


Abstract
Background We sought to better understand the current decision-making criteria and surgical strategies for pelvic fixation in spinal surgery.
Methods A 28-question survey was distributed to an international group of practicing spine surgeons. Questions included training, practice type, criteria for using pelvic fixation, and strategies for pelvic fixation, including the type and technique employed.
Results Of the 56 responders, 32% were neurosurgeons, and 67% were affiliated with academic institutions. Factors that most influenced the use of pelvic fixation were 3-column osteotomy (3CO), high-grade spondylolisthesis, and L5 to S1 pseudarthrosis. Most report using a single point of pelvic fixation per side for the following: deformity 4+ levels without 3CO (55%) and spondylolisthesis grade 3 (59%). The upper instrumented vertebra threshold for pelvic fixation in degenerative pathology was L2 (70%) or L3 (16%). Most surgeons chose 2 points of fixation per side in the setting of 4 or more levels with 3CO (69%) and revision of at least 3 levels (68%). The predominant (77.6%) fixation preference was S2-alar-iliac screws. Surgeons report using navigation (70%), fluoroscopy (23%), free hand (21%), and robot-assisted (7%) for screw placement. The most common pelvic screw diameter and length were 8.5 mm and 90 mm, respectively. A 5% to 10% pelvic fixation revision rate was reported, primarily for instrumentation failure or pseudarthrosis.
Conclusion This survey-based study highlights factors influencing surgeons’ decisions on pelvic instrumentation. While complex corrections or revisions often require robust fixation, variability arises in simpler cases, influenced by factors like age, obesity, and bone quality.
Level of Evidence 4.
Introduction
Pelvic fixation is critical to spinal surgery, particularly in managing complex spinal deformities and high-grade spondylolisthesis. The evolution of fixation techniques has seen significant advancements, with the introduction of S2-alar-iliac (S2AI) screws providing a stable and reliable method of achieving pelvic fixation. Traditional iliac screws have been associated with higher rates of implant prominence and complications, necessitating the development of lower profile and more biomechanically advantageous techniques.1,2 The increasing use of S2AI screws among spine surgeons highlights their effectiveness in providing stable fixation, particularly in complex cases involving deformity corrections and high-grade spondylolisthesis.1 Studies have demonstrated that S2AI screws provide superior biomechanical stability and lower rates of implant prominence compared with traditional iliac screws, offering advantages such as easier insertion, reduced need for rod contouring, and lower risk of screw loosening and prominence.3,4 Additionally, 1 study found S2AI screws were associated with a significantly lower rate of surgical site infections (2.2% vs 23.5%).5
Spine surgeons choice of pelvic fixation strategy is widely heterogeneous. Influencing factors include deformity severity, spondylolisthesis grade, age, body mass index, bone quality, and pseudarthrosis.1 Understanding current trends and preferences in spinopelvic fixation can provide valuable insights into optimizing surgical outcomes and guide future research and development.
The current study investigated current trends and preferences in lumbosacral-pelvic fixation among spine surgeons in North America and Europe. Through a cross-sectional survey, we sought to better understand the current decision-making criteria and surgical strategies utilized by spine surgeons regarding pelvic fixation in both degenerative and deformity surgery in the following areas: factors influencing the decision to perform pelvic fixation and the type and technique of pelvic fixation. By addressing these objectives, this study aims to provide an overview of current practices in spinopelvic fixation and identify areas for future research and innovation.
Methods
Study Design and Setting
The Spinopelvic Study Group (SPSG) conducted an international, cross-sectional survey to gather detailed information on current pelvic fixation practices among spine surgeons. The survey was distributed electronically via a secure, web-based platform to a global network of practicing orthopedic and neurosurgery spine surgeons.
The survey instrument consisted of 28 multiple-choice questions structured to capture comprehensive data on various aspects of spinopelvic fixation. Surgeon demographic information included residency training (orthopedic or neurosurgery), subspecialty training (eg, spine fellowship), and current practice setting or practice type (academic, private, or public hospital). Several questions surrounding indications for spinopelvic fixation were asked, including deformity severity, spondylolisthesis grade, and the presence of pseudarthrosis. Spinopelvic fixation method choices were sacro-alar-iliac (SAI; starting point on the sacrum), modified iliac (low start on the posterior superior iliac spine), and traditional iliac (starting point on the posterior superior iliac spine). Imaging modality choices were navigation, fluoroscopy, robot-assisted, and free hand.
