


Abstract
Background Multilevel anterior cervical discectomy and fusion inevitably yields a higher chance of pseudarthrosis or require more reoperations than single-level procedures. Therefore, multilevel cervical disc arthroplasty (CDA) could be an alternative surgery for cervical spondylosis, as it (particularly 3- and 4-level CDA) could preserve more functional motility than single-level disc diseases. This study aimed to investigate the clinical and radiological outcomes of 4-level CDA, a relatively infrequently indicated surgery.
Methods The medical records of consecutive patients who underwent 4-level CDA were retrospectively reviewed. These highly selected patients typically had multilevel disc herniations with mild spondylosis. The inclusion criteria were symptomatic cervical spondylotic myelopathy, radiculopathy, or both, that were medically refractory. The clinical outcomes were assessed. The radiographic outcomes, including global and individual segmental range of motion (ROM) at C3-7, and any complications were also analyzed.
Results Data from a total of 20 patients (mean age: 56 ± 8 years) with an average follow-up of 34 ± 20 months were analyzed. All patients reported improved clinical outcomes compared with that of preoperation, and the ROMs at C3-7 were not only preserved but also trended toward an increase (35 ± 8 vs 37 ± 10 degrees, pre- vs postoperation, P = 0.271) after the 4-level CDA. However, global cervical alignment remained unchanged. There was one permanent C5 radiculopathy, but no other neurological deteriorations or any reoperations occurred.
Conclusion For these rare but unique indications, 4-level CDA yielded clinical improvement and preserved segmental motility with low rates of complications. Four-level CDA is a safe and effective surgery, maintaining the ROM in patients with primarily disc herniations and mild spondylosis.
Clinical Relevance For patients with mild spondylosis, whose degeneration at the cervical spine is not so severe, CDA is more suitable.
Level of Evidence 4.
- anterior cervical discectomy and fusion (ACDF)
- cervical disc arthroplasty (CDA)
- range of motion (ROM)
- multi-level
- four-level
Introduction
During the past 2 decades, cervical disc arthroplasty (CDA) has become accepted as a viable alternative to anterior cervical discectomy and fusion (ACDF) as a surgical management strategy for 1- or 2-level cervical disc herniation or spondylosis that causes radiculopathy, myelopathy, or both. Many United States Food and Drug Administration investigational device exemption randomized controlled trials have demonstrated the safety and efficacy of CDA in comparison to ACDF in 1- and 2-level diseases.1–3 Furthermore, 10-year follow-up data for CDA also demonstrated long-term clinical and radiological outcomes favoring CDA over ACDF4 for the preservation of segmental mobility and possibly less chance of adjacent segment degeneration.5
The superiority of motion preservation in CDA over ACDF is likely amplified as the levels of diseased discs increase. In the trials comparing 1-level CDA to ACDF, there was an average loss of 7 to 9 degrees of flexion-extension range of motion (ROM) after arthrodesis.6 For patients with only 1-level disc herniation, this mitigation of flexion-extension ROM of less than 10 degrees after ACDF affects minimal global neck motion and is thus often unnoticeable in daily activity. Therefore, the advantageous preservation of motion with CDA over ACDF might not be eminent in 1-level disease. However, the loss of nearly 10 degrees for each level could become significant in patients who undergo 3- or 4-level ACDF that inevitably causes 30 or 40 degrees of elimination in flexion-extension ROM.7 Reports on comparisons of CDA to ACDF for 2- and 3-level treatment demonstrated equivalent neurological improvement and similar complication rates between the 2 cohorts, but the multiple levels of ACDF, which aimed to fuse the spine, simultaneously caused a reduction in flexion-extension ROM by more than 17 to up to 22 degrees.8,9 In contrast, the neck ROM of patients with 2 or more levels of CDA was well maintained in many series of patients.8,9 Therefore, the maintenance of spinal segmental ROM by CDA in 4-level cervical spondylosis is intuitively advantageous to ACDF, though it requires data for corroboration. Therefore, this study aimed to demonstrate the efficacy and durability of 4-level CDA.
