


Abstract
Background Oblique lumbar interbody fusion (OLIF) through a prepsoas approach was identified as an alternative to alleviate complications associated with direct lateral interbody fusion. Cage placement is known to influence cage subsidence and fusion rates due to suboptimal biomechanics. There are limited studies exploring cage obliquity as a potential factor influencing fusion outcomes. Hence, our objective was to assess the effects of cage obliquity and position on fusion rates, subsidence, and sagittal alignment in patients who underwent OLIF.
Methods Patients who underwent OLIF for levels L1 to L5 in our center, performed by a single surgeon and with a minimum of 12 months of follow-up, were included in the study. Cage obliquity and sagittal placement were measured, and their correlation with fusion, subsidence, and sagittal alignment correction was assessed. Fusion and subsidence were evaluated using the Bridwell Criteria and Marchi Criteria, respectively.
Results Among the included patients (age, 67.5 ± 7.93 years; 16 men and 37 women), 97 fusion levels were studied. The mean cage obliquity was 4.2° ± 2.8°. Ninety-six levels (99.0%) were considered to have achieved fusion with a Bridwell score of 1 or 2. Eighty-one (83.5%), 14 (14.4%), and 2 (2.06%) operated levels had a Marchi score of 0, 1, and 2, respectively. A Marchi grade of 1 or higher was considered indicative of significant subsidence. There was good improvement in both the segmental lordosis angle (4.2° ± 5.7°; P < 0.0001) and disc height (4.5 ± 3.8 mm; P < 0.0001). Cage placement did not have any statistical correlation with fusion rates, subsidence, or sagittal alignment.
Conclusions Our results indicate that OLIF facilitates appropriate cage placement with only a minor degree of cage obliquity, typically less than 20°. This minor obliquity does not lead to lower fusion rates, increased subsidence, or sagittal malalignment. Despite subsidence being common, the majority of these cases resulted in complete fusion.
Level of Evidence 3.
Introduction
Since its development by Luis Pimenta 2 decades ago, the minimally invasive extreme lateral interbody fusion, also known as direct lateral interbody fusion, has emerged as a valuable technique for approaching the lumbar spine via a transpsoas approach. This technique has demonstrated numerous advantages, including high fusion rates, effective deformity correction, and indirect decompression.1 Later, Hynes modified this approach to access the spine through a prepsoas or anterior-to-psoas oblique corridor to circumvent concerns about the transpsoas approach such as thigh pain, lumbar plexus injury, and obstruction of the approach by a high iliac crest.2 This was labeled the oblique lumbar interbody fusion (OLIF). The technique offers a lower risk of psoas and lumbar plexus injuries compared with direct lateral interbody fusion, as well as a lower risk of injury to the bowel and great vessels compared with an anterior approach.3
However, the OLIF approach has raised some questions, especially with regard to cage placement, particularly if the cage is placed obliquely. Cage placement is known to affect lordosis and foraminal decompression and influences the incidence of cage subsidence and fusion rates due to suboptimal biomechanics, potentially leading to persistent symptoms, implant failure, and the necessity for revision surgery.4–6 Nonetheless, the relationship between cage orientation and its effects on the radiological outcomes of OLIF remains inadequately explored in the literature. Hence, we aim to investigate the relationship between cage placement, position, and orientation with objective measures of fusion rates, subsidence rates, and the degree of sagittal alignment correction.
Materials and Methods
This is a retrospective study of patients who underwent an OLIF procedure in our tertiary center under a single surgeon. These patients had a minimum of 12 months of postoperative follow-up. We included all patients who underwent OLIF for the spinal levels between L1 and L5 for lumbar degenerative disease, lumbar spinal stenosis, and lumbar spondylolisthesis. All patients underwent postoperative computed tomography (CT) of their lumbar spine to assess fusion. We excluded patients who were treated for traumatic, infective, and malignant spine diseases, as well as patients who underwent revision surgery.
