


Abstract
Background The number of spinal surgeries performed worldwide have significantly increased over the past decade. However, to the best of our knowledge, there are no national or international studies that report the overall picture of complications following spinal surgery. This article sought to identify the incidence and causes of reoperations in patients undergoing spinal surgery, as well as the average time from index surgery to reoperation. Furthermore, the purpose was to identify the microbiological agents present in cultures from infected patients.
Methods This was a retrospective cohort study that used a university hospital’s medical records as the data source. The study population comprised 2110 patients who underwent spinal surgery during a 40-month period between 2015 and 2018. All suspected reoperations were verified manually. Additional data collected for reoperations included cause, time from index surgery, and laboratory results from cultures. Descriptive analysis was used.
Results The incidence of reoperations during the study period was 11% (n = 232). The most common cause of reoperation was infection (28%, n = 65), followed by implant-related causes (19%, n = 44) and hemorrhage/hematoma (15%, n = 34). The time between index surgery and reoperation varied, but half of all reoperations occurred within 30 days. Coagulase-negative staphylococci were the most common type of bacteria (positive cultures in 39% of infected patients).
Conclusion The number of reoperations in the studied hospital were high during the study period. Infections accounted for a large percentage of reoperations, suggesting that effective preventive measures might significantly reduce the total number of reoperations.
Clinical Relevance Postoperative infection causing reoperations after spinal surgeries is a large problem, and finding effective preventive measures should be a priority for caregivers.
Level of Evidence 3.
INTRODUCTION
The number of spinal surgeries performed in Sweden have increased significantly during the past decade. For example, the numbers of lumbar spine surgeries almost doubled between 2007 (4932) and 2017 (9484).1,2 Adverse events in general are a major problem both globally and nationally.
Several Swedish studies of spinal surgery have reported a reoperation rate ranging from 5.4% to 27%, depending on the type of operation and the length of follow-up.3–6 However, the majority of these studies4–6 are based on data from the Swedish National Spine Register (Swespine) and might underestimate the number of reoperations. A study comparing Swespine with insurance claims found that only 65% of complications were registered in Swespine.7 Several other studies that investigated the long-term outcome after different types of spinal surgeries only reported if additional surgery had been performed but not the cause.8–10 To the best of our knowledge, there are no national or international studies that report the overall picture of complications following spinal surgery. As a result, a survey of complications in spinal surgery is needed.