However, very few patients with multilevel disc herniations are eligible for CDA. The best candidates for multilevel CDA are patients with primarily disc herniations and only mild spondylotic osteophytes, such that their facet joints remain competent, and there is minimal instability. In common practice, multilevel disc problems are frequently associated with ankylosing osteophytes, kyphosis, and severe facet arthropathy, which warrant ACDF for better correction of deformity and restoration of stability. Therefore, 3 or 4 levels of CDA are very rarely indicated and should be reserved for young patients with adequate bone quality. Most of the commonly seen patients who have 3- or 4-level cervical spondylosis come with a coexisting deformity and profound osteophytes that require ACDF or other posterior surgical approaches. Although many reports have demonstrated the effectiveness of multilevel ACDF, the rates of pseudarthrosis unavoidably increase as the fusion constructs get longer.10 Moreover, the limitation of neck mobility and neck stiffness is substantial and could significantly compromise the quality of life. Therefore, it is reasonable to infer that multilevel CDA is a superior surgical option for several reasons—including achieving direct decompression anteriorly, avoidance of posterior muscular tension-band injury, and the preservation of neck mobility—compared with other cervical fusion surgery. As there is a clear trend of spinal surgery pushing beyond the envelope of CDA,11 the effectiveness, clinical results, and safety of 4-level CDA should be examined.
In this retrospective study, highly selected patients, who were appropriate candidates for 4-level CDA, were investigated for their results spanning more than 2 years. The clinical outcomes, radiographic measurements, segmental mobility, and complications were all reported to address the risks and benefits of multilevel CDA with the upmost discs replaced. To our knowledge, this is, to date, the largest cohort reported on the surgery of 4-level CDA.
Methods
Patient Enrollment
The present retrospective study was conducted using a prospectively collected patient database. All patients’ medical records and images were retrospectively reviewed. Preoperative medical images, such magnetic resonance images, computed tomography images, and radiographs, were routinely obtained for the diagnosis of cord compression and evaluation of segmental stability, ROM, bone spurs, calcified discs, or ossification of the posterior longitudinal ligament (OPLL).
A series of consecutive patients older than 18 years who underwent 4-level CDA with Prodisc-C Vivo (Centinel Spine, West Chester, PA) or Mobi-C (Zimmer-Biomet, Warsaw, IN) artificial discs at C3-7 of the cervical spine were included. The surgical indications for CDA were symptomatic disc herniation and/or spondylosis with radiculopathy, myelopathy, or both (Figure 1). Any hybrid construct consisting of the combination of CDA and ACDF was not enrolled in this study. All patients failed at least 12 weeks of conservative management, including medication, physical therapy, and pain control. Exclusion criteria were identical to previous FDA-IDE trials,3,12–14 which were: (1) spinal trauma and fracture; (2) evident segmental instability (ie, more than 2 mm translation or 20° angular motion); (3) ankylosis or arthrodesis without mobility; (4) severely incompetent facet joints; (5) adjacent segment disease; (6) OPLL; (7) kyphotic deformity; (8) infection; and (9) long-term steroid use. Systemic diseases such as severe osteoporosis, malignancy, metabolic bone disease, and cerebrovascular disease were excluded. Autoimmune disease or spondyloarthropathy, such as rheumatoid arthritis or ankylosing spondylitis, were also contraindicated for CDA.

The preoperative magnetic resonance image of a 53-year-old woman who underwent 4-level CDA. Each level from C3-4 to C6-7 showed significant disc herniation and spinal stenosis that required surgery.
Surgical Technique
The classic Cloward technique for an anterior cervical approach was performed in all patients.15 Following complete discectomy, bilateral uncovertebral joints, bone spurs, and posterior longitudinal ligaments were generously removed with high-speed burrs and Kerrison’s rongeurs to achieve decompression of the dura sac and exiting nerve roots. Decent carpentry (careful endplate preparation, selection of the most appropriate size of artificial disc, and centering of the CDA device) was undertaken during implantation to ensure the best function of the artificial discs at C3-7.16 Copious saline irrigation was used persistently to wash away the bone dust during osteophyte drilling in every case. All surgeries were executed by senior neurosurgeons with consistent techniques, as described in our previous reports.8,17,18
Clinical and Radiographic Outcomes
In our prospective database, a postoperative outpatient clinic was arranged on a regular basis for clinical parameters and radiographic image follow-up. The postoperative follow-up time points were set at 6 weeks and at 3, 6, 12, and 24 months for all patients. After 24 months, annual follow-ups were arranged at the patient’s discretion. We routinely collected pre- and postoperative clinical patient-reported outcomes (PROs) such as the visual analog scale (VAS) for arm and neck pain, Neck Disability Index, and modified Japanese Orthopedic Association scores. Radiographic images in clinics were also collected, including antero-posterior, lateral, and flexion-extension x-ray films taken at every regular visit. Both subaxial C3-7 ROM and individual segmental ROM at each operative level (C3-4, C4-5, C5-6, and C6-7, respectively) were measured with standing lateral flexion and extension radiographs at preoperation and final follow-up using the Cobb method.3,17 Pre- and postoperative C2-7 global alignments, including C2-7 Cobb angle and sagittal vertical axis, were also measured with standard antero-posterior and lateral radiographs.17 All the measurements of ROMs and global alignments, both pre- and postoperatively, were determined by a radiologist independently with the PACS system software, SmartIris (Taiwan Electronic Data Processing Co., Taiwan).