Operative Technique
The surgical technique has been described in detail according to Wong et al.7 The procedure is performed with the patient under general anesthesia. The patient is positioned in a right lateral decubitus position on a radiolucent table. Once positioned, the legs are slightly flexed. Prior to the commencement of surgery, the position and level of surgery are checked on C-arm fluoroscopy. An incision of roughly 5 cm is made approximately 3 to 5 cm anterior to the middle of the disc. The fascia of the external oblique is incised with electrocautery. Gentle finger dissection of the external oblique, internal oblique, and transversalis muscles is performed. Once the retroperitoneal fat plane is reached, the space is developed both cephalad and caudal to the desired disc level. A guide wire is inserted, followed by a series of dilators to create space pushing aside the surrounding tissues. Subsequently, a retractor is positioned over the dilators. This can be anchored to the vertebral body using a pin. The retractor blades are oriented to allow for an orthogonal maneuver to access the disc space. This is utilized during disc removal, sequential trialing, and final placement of the interbody cage. Annulotomy and discectomy are performed, and the disc space is prepared. After completing the disc preparation, a contralateral annular release is performed using a blunt-tipped shaver or Cobb elevator. Sequential trials distract the disc space and allow indirect decompression. Finally, a wide-bodied interbody cage is prepared with demineralized bone matrix and bone morphogenic protein. It is then placed within the disc space. The procedure can be accompanied by posterior stabilization. This can be performed using either the open or minimally invasive surgery technique. Pedicle screw insertion is performed under navigation or with robotic assistance.
Radiological Parameters
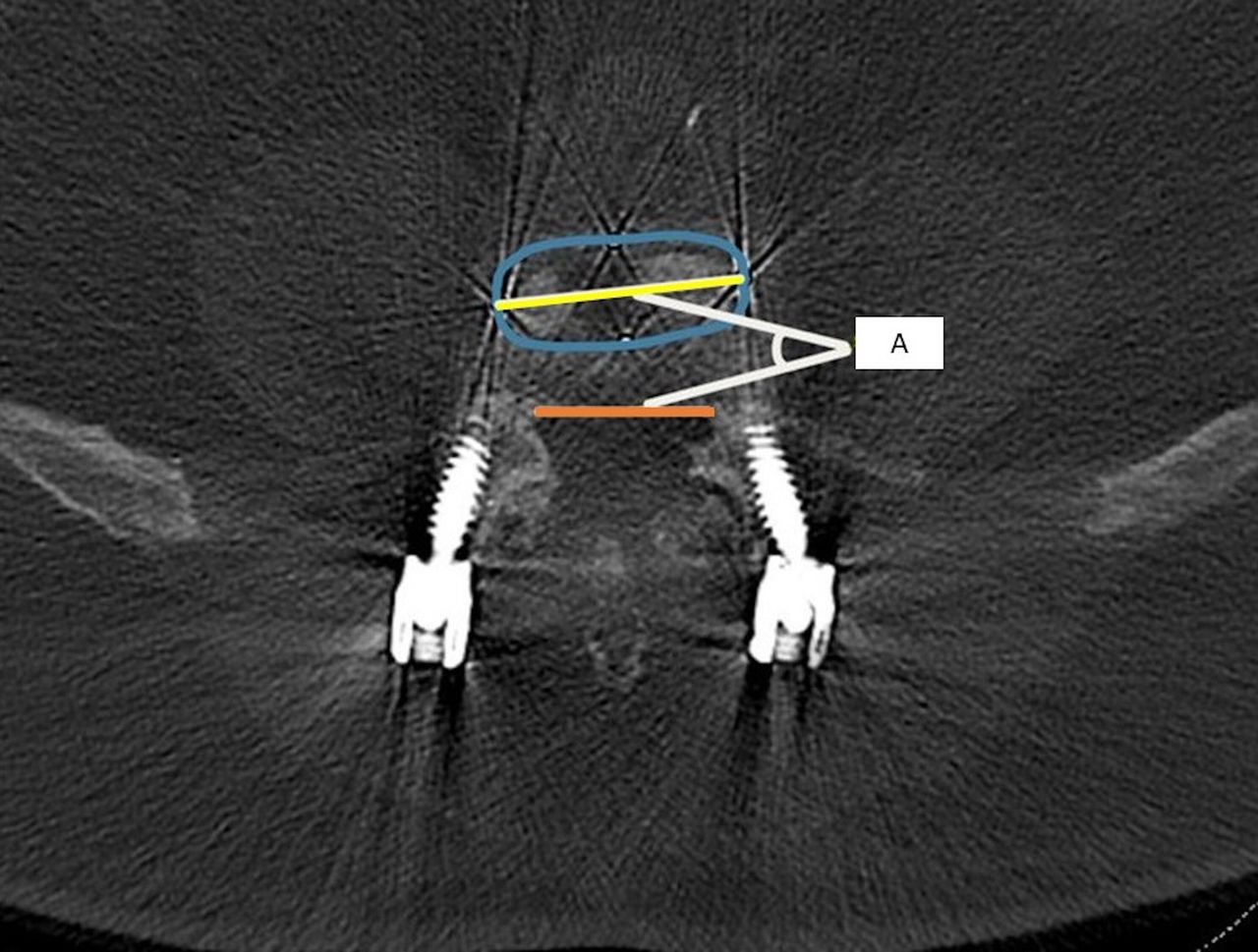
Postoperative radiological outcomes were assessed with standing lumbar spine radiographs and lumbar spine CT images. Radiological data were collected by 3 independent observers who not involved in the surgery, with each observer assessing different sets of images. Cage placement in the sagittal plane was assessed using erect lateral lumbar spine radiographs. Cage obliquity was assessed using axial cuts on the CT image. This was measured as