Survey Administration
All members of the SPSG completed the survey. Additional spine surgeons were recruited through SPSG member contacts including colleagues, partners, and members of various international spine societies across a wide variety of spine pathology, including the Lumbar Spine Research Society, Congress of Neurological Surgeons, Scoliosis Research Society, American Academy of Neurological Surgery. Participation was voluntary and anonymous. An independent observer oversaw the data collection process to ensure the impartiality of the responses.
Data Collection and Analysis
Responses were collected over a 3-month period. Data were anonymized and stored securely. Descriptive statistics were calculated for all variables.
Results
The survey was completed by 56 surgeons; 68% of respondents identified as orthopedic surgeons, 32% as neurosurgeons, and 96% of all respondents completed a spine fellowship. Practice location was skewed toward academic based at 67% of respondents, 14% are in private practice, and 18% are hospital based. Survey respondents reflected broad society membership.
Factors Influencing Decision to Perform Pelvic Fixation
Key factors influencing the use of pelvic fixation included 3-column osteotomies (3CO; 14%), high-grade spondylolisthesis (13%), and L5 to S1 pseudarthrosis (12%). In cases of degenerative pathology, the upper instrumented vertebrae (UIV) threshold for pelvic fixation was L2 in 70% of cases, L3 in 16%, and the lower thoracic region in 11%.
Type of Pelvic Fixation
For deformity cases involving 4 or more levels without a 3CO, 55% of surgeons chose 1 point of pelvic fixation per side. In contrast, for deformities with 3CO, 69% opted for 2 fixation points per side. For high-grade spondylolisthesis (grade ≥3), 59% of responding surgeons used 1 point of pelvic fixation per side.
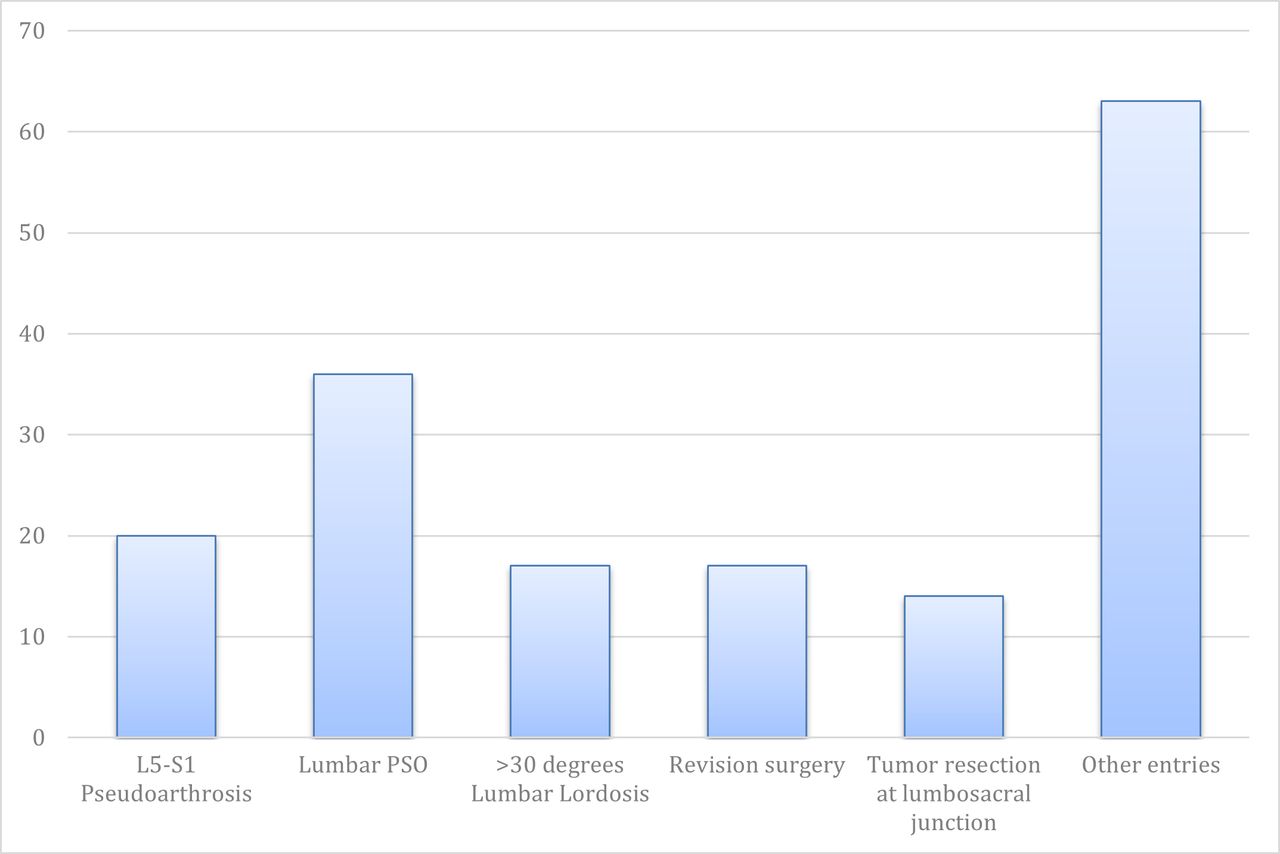
Conditions prompting the use of more than 2 rods across the lumbosacral junction included high-grade spondylolisthesis, lumbar pedicle subtraction osteotomy, L5 to S1 pseudarthrosis, and correction of lumbar lordosis greater than 30° (Figure 1).