Statistical Analysis
Paired and independent t tests were used for the analysis of continuous variables. Analyses of categorical variables were performed via Pearson’s χ 2 test. All statistical analyses were performed using the SPSS software (SPSS Inc., Chicago, IL). The statistical significance was set at P < 0.05.
Results
Demographics, Clinical PROs, and Complications
A total of 20 patients who underwent 4-level CDA surgery with Prodisc-C Vivo or Mobi-C artificial discs were retrospectively reviewed. All patients received the same kind of devices (either Prodisc-C Vivo or Mobi-C) without mixed brands of artificial discs or other implants. Sizing of each artificial disc was determined intraoperatively using the device-specific implant trials, according to reference measurements made by preoperative computed tomography, with each one tailor-made for each indexed level. None of the patients had any ACDF or anterior cervical corpectomy or fusion hybrid construct in the series. These patients were typically younger and not affected by osteoporosis. The average age at operation was 56 ± 8 years, and there was a male predominance (men:women = 17:3). The mean follow-up was 34 ± 20 months. All the demographic data are provided in Table 1.
Patients’ demographic data, radiographic outcomes, and complication profile.
All clinical outcomes demonstrated significant improvement after surgery. At the final follow-up, the PROs were improved, including visual analog scale of neck and arm pain, which improved from 4.6 ± 4.0 and 4.3 ± 3.6 to 1.3 ± 1.8 and 1.0 ± 1.7 (P = 0.021 and 0.026), respectively; the Neck Disability Index from 8.2 ± 7.4 to 3.9 ± 3.0 (P = 0.034), and the Japanese Orthopedic Association scores from 13.8 ± 1.7 to 15.2 ± 1.3 (P = 0.041; Table 2).
Clinical outcome measures.
Complication profiles are detailed in Table 1. There were a few common and self-limiting complications of anterior cervical spine surgery, including transient dysphagia and C5 radiculopathy. In the series, there were 2 cases of transient dysphagia, and both were resolved within 3 months. There was no permanent dysphagia or hoarseness. A total of 3 patients developed unilateral C5 radiculopathy after surgery. One of the C5 radiculopathy cases did not resolve at the final follow-up, while the other 2 were transient and recovered after rehabilitation within 6 months. There was no intraoperative cerebrospinal fluid leakage or other wound complications. To date, there was no secondary surgery, no implant failure, and no need of removal or revision (CDA conversion to ACDF) in the series during the entire follow-up period.
Radiographic Outcomes
The global neck motion after 4-level CDA in every patient was well preserved at the final follow-up. The pre- and postoperative subaxial C3-7 ROMs and individual segmental ROMs at each operated level are demonstrated in Table 1. In the series of 20 patients, the 4-level CDA successfully preserved subaxial ROM at a mean of 37 ± 10 degrees postoperation compared with that of 35 ± 8 degrees preoperation at C3-7. Although the mean subaxial C3-7 ROM increased by 2 degrees postoperation, there was no statistical difference (P = 0.271; Figure 2). Moreover, the mean ROM of each level (ie, C3-4, 4–5, 5–6, and 6–7) after 4-level CDA was averaged at 9 ± 0.9, 9 ± 0.9, 9 ± 1.0, and 9 ± 1.0 degrees, respectively. Each CDA level contributed almost equally to mobility from C3-4 to C6-7 in this series of patients. Pre- and postoperative C2-7 global alignment did not significantly differ after 4-level CDA. The C2-7 Cobb angle slightly increased from 8 ± 11 to 12 ± 12 without a statistical difference (P = 0.114). C2-7 sagittal vertical axis remained mostly unchanged (preoperative: 2.2 ± 1.3 cm vs postoperative: 2.3 ± 1.5 cm, P = 0.804).