the angle between a horizontal line down the length of the cage and a line along the posterior border of the vertebral body (Figure 1).5,8 We defined significant obliquity as a reading of more than 20°.

Obliquity of the cage was measured as an angle (A) between a horizontal line (yellow) down the length of the cage and a line along the posterior border of the vertebral body (orange) using the computerized software. The blue line represents the outline of the interbody cage.
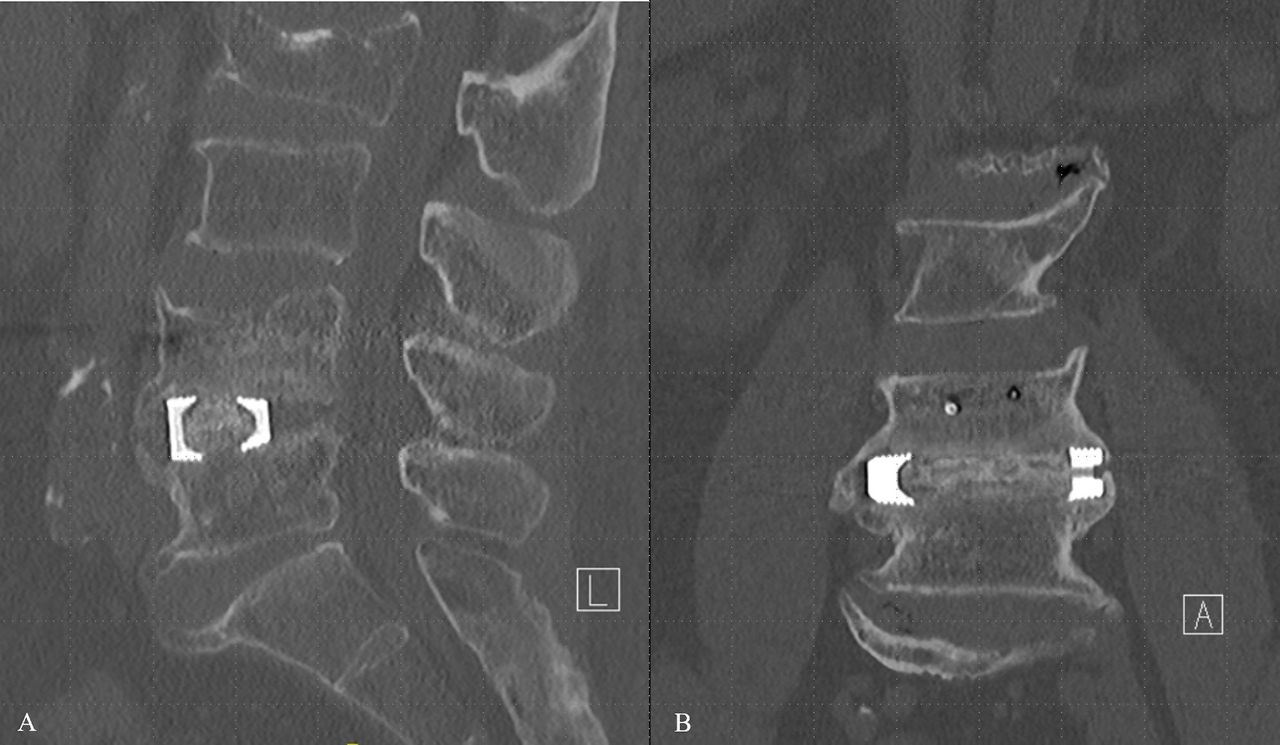
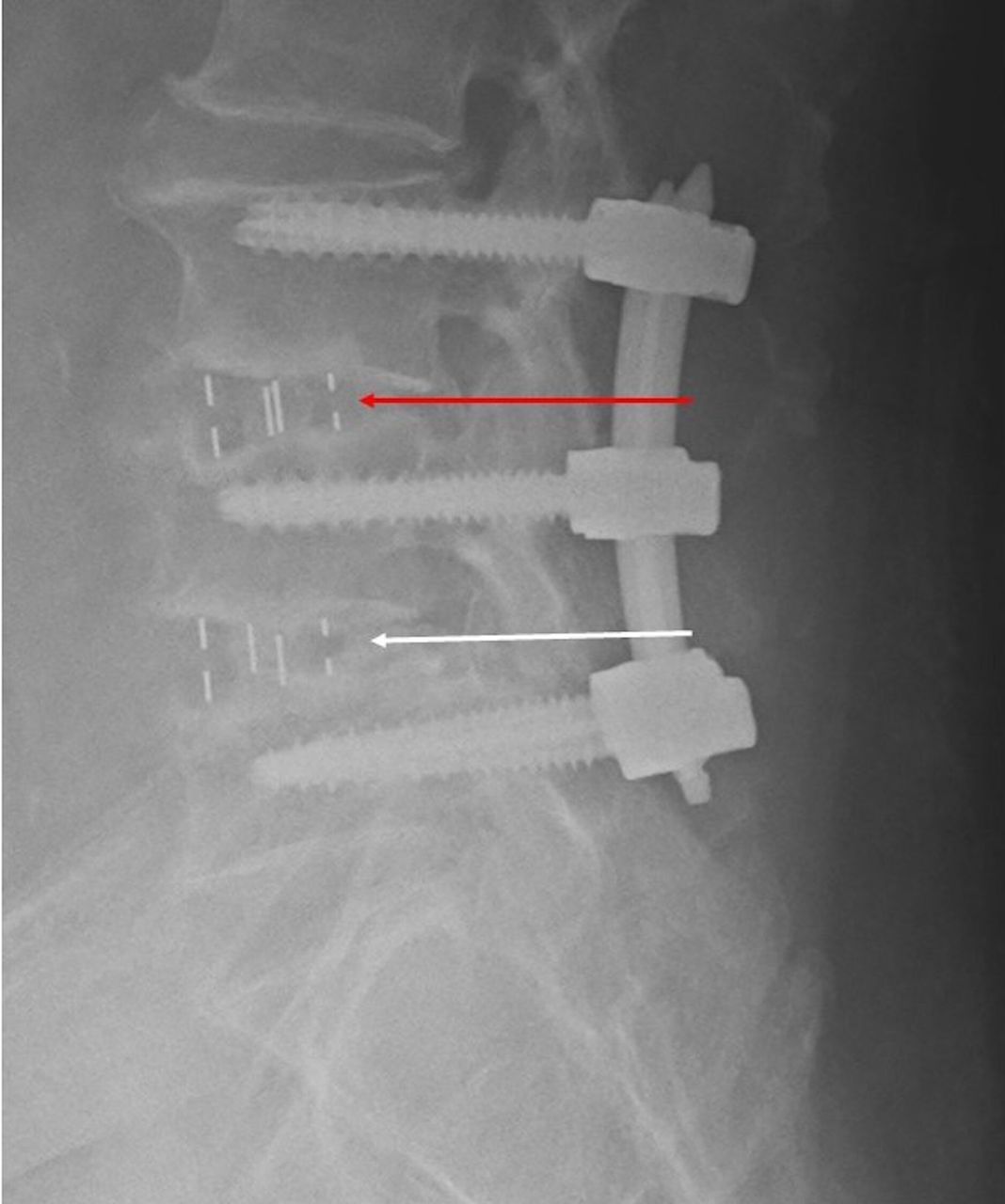
The segmental lordosis angle (SLA) was measured between the inferior endplate of the upper vertebra and the superior endplate of the lower vertebra on preoperative and immediate postoperative radiographs. The measurements were done in accordance with recommendations by Kaliya-Perumal et al.4 Fusion was assessed based on postoperative CT images and categorized according to the Bridwell classification.9 Figure 2 shows complete fusion achieved in one of our patients. Subsidence was assessed based on postoperative radiographs and graded based on the Marchi classification.10 Figure 3 shows a case of subsidence from our patient pool.

