposite effect with ExcelsiusGPS, with more screw offsets and pedicle breaches noted in women, which they attributed to higher rates of osteoporosis in postmenopausal women.23 Furthermore, although Zhang et al identified osteoporosis as a risk factor for unsatisfactory screw placement with Renaissance, they did not find female gender to be significant.22 Although our study findings diverge from those of Toossi et al, the overall rate of screw inaccuracy was low in our study, suggesting that the contribution of gender may not necessarily be clinically significant.
Thoracic screw placement and revision surgery status were also noted as independent factors influencing ExcelsiusGPS-assisted screw accuracy. Higher levels of misplacement have been reported for the thoracic spine compared with the lumbar spine using conventional nonrobotic techniques, in part attributable to the complex anatomy of the thoracic spine and smaller sizes of the pedicles.24 The middle thoracic levels in particular have narrow pedicles and require smaller screws than other regions. Indeed, a prior review of 9,179 pedicle screws placed at our institution using freehand techniques also identified thoracic screw placement as an independent risk factor for screw malposition and screw revision surgery.8
Similarly, the association of revision surgery status with screw malposition is not surprising, likely reflecting the increased complexity of revision surgeries. Ando et al found new freehand pedicle screws to have higher perforation rates in the thoracic and lumbar spine if they were of a larger diameter than the prior screw.25 Therefore, several methods have been suggested to improve pedicle instrumentation revision. For example, Matheus et al reported a case of ExcelsiusGPS-assisted pedicle stacking, in which a second set of screws are placed at a previously instrumented level without removing the old screws. This technique reduced operative time without causing any postoperative complications and may represent a new avenue for stereotactic robotic guidance.26
Limitations
The results of this retrospective study reflect the experience of a single institution and fellowship-trained spine surgeons. The most significant limitation is that only patients with postoperative CT images were included, as a CT is needed in order to assess the accuracy of screw placement using the GRS classification system. Our institution transitioned from postoperative CT images to postoperative x-rays for verification of screw position after surgeons gained mastery of the robotic system and demonstrated consistently high screw placement accuracy rates. An analysis of the learning curve associated with ExcelsiusGPS in our institution indicated that general proficiency is observed after the 20th case and mastery achieved after the 67th case.27
Postoperative CT was ordered only after mastery was achieved if the following concerns were present: misplaced instrumentation, suspected screw malpositioning, new or worsening radiculopathy, suspicious findings on postoperative x-ray imaging, persistent or new onset pain, or other neurological process. As a result, there were no patients who required a screw revision that did not also have a postoperative CT image. Therefore, the actual accuracy of the ExcelsiusGPS platform is likely higher than calculated in this study due to selection bias. Furthermore, the overall rarity of inaccurate screw placement may limit conclusions about risk factors of malposition. Future multicenter prospective studies can improve external validation. Nonetheless, the study serves as a retrospective review of our experience with robotic-assisted pedicle screw placement, and findings are comparable to other studies showing improved accuracy rates using robotic platforms compared with freehand navigation.
Conclusion
Our review of 728 pedicle screws placed in 177 patients throughout the cervical, thoracic, and lumbar spine illustrate the safety of robotic-assisted pedicle screw placement. High levels of screw accuracy (96.3%) and a low rate of screw revision (0.4%) were noted. These accuracy rates exceed the reported literature on freehand techniques. Identification of predictors of screw inaccuracy, such as thoracic screw placement and revision surgery status, illustrates that similar considerations apply to both freehand and robotic screw placement.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Nicholas Theodore receives royalties from and owns stock in Globus Medical. He is a consultant for Globus Medical and has served on scientific advisory board/other office for Globus Medical. The remaining authors have no conflicts of interest to disclose.
Previous Presentation AANS/CNS Joint Section on Disorders of the Spine and Peripheral Nerves Annual Meeting, on 16 to 19 March 2023, as an I-Presentation.
- Revision received September 2, 2024.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.