The aim of the present study was to identify the incidence and causes of reoperations in patients who had previously undergone spinal surgery at a university hospital between 2015 and 2018. In addition, we wanted to delineate the average time difference between index surgery and reoperation, as well as the microbiological agents present in cultures from infected patients.
METHODS
This study is a retrospective analysis of medical records from 2015 through 2018. The university hospital’s internal patients’ medical records and the surgical planning program were used as a data source. The study conforms to the criteria issued by Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).11 The chosen definition of a reoperation in this study was that the operation was described or coded as a reoperation in the operation or discharge entry of the medical record.
Study Population
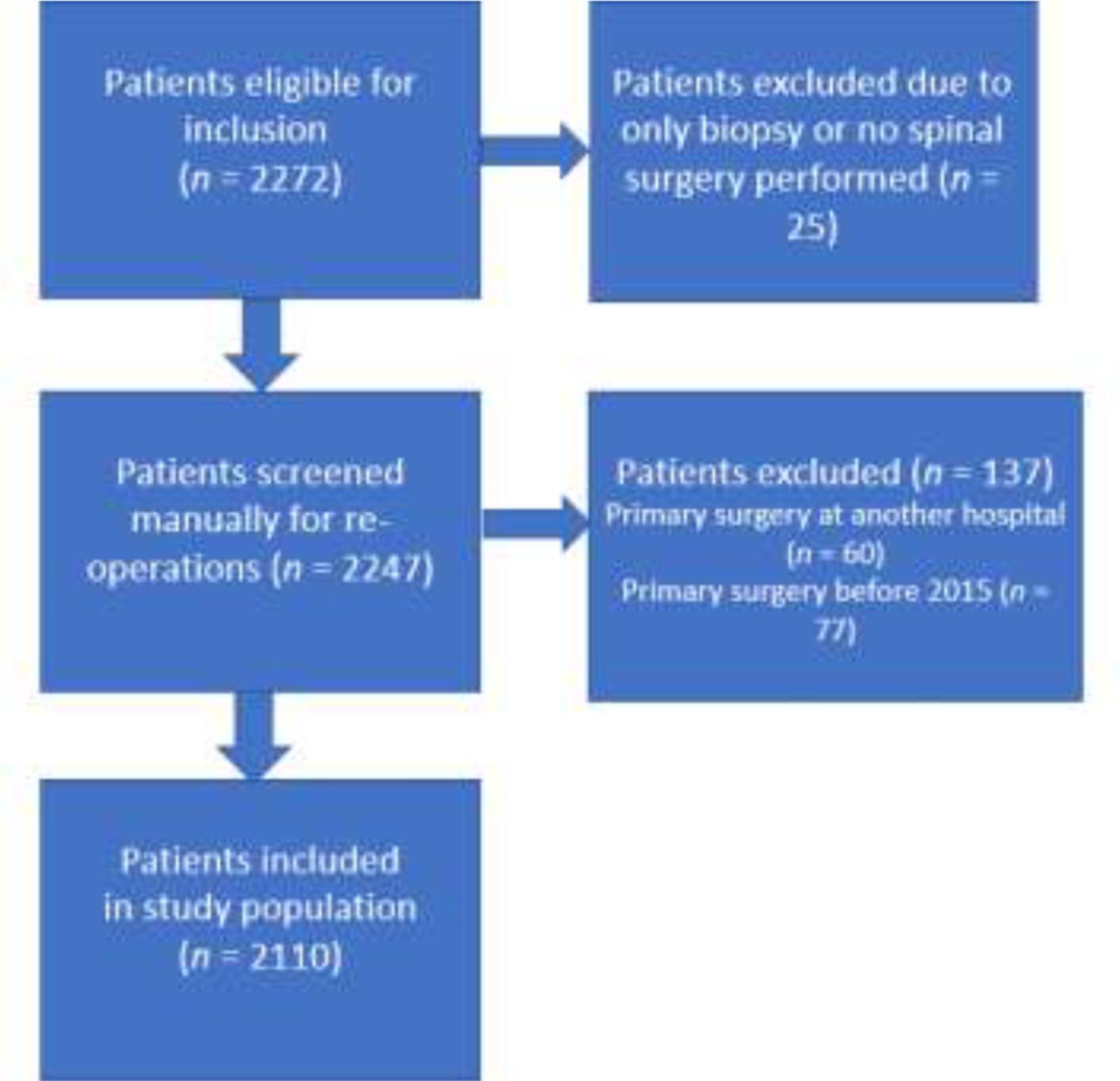
The study population comprised 2110 consecutive patients who underwent a primary surgery on the spine during the study period. The exclusion criteria were patients who underwent surgery on a different part of the body than the spine, who had a biopsy only, whose primary surgery took place at another hospital, or whose primary surgery took place before 2015. A flow chart of population selection is provided in the Figure.
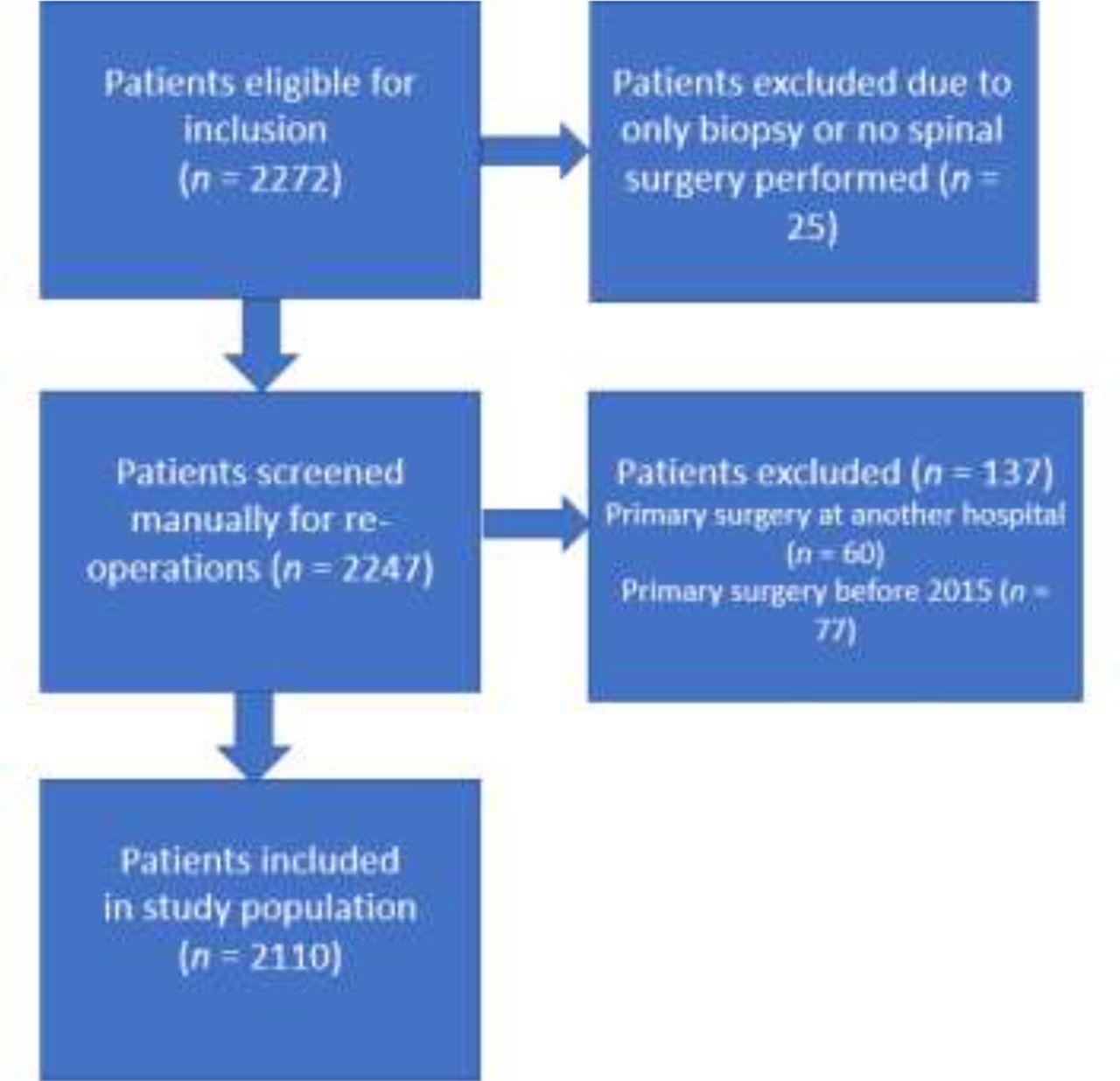
Preferred reporting items for systematic reviews and meta-analyses flow chart of population selection.
Variables and Data Extraction
The following variables were retrieved for the entire study population: age, gender, physiological status (according to the American Society of Anesthesiologists Physical Status Classification System), type of index surgery (following classification codes from the National Board of Health and Welfare in Sweden), date for index surgery, diagnosis (according to the International Classification of Diseases 10, by the World Health Organization), and operating time. For the few cases (n = 8) in which operating time was missing, this variable was estimated from the intraoperative anesthesia record.