Computerized tomographic image of the lumbar spine showing complete fusion on both the lateral (A) and anteroposterior (B) views.

Radiographs of the lumbar spine in the lateral view. At the L3/4 level, there is subsidence of the entire cage (red arrow), while at the L4/5 level, there is no subsidence (white arrow).
Statistical Analysis
Statistical analysis was performed using GraphPad Prism software version 8.0 for Windows (GraphPad Software, San Diego, CA, USA). The correlation between cage placement and fusion and subsidence rates was tested using Spearman’s correlation. Differences between outcome measures pre- and postsurgery were tested using the Wilcoxon test. A P value of <0.05 was considered statistically significant.
Ethical Statement
This study was approved by the Domain Specific Review Board, National Healthcare Group, Singapore (2023/00108). The requirement for written consent was waived.
Results
The study included 53 patients and 97 operated levels. There were 16 (30.2%) men and 37 (69.8%) women. The mean age of the patients was 67.5 ± 7.93 years. Other forms of demographic data, including body mass index, American Society of Anesthesiologists grade, history of smoking, and diabetes mellitus status, were also collected (Table 1). All patients had a minimum of 12 months of postoperative follow-up, and fusion was assessed using postoperative CT images obtained at a mean of 12.6 months after surgery.
Summary of patient and surgical details.
Cage Placement
Cage placement was assessed on immediate postoperative radiographs. In the sagittal plane, the cage was placed at a mean value of 1.9 ± 2.5 mm anterior to the middle of the vertebral body. Eight (8.25%) levels had cages placed in the anterior one-third of the vertebral body, and 89 (91.8%) were placed in the middle one-third of the vertebral body. In terms of cage obliquity, the cage was placed at a mean value of 4.2° ± 2.8° oblique from the horizontal axis. We further stratified this into 2 groups. The first group included cages placed within 0° to 5° from the horizontal axis, and the second included cages placed within 5° to 10° from the horizontal axis. There were 69 (71.1%) cages in the 0° to 5° group and 28 (28.9%) cages in the 5° to 10° group. These findings are shown in Table 2.
Positioning of interbody cages.
Fusion Rate
Fusion was assessed on postoperative CT at a mean of 12.6 months after surgery. The degree of fusion was classified based on the modified Bridwell fusion criteria, which are stratified as follows: Grade 1: Fusion with remodeling and trabeculae present; Grade 2: Graft intact, not fully remodeled and incorporated but no lucency present; Grade 3: Graft intact, potential lucency present at top and bottom of the graft; Grade 4: Fusion absent with collapse or resorption of the graft.9 Images of different grades of fusion in our patient pool are shown in Figure 4. Eighty-one levels (83.5%) achieved fusion with a Bridwell score of 1, 15 levels (15.5%) achieved a Bridwell score of 2, and 1 level (1.03%) achieved a Bridwell score of 3. None of our cases had a Bridwell score of 4. We considered a score of 1 or 2 as achieving fusion. Ninety-six (99.0%) operated levels achieved fusion. The mean Bridwell score was 1.1 ± 0.4 (Table 3).