Conditions for use of 2 or more rods across the lumbosacral junction.
The method of preferred fixation was SAI screws, used by 77.6% of surgeons. The most common screw diameters were 8.5 and 10.5 mm, used by 29% and 24% of surgeons, respectively. The most common screw length was 90 mm (59%). For 2 points of pelvic fixation bilaterally, 27% of surgeons preferred 2 SAI screws per side, while 16% preferred to use an iliac and an SAI screw per side (Figure 2 shows stacked SAI screws). Navigation was the most common modality for placing pelvic fixation (70%), followed by fluoroscopy (23%), free-hand methods (21%), and robot assistance (7%). The need for pelvic fixation revision among surveyed surgeons was approximately 5% to 10%, with the most common reasons being instrumentation failure and pseudarthrosis.

Stacked sacro-alar-iliac pelvic fixation, consisting of S1-alar-iliac and S2-alar-iliac screws with 4 rods across the lumbosacral junction.
Discussion
Results of this survey show that while there is considerable variation in the method of pelvic fixation, there is relative consensus on when to instrument to the pelvis. Factors such as degree of deformity correction, 3CO, and instrumented arthrodesis extending cephalad or from L2 to the sacrum typically warrant pelvic fixation.
The predominant (77.6%) fixation preference in the survey was S2AI screws. This is most likely attributed to the increasing body of evidence demonstrating the advantages of S2AI fixation over traditional iliac fixation. These advantages, which have been reported in the literature encompassing the adult and pediatric populations, include a statistically significant decrease in gluteal pain, revision surgery, acute infections, implant loosening, and delayed wound infections.5–8 The preference for S2AI screws underscores their reliability in providing stable fixation and a lower reoperation rate, compared with traditional iliac fixation, particularly in complex deformity case corrections.9 S2AI screw fixation is associated with fewer clinical and radiographic complications in the adult and pediatric populations vs traditional iliac screw fixation techniques.6
Number of Pelvic Fixation Points per Side
Most surgeons chose 2 points of fixation per side in the setting of fusion of 4 or more levels with 3CO (69%) or revision of 3 or more levels (68%). The number of pelvic fixation points per side was dependent on the reason for surgery (ie, deformity, trauma, degenerative, tumor, and infection). This is an area that remains poorly studied, and the consensus on surgical technique is lacking. The lumbosacral junction acts as the foundation in long spinal constructs undergoing extensive strain forces after surgery.10–12 The goal of pelvic fixation is to ameliorate this problem, provide a solid foundation for the cephalad portion of the spinal instrumentation, and improve fusion rates across the lumbosacral junction. Nevertheless, pelvic fixation failure with S2AI and traditional iliac techniques is not uncommon.13,14 In a multicenter retrospective review, a 5% acute failure rate was reported.15 Therefore, there has been increasing interest within the spinal deformity community on how to avoid failures and prevent a return to the operating room. Multiple points of pelvic fixation have been proposed in the literature to solve this problem. However, clinical evidence is still lacking as to whether this improves acute failure rates.