During manual screening, 2 different research staff members separately verified suspected reoperations by reviewing the medical records of all patients (n = 369) who underwent more than 1 surgery during the study period, had a diagnosis representing a complication, did not have a registered diagnosis, or had a type of surgery related to reoperation (wound debridement, vacuum-assisted treatment of wounds, extraction of implants, and operation on patient with infection). For patients with a verified reoperation, the following additional data were collected: date of reoperation, cause of reoperation, total number of reoperations (until 1 April 2020, when the manual review started), and cultures (when available).
Statistical Methods
Statistical analysis was performed using IBM SPSS Statistics for Windows, version 28. Only descriptive analysis has been used in this study because the sample had to be divided into subgroups related to types of surgery. We analyzed measurements of frequency on the number of patients with reoperations and causes of reoperations. Demographic data were analyzed using measurements of central tendency and dispersion. In the analysis, the type of surgery was crudely organized into 7 groups consisting of the 5 most common types of surgery and 1 group consisting of all surgeries with implants and 1 group with all spinal surgeries. No analysis was performed with regard to the level of the spine that was involved in the surgery. The reason for this is that these data were missing for most of the operations in the database of the surgical planning program.
For patients who had multiple index surgeries (different levels of the spine) during the study period, only data from the first operation were analyzed. When presenting the cause of reoperation, we chose to show the 7 most common causes in this population (infection, implant-related, hemorrhage/hematoma, patient not experiencing improvement, residual stenosis or restenosis, herniated disc recurrence, and spinal fluid leakage). Implant-related complications consist of implant migration, implant breakage, misplaced implant, and pain over the implant site (eg, implant pressing against the skin). Infection as a cause of reoperation was defined as a patient in whom the decision to perform revision surgery was taken based on a suspected or confirmed (clinical signs or blood samples/cultures) infection. A patient not experiencing any improvement was defined as a patient in whom the decision to perform revision surgery was based on the patient’s subjective experience of pain or other symptoms.
Furthermore, the present study analyzed only the primary cause of reoperation (stated in patients’ medical records as the main reason for performing additional surgery). It is important to remember that in several cases, there were multiple complications; for example, a patient with infection might also turn out to have implant migration and vice versa.