Computed tomography images showing different degrees of fusion. (A) Complete fusion (Bridwell 1). (B) Intact graft without complete remodeling (Bridwell 2). (C) Lucencies are seen in both superior and inferior aspects (Bridwell 3) at the L2/3 level as indicated by the white arrow.
Postoperative fusion and subsidence rates.
Subsidence Rate
Subsidence was assessed on postoperative radiographs taken approximately 12 months after surgery. The degree of subsidence was classified based on the Marchi criteria for subsidence, which is stratified by the degree of subsidence into the vertebral body endplate: Grade 0: 0% to 24%; Grade 1: 25% to 49%; Grade 2: 50% to 74%; Grade 3: 75% to 100%.10 Eighty-one (83.5%) operated levels had a Marchi score of 0, 14 (14.4%) had a Marchi score of 1, and 2 (2.06%) had a Marchi score of 2. The mean Marchi score was 0.186 ± 0.44. We considered a Marchi grade of 0 to have minimal subsidence and a Marchi grade of 1, 2, or 3 to have significant subsidence. Eighty-one (83.5%) operated levels had minimal subsidence, while 16 (16.5%) levels had significant subsidence (Table 3).
Sagittal Alignment Correction
Sagittal alignment was assessed on preoperative and immediate postoperative lateral radiographs of the lumbar spine. The parameters used to evaluate sagittal alignment were the SLA and disc height (DH). The SLA is the angle measured between the inferior endplate of the upper vertebra and the superior endplate of the lower vertebra. DH is the distance measured between the anterior-most aspect of 2 adjacent endplates. There was good improvement in both SLA and DH. In terms of SLA, there was a statistically significant increase in the angle of 4.2° ± 5.7° (P < 0.0001). In terms of DH, there was also a statistically significant increase of 4.5 ± 3.8 mm (P < 0.0001; Table 4.
Measure of sagittal alignment correction.
Correlations
We assessed the correlation between cage placement and postoperative radiological outcomes. There did not appear to be any correlation between cage placement and the outcomes of fusion, subsidence, and correction of sagittal alignment correction. This is exhibited in both Tables 3 and 4.
Discussion
The introduction of the OLIF procedure by Hynes2 overcame the limitations of the direct lateral approach, namely the risk of a plexus injury, postoperative thigh pain, and the constraint of a high iliac crest. By using a bare area between the anterior border of the psoas and aorta, this “oblique” corridor could be widened for lateral access to the disc space of the lumbar spine. In recent years, there has been good evidence