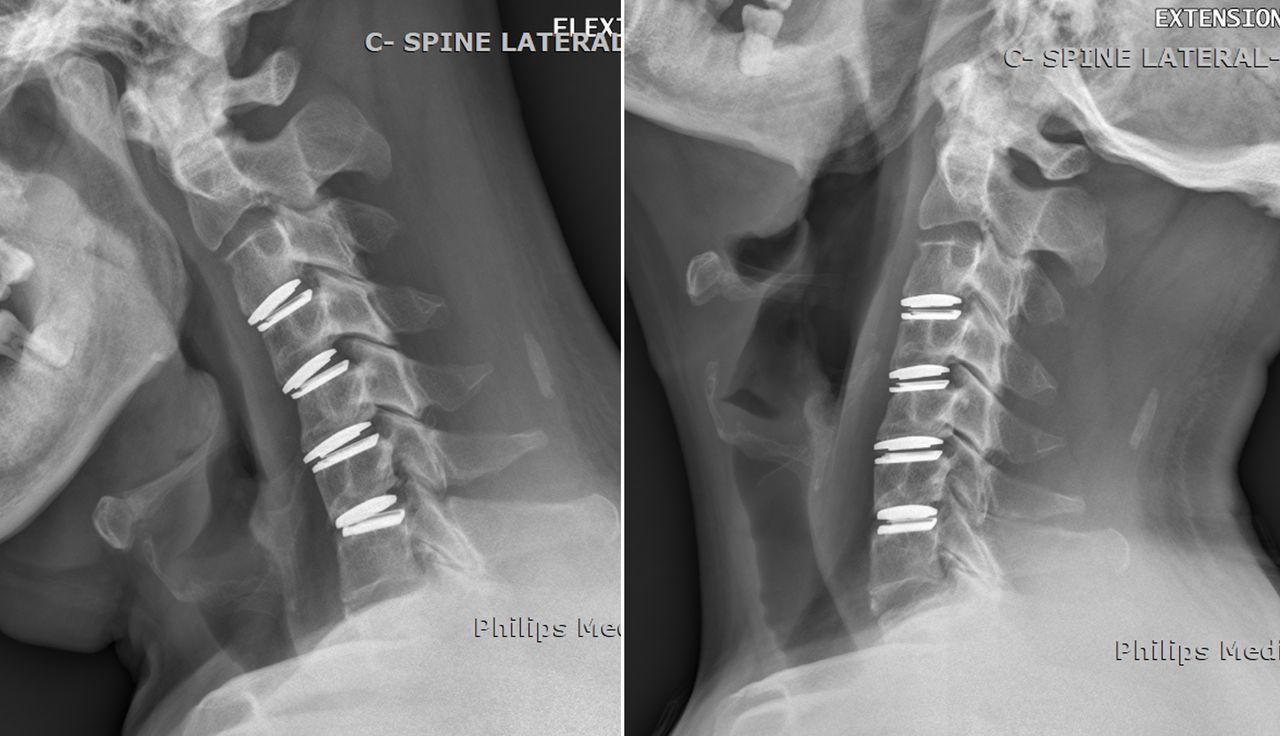
Postoperative flexion/extension radiographs from the patient in Figure 1 at 24 months after surgery. The range of motion at each level was well preserved. Each artificial disc was demonstrated to be well-functioning.
Discussion
The present study, which to our knowledge is the first in the literature with more than 2 years of PROs, included a series of 20 patients who underwent 4-level CDA with a mean follow-up of more than 30 months. The report demonstrated neurological success and improved clinical outcomes, with well-preserved segmental spinal motility in every patient. The retrospective study also had the merit of very strict and homogeneous inclusion criteria for CDA, which excluded patients with slight kyphosis, ankylosis, or facet arthropathy. Although these patients arguably could also be candidates for ACDF in conventional concepts, in the current study, the results have demonstrated a potential advantage of using CDA to maintain the spinal motion at all 4 disc levels (ie, C3-7). With high rates of clinical success, 4-level CDA unanimously preserved flexion-extension ROM at approximately 37 degrees on average at C3-7. Typically, these patients were relatively young, usually aged in their 40s to 50s, and had substantial neurological symptoms, including myelopathy concomitant with radiculopathy, that were caused by multiple disc herniations. Despite the lack of a cohort of 4-level ACDF patients for comparison, this study demonstrates the maintenance of a large amount of motion relative to the minimal motion that would be expected in a successful ACDF. With a similarly low rate of complications as ACDF, CDA relieves neurological symptoms successfully with the preservation of spinal ROM. Moreover, there were no device-related complications or the need for a revision or secondary surgery during the follow-up. In contrast, multiple levels of ACDF inevitably yield a higher chance of pseudarthrosis or the need for reoperations, albeit not very frequently. Therefore, multilevel CDA could have a role as an alternative surgery for cervical spondylosis, especially for patients whose pathology is primarily limited to the disc.