To ascertain the correctness of our database, we selected a random sample of 100 operations from the original database (before excluding patients) and compared the diagnosis and type of surgery in the surgical planning program with the patient’s electronic medical records.
RESULTS
Among the 2110 patients in the studied population, 11% (n = 232) were patients with a manually confirmed reoperation during the study period. Demographics and clinical data grouped by type of surgery are summarized in Table 1. Operations involving implants have a longer operating time and a higher reoperation rate. Deformity surgery (idiopathic or degenerative scoliosis) stands out as the type of surgery that has the highest frequency of reoperations (19%).
Demographics for patients undergoing primary spinal surgery between 1 January 2015 and 20 May 2018, grouped by the type of surgery.
The reoperation frequency was higher for the group of patients with the longest follow-up. More than half (51%) of all patients who required revision surgery had their reoperation within 30 days. The reoperation frequency, depending on follow-up time, is presented in Table 2.
Reoperation frequency depending on follow-up time for patients undergoing spinal surgery between 1 January 2015 and 20 May 2018.
The most common cause of reoperation was infection (n = 65, 28%), followed by implant-related complications (n = 44, 19%), and postoperative hematoma (n = 34, 15%). Infection was the most common cause regardless of the length of follow-up. Among patients who had a reoperation because of infection, 26% (n = 17) required 3 or more reoperations. Most of the infected patients (89%, n = 58) had index surgery involving implants. In the subgroup of patients who had deformity surgery as the index surgery, the number of patients who had a reoperation because of infection were 71.4% (n = 20). The causes of reoperations are presented in Table 3.
Causes of reoperations in all groups, with primary causes.
The time between index surgery and reoperation varied, depending on the cause of the reoperation. In patients reoperated for infection (n = 65), 71% (n = 46) had their reoperation within 30 days. In patients with implant-related causes of reoperation (n = 44), 59% (n = 26) waited more than 100 days between index surgery and reoperation. For the small number of patients who had a reoperation because they did not experience any improvement (n = 14), all but 1 waited more than 6 months between index surgery and reoperation.
Positive bacterial cultures from patients reoperated for infection showed that different types of skin bacteria were the most common agents. Coagulase-negative staphylococci were the most common type of bacteria (39%, n = 25), while Propronibacterium acnes was the most commonly isolated single bacterium (32%, n = 21), followed by Staphylococcus aureus (19%, n = 12). There were also 7 negative cultures (11%) among patients undergoing a reoperation because of infection. More than 1 infectious agent was present in 11 (17%) cultures.
Based on the comparison of data sources in a random selection of 100 operations, the agreement between the data from the surgical planning program and the patient medical records was found to be low. The information regarding the type of surgery and diagnosis was only the same in both systems in 62% of the reviewed cases, while the remaining cases all differed in some way. In 14% of the reviewed cases, the reported type of surgery or diagnosis differed completely between the 2 systems.
DISCUSSION
Our study found that 11% of all spinal surgery patients required a reoperation during the study period. The most common causes of reoperation were infection (28%), followed by implant complications (19%), and postoperative hematoma (15%). The time between the index surgery and reoperation varied, depending on the cause of reoperation, but half of all reoperations occurred within 30 days. In patients undergoing reoperation because of infection, coagulase-negative staphylococci were the most common type of bacteria (positive cultures in 39% of the patients).
The overall reoperation frequency is within the range of previously published studies, with frequencies ranging between 5.4% and 27% for various types of surgeries and length of follow-up.3–6,12 Even so, the incidence in the present study is still high and the cost in personal suffering and the draining of hospital resources are substantial.
For surgical procedures without instrumentation, our results compare well with results from existing literature. For decompression/laminectomy, we found a reoperation rate of 9.7%, while other studies have reported rates between 4% and 14.9%.13–15 The reoperation rate for open discectomy in our cohort was 6.6%, corresponding to 5.6% to 9.8% in previous studies.16,17
The most common cause of reoperation in our study population was infection, representing 28% of all reoperations. In several previous studies of different types of spinal surgeries,3,4,6 the most common reason for reoperation was instead implant-related causes (29%–59%). In these studies, the population consisted of patients with surgery involving implants. If we limit our study population to the subgroup undergoing implant surgery, the result is similar (33% of reoperations caused by complications with implants). However, infection is still the most common cause of reoperation in this subgroup (responsible for 44% of the reoperations). The number of patients in our population requiring revision surgery because of infection (n = 65, 3.1%) correspond to findings in other studies (2.1%–3.1%).18–20 However, most of the infected patients in our cohort had undergone operations involving implants. If we look at this subgroup alone, the reoperation rate because of infection was 6% (n = 58). Since the causes of infection are multifactorial and many risk factors are modifiable21 and, given the large scale, often persistent suffering that infections following implant surgery has on patients,22–25 the need to systematically reduce the risk of infection is substantial. Moreover, the economic impact on hospital and social resources is almost 4 times higher than that for uninfected patients.24 Preventing surgical site infections (SSI) should therefore be a priority for caregivers.