Pelvic Screw Fixation Characteristics
The survey identified 8.5 mm and 10.5 mm as the most common pelvic screw diameters, with 90 mm as the preferred screw length employed during pelvic fixation. McCord et al demonstrated that the biomechanical advantage of performing iliac fixation resides in passing the middle column’s pivot point and the length factor of the screw in the cancellous bone of the ilium.16 The L5 to S1 junction is immobilized through the middle of the L5 to S1 disc space based on the length of the iliac screw serving as a lever arm.17 Some have suggested that screws with a longer position within the ilium may reduce the likelihood of screw loosening in the cancellous bed.7,16 Unlike traditional iliac screws that pass through 1 cortical zone and reside in a cancellous bone bed, SAI screws have cortical purchase in the sacrum and the ilium, crossing the SI joint.17–19 O’Brien et al showed that longer is not better when it comes to SAI fixation; 65 mm screws were not biomechanically inferior to 80 mm SAI screws or 90 mm iliac screws.17 However, Santos et al contradicted this by showing that the critical factor is not the trajectory itself but the extent to which the screw engages the cortical bone, which is responsible for generating higher insertional torques.20 The lack of increased insertional torque at depths under 80 mm is due to the iliac wing’s width, limiting lateral cortical bone engagement. This highlights screw depth and size as more critical to fixation strength than trajectory, with larger, longer screws better engaging cortical bone.20 In terms of width, Martin et al demonstrated that when diameters of less than 8.5 mm were used, there was an increased early failure rate in pelvic fixation.21
UIV Threshold for Pelvic Fixation
The survey showed that the UIV for which surgeons would most frequently employ pelvic fixation is L2 or above (70% of the time) followed by L3 or above (16% of the time). In long-segment fusions, the forces acting on the lower part of the spine, particularly the lumbosacral junction (L5–S1), are significantly increased. Without pelvic fixation, there is a higher risk of implant failure, loosening of S1 screws, and loss of alignment at the lumbosacral junction.22 Pelvic fixation provides additional support by anchoring the spine to the pelvis, potentially preventing complications like pseudarthrosis and instrumentation failure.1,23 An ideal lumbosacral construct should withstand large loads before failing and maintain strain within an optimum range of 2% to 10%.16 While there are studies in the spine deformity literature that demonstrate the biomechanical advantages of pelvic fixation in long thoracolumbar fusion constructs vs sacral fixation.16,24,25 Evidence from the literature for the implementation of pelvic fixation when treating degenerative processes, without high-grade (>3) spondylolisthesis, sagittal/coronal deformity, trauma, tumor, pseudarthrosis, infection, or revision procedures is lacking. Long fusions that terminate in the sacrum alone, consisting of bicortical screws, can undergo failure as high as 44%.7,22,26,27 Biomechanically, SAI screw placement has advantages over standard S1 fixation in reducing sacroiliac joint motion.25 SAI screws minimize the strain on spinal rods by offering a more direct connection between the spine and pelvis, reducing the likelihood of rod breakage or instrumentation failure.18,28 Because they engage the pelvis directly, SAI screws allow for better load sharing across the spinal construct, reducing stress at the lumbosacral junction. This improves fusion rates and reduces the risk of pseudarthrosis, which is more common when using S1 screws alone in long fusions.18,29
Factors Influencing the Decision to Perform Pelvic Fixation
According to our survey, the most common indications for pelvic fixation include deformity correction involving 4 or more levels and high-grade spondylolisthesis (greater than or equal to grade 3). These answers are commensurate with the literature.18,23,30 A widely accepted indication for sacropelvic fixation is a long thoracolumbar-sacral fusion involving 5 or more levels that end at the sacrum.31 Biomechanical evidence suggests that in instrumented fusions extending above L3, sacral screws should ideally be reinforced with supplemental iliac screws or additional spinopelvic fixation.31,32 Due to its exceptional fixation strength when properly executed, pelvic screws can provide essential foundational support to assist in spondylolisthesis reduction by reducing the shear forces on sacral screws during fusion maturation.23 Additional considerations for pelvic fixation in the surgical planning phase include treatment of spine tumors, pelvic trauma, or infectious processes involving the pelvis.8,33–35 Spinopelvic fixation is also indicated for correcting lumbar deformity and pelvic obliquity, particularly in children with neuromuscular deformities. Anchoring only in the sacrum often fails to provide and sustain the required correction, as it relies on shorter screws and limited fixation within the sparse trabecular bone, rather than the more secure cortical confinement available in the ilium.30,36,37 Low sacral bone quality and significant biomechanical stresses at the lumbosacral junction can lead to a high incidence of instrumentation-related complications along with sacral screw loosening.22,38 Implant failure at the distal extent of a multilevel construct anchored in the sacrum alone can lead to lumbar-sacral junction instability, leading to pseudarthrosis and screw loosening necessitating pelvic fixation.22,31,39
Multiple Points of Pelvic Fixation
The survey highlights the increasing use of multipoint pelvic fixation, with 41.5% of respondents employing this technique in 2022. Utilizing both multiple pelvic screws and a multi-rod construct can enhance the mechanical stability of the lumbosacral junction and decrease the stress on instrumentation, interbody cages, the S1 superior endplate, and the sacrum.40 Polly et al discuss a stacked SAI approach using 2 points of sacral-alar fixation on each side as a strategy to mitigate pelvic fixation failure.10 At the time this manuscript was written, there were no definitive studies analyzing the failure rate of multiple points of iliac or SAI fixation as compared to the previous pelvic failure data.