Three-, 4-, and even 5-level ACDFs are established surgical procedures that have been published in the literature worldwide.19–21 It is evident that there would be a tremendous loss of neck ROM after multilevel ACDF, as it aims to fuse. A major reduction of neck ROM in sagittal plane flexion (39.5%) and extension (18.3%), lateral flexion (25.7%–25.9%), and rotation (14.0%–14.4%) has been reported with 4-level ACDF.7 In contrast, previous reports on 2- and 3-level CDA demonstrated successful preservation of 17 and 25 degrees of neck ROM on average, respectively.8,22 In the present study, 4-level CDA successfully preserved approximately 37 degrees of neck ROM on flexion-extension dynamic radiographs at the final follow-up. Although single-level ACDF may not significantly disturb the neck mobility of patients, multilevel arthrodesis apparently limits neck motility and lowers the quality of life.23 This addition of ROM preservation of the neck at multilevels of surgery may be the most underrated benefit of CDA.
Two-level CDA is a commonly accepted alternative to 2-level ACDF with the potential advantages of fewer reoperations and reduced chances of adjacent segment degeneration, and these have been demonstrated by several prospective randomized controlled trials with 7 to 10 years of follow-up.4,5,24–27 On the other hand, for multisegmental cervical spondylosis and stenosis, 4-level ACDF has been known for its increasing risk of nonunion, as more bone-graft interfaces are inevitably involved. With the currently available biologics, the incidences of pseudarthrosis for 4-level ACDF could be reportedly as high as 60%.28–31 Moreover, the 4-level ACDF unavoidably limits neck motion and increases pressure loads on adjacent segments, which could adversely affect quality of life. Therefore, with the option of CDA, 4-level ACDF should be reserved for patients with kyphotic deformity, incompetent posterior elements, or ankylosing osteophytes that require instrumented fusion for correction of alignment issues. For patients with mostly disc herniations and little facet arthropathy, 4-level CDA is the preferred surgical option based on the higher chances of preservation of physiological mobility and less risk of pseudarthrosis and subsequent reoperations. Thus, in the authors’ opinion, few patients would consent to 4-level fusion as the control cohort, since the current literature is well elaborated. Although we also agree that some surgeons would choose posterior techniques such as laminoplasty for 4-level disc problems, it is intuitive to address the problem directly via anterior approaches since posterior indirect decompression requires more muscle dissections. Nevertheless, a comparison of CDA to posterior cervical laminoplasty would be inappropriate and beyond the current study concept. For the aforementioned reasons, the current study did not include a control group of 4-level ACDF, posterior fusion, or laminoplasty.
There are limitations to the current study. This is a retrospective review of a small series of patients who underwent 4-level CDA, and there was no ACDF for comparison. However, due to the rarity of pure disc herniations in all 4 levels of cervical spine requiring surgery, this report presents the best currently available data to date. Patients with 4-level disc problems that were complicated with any kyphosis, facet arthrodesis, or small segmental OPLL would be advised to undergo ACDF. Considering the long history of ACDF since 1958, 4- or 5-level ACDF surgery could be referenced in the literature for fusion rates and complication profiles. The current study focused on a series of 4-level CDA patients with strict selection criteria in a high-volume cervical spine surgery center. All the surgical and complication profiles, as well as clinical and radiological outcomes, were reported. The study of this 4-level CDA surgery also had less concern about the development of adjacent segment disease because all discs of the subaxial cervical spine were treated. The effect of long-term motion preservation and the development of heterotopic ossification require additional investigations.
Conclusion
Using the strict selection criteria for surgery, 4-level CDA yielded clinical improvement and preservation of spinal motility with low rates of complications. Four-level CDA is a safe and effective surgical option and has the potential advantage over ACDF by maintaining the ROM in patients with cervical disc herniations, mild spondylosis, and competent posterior elements.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval The present retrospective study was approved by the IRB of our institute. Informed consents were waived by the IRB.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.