demonstrating the benefits of the OLIF procedure for spinal fusion. There is a reduced risk of psoas and lumbar plexus injury compared with other more direct lateral approaches.3 Studies have shown that OLIF is superior with regard to sagittal alignment correction as well as with greater degrees of segmental lordosis creation and DH restoration.11 There is also evidence showing that OLIF is superior to other forms of indirect decompression in terms of fusion rates.12
However, there remains some debate as to whether an oblique approach affects the position and orientation of the cage placement, which in turn impacts fusion rates and sagittal alignment. Some studies have reported that an asymmetrically placed cage can result in an unintended coronal malalignment.13 The larger cage is also designed to have more contact with the dense ring apophysis. However, if obliquely placed, the cage will have more contact with the weaker bone of the central endplate instead, which can predispose to higher rates of pseudoarthrosis and subsidence.5,6 An obliquely placed cage can also place the contralateral nerve root at risk of impingement and injury.14,15
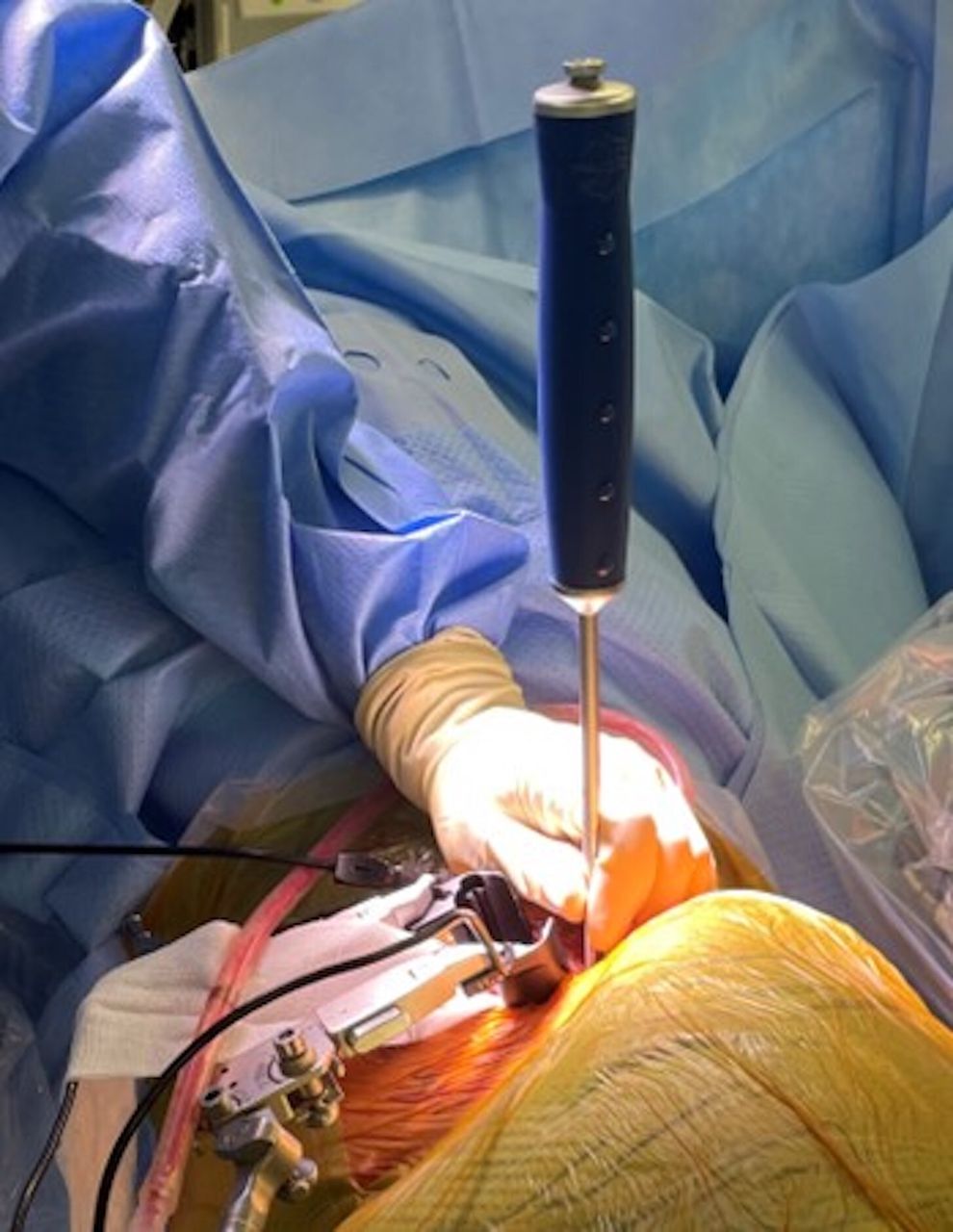
Our study showed that there will likely be a degree of obliquity in the cage placement in OLIF, but it can be kept to a minimum. A recent study by Park et al showed similar results with a mean cage obliquity of 11.3° ± 6.9° and showed that obliquity of greater than 20° was infrequent.5 Our findings were similarly reassuring with a mean cage obliquity of 4.2° ± 2.8°, and all our cages were placed within 10°. This reaffirms the work done by Park et al but also adds on further to their work by evaluating more patients from a different population. When performing the OLIF approach, a bulky psoas, high iliac crest, and close proximity of iliac vessels to the psoas muscle can influence the ease of cage insertion as well as the final obliquity of the cage. The surgeon’s skill and familiarity with the approach also determine his ability to mitigate these factors and navigate the way to the disc space to perform a proper discectomy and cage insertion. Our surgical technique is different in that we tend to perform the orthogonal rotation maneuver outside of the disc space, rather than within the disc (Figure 5). This allows for us to perform a “smoother turn” compared with rotating the cage within the disc space which can be narrow, hindering the degree of rotation we can achieve especially with a larger cage. This may have contributed to the lower degree of rotation seen in our patient pool.