There are already numerous different strategies to try to prevent and lower the incidence of SSI following spinal surgery. However, the level of evidence supporting these strategies is too low to establish a best practice SSI prevention guideline for spinal surgery.26 For this reason, well-designed bundle interventions could be a way forward.
In our population, 3.4% of patients who had decompression surgery also had a reoperation because of residual/restenosis, representing 35% of the reoperations for this type of surgery. This is somewhat lower than the figure in a comparable study exploring outcome after decompressive surgery for spinal stenosis, where 5.8% of the patients underwent additional surgery because of recurrent stenosis.15
Postoperative hematoma resulting in a reoperation had an incidence of 1.6% in our study. A previous study found an incidence of 1.1% after spinal surgery.27 It was a relatively common cause of reoperation in our population, accounting for 26.3% of the reoperations that occurred within 30 days. A multicenter study of reoperations within 30 days found similar results, with a postoperative epidural hematoma responsible for 24% of reoperations.28
The recurrence of lumbar disc herniation as a cause of reoperation following open discectomy was 4.2%, corresponding well to 4.1% to 5.3% found in other studies.5,10
In this study, the incidence of reoperations because of a dura tear was 0.5% (n = 11), comparing well with a previously published study, 0.7%.29
The remaining causes of reoperation (patient not experiencing any improvement and other causes) cannot be further analyzed, since each case represents individual reasons for the decision to perform revision surgery.
The time between index surgery and reoperation varied greatly, depending on the cause of reoperation, in our material. It is interesting that 71% of the patients undergoing a reoperation because of infection had their second surgery within 30 days, but we have been unable to identify other studies with which to compare our result for this variable. In a study with a long-term (5–15 years) follow-up after disc replacement,3 the mean time between the first and second surgery was 35 months. If our study had a similar follow-up period, the relationship between different causes of reoperation might well have shifted.
Our finding of different types of skin bacteria as the most commonly isolated agents in cultures from infected patients corresponds to previous research on the subject.30
The number of spinal surgeries have increased significantly both nationally1,2 and internationally31,32 over a long period. It is therefore increasingly important to continuously evaluate the long-term outcomes of spinal surgery in order to improve clinical practice. To evaluate the long-term outcomes, we need reliable data. Our study found that the data in the studied hospital’s internal records differed, and a manual review was required to acquire reliable data. Because of a considerable amount of under-reporting of complications,7 the use of data from Swespine might also be questionable. To be able to evaluate the long-term outcome with the emphasis on complications, we believe that prospectively collected data represent the best way to obtain reliable data.
Strengths and Limitations
Since we had access to all the internal systems at the studied hospital, we had the opportunity to verify outliers and find data missing from the surgical planning program in another system. All reoperations were confirmed manually by comparing all the available data on the patient.
The case mix at the studied hospital includes a large proportion of patients with complicated procedures and comorbidities that would not be performed at many other private or public clinics. Although it is a strength that our data not only consist of low-risk patients, it also makes it more difficult to compare our findings with reoperation rates in other settings.
There are also several other limitations. Since the agreement between hospital medical record systems was found to be poor, the reliability of baseline data for the entire population is also low. We were only able to manually review all hospital records of suspected reoperations. We would have obtained more reliable results if we had been able to compare all hospital records for the entire study population. The use of a hospital’s medical records means that some of the patients might have had surgery at another clinic prior to or during our study period.
Despite its limitations, we still believe our study provides a valuable insight into the reoperation frequency and causes of reoperation after spinal surgery at the studied hospital.
CONCLUSIONS
The number of reoperations after spinal surgery at the studied hospital were high during the study period. Infections constituted a main cause of reoperations, suggesting that effective preventive measures might significantly reduce the total number of reoperations.
Footnotes
Funding This work was supported by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (ID no: 238801) and the Local Research and Development Council Gothenburg and Södra Bohuslän under Grant Agreement (ID no: 941560).
Declaration of Conflicting Interests All the authors are employed by the studied hospital.
Ethics Approval Ethical permission was given by the Swedish Ethical Review Authority (ID number: 2020-05402).
Data Availability Statement The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.