Navigation Utilization During Pelvic Fixation
The substantial use of navigation systems suggests a trend toward enhancing accuracy and safety in screw placement, which is essential in minimizing complications and improving clinical outcomes.41 In our survey, surgeons report using navigation (70%), fluoroscopy (23%), free hand (21%), and robot-assisted (7%) for screw placement. Matsukawa et al demonstrated the use of O-arm navigation for placing S2AI screws improves the accuracy of screw placement, reduces the likelihood of malposition, and increases safety by providing real-time imaging, particularly in patients with complex spinal deformities or compromised sacral anatomy.42 Navigation enhances the safety and accuracy of pelvic fixation by providing real-time, 3-dimensional imaging, which helps avoid critical neurovascular structures and ensures optimal screw placement, particularly in complex deformity cases.43,44
Despite the valuable insights provided by this survey, several limitations must be acknowledged. First, the survey data are based on self-reported information from spine surgeons, which may introduce bias and affect the accuracy of the reported practices and preferences. Most respondents were orthopedic surgeons and were affiliated with academic institutions. There may be differences in surgical preferences between specialties and practice settings. This is a survey and not a clinical study that tracks clinical outcome data, making the results observational without any clinically actionable suggestions. Additionally, the results do not account for variations in surgical technique, surgeon experience, or geographical location. It is unknown if the surgical approach (ie, minimally invasive vs open) influences the choice of pelvic fixation technique. Moreover, the survey did not ask surgeons to differentiate choices based on primary vs revision surgery.
Despite significant advancements in spinopelvic fixation techniques, further research is needed to address the remaining questions. Future studies should focus on the long-term outcomes of different pelvic fixation methods and constructs, particularly comparing the efficacy and complication rates of iliac screws vs S2AI screws across various patient populations.
Conclusion
This survey is an overview of the current trends and preferences in lumbosacral-pelvic fixation among a group of experienced spine surgeons who perform a variety of complex spine procedures in their practices. The predominant use of S2AI screws reflects their advantages in terms of stability and reduced complications. However, challenges such as instrumentation failure and pseudarthrosis remain prevalent in these surgeries. The ongoing difficulties necessitate further research and innovation in this field, focusing on long-term outcomes and the development of new techniques, proper patient selection, and improvement of instrumentation utilized for pelvic fixation to reduce complications and improve fusion rates.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Sohaib Hashmi reports consulting fees from ATEC, SI-BONE, and Medtronic. Elizabeth Lord reports consulting fees and support for attending meetings/travel from SI-BONE. Joshua Heller reports grants/contracts from Ethicon and Providence Medical Technology; royalties/licenses from Globus, Spinal Elements, and XTANT; consulting fees from ATEC, Globus, Providence Medical Technology, SI-BONE, Spinal Elements, Stryker, XTANT, and Highridge Medical; payment or honoraria from Providence Medical Technology and SI-BONE; support for attending meetings/travel from Providence Medical Technology, SI-BONE, and Spinal Elements; and personal stock in ATEC, SI-BONE, and Spine Biopharma. David Essig reports consulting fees from SI-BONE, DePuy, and Stryker, and support for attending meetings/travel from SI-BONE. Peter Passias reports support or grants from Globus, Medtronic, and Cerapedics; support for attending meetings/travel from SI-BONE; and serving in leadership roles for JNS Spine and Spine. Robyn Capobianco reports stock/stock options from SI-BONE and is an employee of SI-BONE. Christopher Kleck reports consulting fees from Medtronic, SI-BONE, Biocomposites, Allosource, SeaSpine, and Carlsmed, and research support as a primary investigator from Medtronic/Medicrea, SeaSpine, Medacta, Synergy, SI-BONE, Globus, and Personalized Spine Study Group. David Polly reports grants or contracts from SI-BONE, Medtronic, Globus, and AO Spine; royalties/licenses from SI-BONE; consulting fees from SI-BONE, Medtronic, and Globus; payment/honoraria from SI-BONE; patents (planned, issued, or pending) from SI-BONE; and a leadership role for the Minnesota Orthopedic Society. Scott Zuckerman reports consulting fees (less than $10,000) from NFL and Medtronic.
Ethics Approval This survey of surgeons does not include patient information, negating need for informed consent or IRB approval.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.