Intraoperative photo showing the author’s maneuver for orthogonal rotation of the cage. Note that while the retractor is placed obliquely, the maneuver is performed outside the disc space.
To date, there are few studies showing a clear relationship between cage placement and the incidence of pseudoarthrosis and subsidence. Our study demonstrates that there is statistically no strong correlation between the degree of cage obliquity and rates of fusion or subsidence (P = 0.293 and 0.931, respectively). We also demonstrated that there is no statistically strong correlation between malpositioning of the cage in the sagittal plane and rates of fusion or subsidence (P = 0.0638 and 0.474, respectively). Park et al similarly showed that cage obliquity did not have any statistically significant impact on fusion rate and attributed a higher subsidence rate to cage height rather than placement.5
Our findings, based on Marchi grading, showed that subsidence was relatively common and is to be expected in OLIF. However, most of these cases were mild and went on to achieve complete fusion. Eighty-one levels had minimal subsidence with a Marchi score of 0. At the same time, 16 levels had significant subsidence with a Marchi score of 1 or higher. However, only 2 levels had more severe subsidence with a Marchi score of 2. Of these 2 levels, only 1 progressed to pseudoarthrosis, while the other ended up achieving complete fusion. The 1 case of pseudoarthrosis had other contributing factors, including a significant smoking history, the absence of usage of bone morphogenic protein, and instrumentation with a long construct that may confound the relationship between subsidence and fusion. Overall, our data reaffirm current literature that although OLIF has a relatively higher subsidence rate, it still enjoys a high rate of fusion and is a powerful minimally invasive technique for lumbar interbody fusion.3,15–17
Our results also showed that OLIF was effective in correcting sagittal deformity. We demonstrated an increase in SLA of 4.2° ± 5.7° (P < 0.0001) and in DH of 4.5 ± 3.8 mm (P < 0.0001). Jin et al demonstrated a 5.5° increase in SLA and a 5-mm increase in DH, while Shiga et al showed a 3.8° increase in SLA.18,19 These are similar to our results. Additionally, we showed that there was no statistically significant correlation between greater cage obliquity and the increase in SLA or DH (P = 0.931 and 0.111, respectively). Again, this demonstrates that a small degree of obliquity of the cage does not affect the correction of sagittal deformity.
Limitations
This study is not without limitations. This is a retrospective study with a limited sample size. Patients had a relatively short follow-up time of 1 year. Although this period can be considered sufficient to assess the outcome in terms of fusion, longer follow-up may have given additional information. Additionally, the study did not account for factors such as smoking, osteoporosis, and steroid use, which may have influenced the outcomes. Integrating these factors into future studies would contribute to a more comprehensive understanding. Furthermore, none of the patients included in this study exhibited higher degrees of obliquity. Hence, the outcome in such patients remains to be understood.
Conclusion
Our findings highlight that OLIF enables appropriate cage placement, with a very minimal cage obliquity, usually below 20°. This minimal obliquity does not correlate with reduced fusion rates, heightened subsidence, or sagittal malalignment. It was also noted that subsidence was common and is to be expected in OLIF. However, it does not necessarily impact fusion outcomes, as evidenced by complete fusion in most of the patients included in this study. These findings emphasize the safety profile of OLIF, positioning it as a reliable and effective lumbar fusion technique.
Acknowledgments
The study team would like to acknowledge Dr. Arun Kumar Kaliya Perumal for providing his invaluable insight and ideas as well as assisting with the proof reading and editing of the manuscript.
Footnotes
Funding No funding was received for this study.
Declaration of Conflicting Interests Each author certifies that neither he or she, nor any member of his or her immediate family, have funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Institution Review Board Approval This study was approved by the Domain Specific Review Board, National Healthcare Group, Singapore (2023/00108). The requirement for written consent was waived.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.