


Abstract
Background Anterior lumbar interbody fusion (ALIF) has emerged as a valuable technique for managing lumbar degenerative conditions and revision surgeries, particularly for addressing complications associated with transforaminal lumbar interbody fusion (TLIF) and posterior lumbar interbody fusion (PLIF) cages. However, there is limited evidence documenting its safety and feasibility in the context of revision procedures involving cage removal.
Objective To evaluate intraoperative outcomes of ALIF for TLIF/PLIF cage removal, focusing on complications, surgical times, and blood loss in a substantial case series.
Methods This case series analyzed data from 135 patients who underwent ALIF for TLIF/PLIF cage removal between January 2019 and May 2023. Surgical indications included pseudarthrosis, cage migration, and infection. Outcomes assessed included intraoperative complications, surgical duration, and estimated blood loss.
Results Of the 135 patients (median age: 47 years, range: 15–78), vascular injuries occurred in only 4 cases, all involving the left iliac vein, and were managed intraoperatively without sequelae. No injuries to retroperitoneal, neural, or organ structures were observed. Median surgical time was 100 minutes (range: 50–210), with most cases resulting in less than 150 mL of blood loss. These findings demonstrate the feasibility of ALIF for managing TLIF/PLIF complications.
Conclusion ALIF is a safe and effective option for revision surgeries involving TLIF/PLIF cage removal, offering a low complication profile and manageable intraoperative challenges. A critical factor contributing to these favorable outcomes is the multidisciplinary approach, where the collaboration between access and spine surgeons ensures meticulous handling of anatomical and vascular challenges.
Clinical Relevance This study provides valuable data for further prospective research to explore long-term outcomes and refine surgical techniques.
Level of Evidence 4.
Introduction
Surgeries addressing lumbar spine disorders are among the most executed interventions in modern medicine, offering substantial relief and functional restoration to patients afflicted with degenerative or structural spinal conditions. However, despite their prevalence and effectiveness, these procedures carry inherent risks that are magnified in revision contexts.1,2 Complications, such as vascular injuries, neural compromise, pseudarthrosis, and cage migration, pose significant obstacles for surgeons and patients.3,4 An understanding of these challenges is essential to advancing both surgical practices and patient outcomes in spinal care.
Within this domain, anterior lumbar interbody fusion (ALIF) has emerged as a pivotal technique for managing lumbar degenerative diseases. Unlike posterior approaches, ALIF leverages an anterior pathway, sparing the posterior spinal anatomy and thereby preserving critical paraspinal musculature and neural structures.5 This approach offers several notable advantages: it enables more precise sagittal alignment correction, achieves higher fusion success rates, and provides superior access to intervertebral disc spaces, particularly in the lower lumbar regions.6,7 However, these benefits are accompanied by considerable risks. The surgical proximity to major vascular structures introduces a heightened likelihood of vascular injuries, necessitating rigorous preoperative planning and meticulous intraoperative attention.2,4 Revision surgeries further complicate this scenario, as scar tissue and altered anatomical landscapes amplify the technical challenges involved.8
The removal of transforaminal lumbar interbody fusion (TLIF) or posterior lumbar interbody fusion (PLIF) cages in revision surgeries presents an intricate surgical landscape. Scar tissue from previous operations frequently obscures vital anatomical landmarks, increasing the difficulty of navigation and the risk of intraoperative complications.9 Furthermore, retrospective studies have highlighted how improper placement or migration of interbody cages can disrupt spinal alignment and compromise fusion efficacy, necessitating even more strategic surgical planning.10,11 Managing the iliolumbar vein poses a critical challenge in anterior lumbar techniques, demanding heightened precision in vascular manipulation, especially in the more complex revision scenarios.3,12
Despite these challenges, ALIF has demonstrated promise as a preferred technique in revision surgeries, offering robust biomechanical stabilization and the ability to bypass posterior scarring.3,5,12,13 The anterior approach not only facilitates spinal alignment but also enhances the fusion surface area, optimizing the potential for successful outcomes even in technically demanding cases.5,6
The biomechanical principles underlying ALIF contribute significantly to its success. By maximizing the contact area for fusion and allowing for optimal lordotic correction, the technique strengthens spinal stability and alignment. Such attributes are invaluable in revision cases, where the complexity of the surgical environment demands precision and adaptability.5,6 Nonetheless, the specific technical difficulties associated with revision ALIF, especially those involving the removal of TLIF or PLIF cages, remain inadequately explored. While primary ALIF procedures have been extensively studied, a comprehensive examination of their safety and efficacy in revision settings is critical to guiding clinical decision-making and refining surgical methodologies.
This study seeks to address the knowledge gap by systematically analyzing intraoperative complications associated with ALIF in revision surgeries that involve the extraction of TLIF and PLIF cages. Key variables, such as vascular injury, operative durations, and procedural complexities, will be assessed within a robust case series. By illuminating these aspects, this research aspires to provide actionable insights, inform surgical planning, and ultimately improve outcomes for patients navigating the challenges of complex lumbar spine disorders.
Methods
Study Design and Setting
This investigation was designed as a retrospective case series and conducted at the Aécio Dias Access Institute (IAAD). The study reviewed 3438 ALIF procedures performed between January 2019 and May 2023. The database was populated in real time during each procedure, with surgical details entered contemporaneously by trained personnel, ensuring high accuracy and data integrity. This approach eliminated the need to access physical or digital hospital records, providing a reliable and secure source of information for this study. Furthermore, the real-time data entry process minimized errors, offering an invaluable resource for clinical research.
Patient Selection
From this dataset, 135 surgeries were selected according to strict inclusion criteria, focusing exclusively on revision cases involving the removal of TLIF or PLIF cages. These revisions were indicated due to complications from the prior procedures, such as cage migration, pseudarthrosis, or infection. Only adult patients aged 18 years or older were included, while pediatric patients and those undergoing surgeries for indications other than TLIF/PLIF cage removal were excluded to ensure a homogeneous study population (Figure 1).

Patient selection.
Surgical Technique
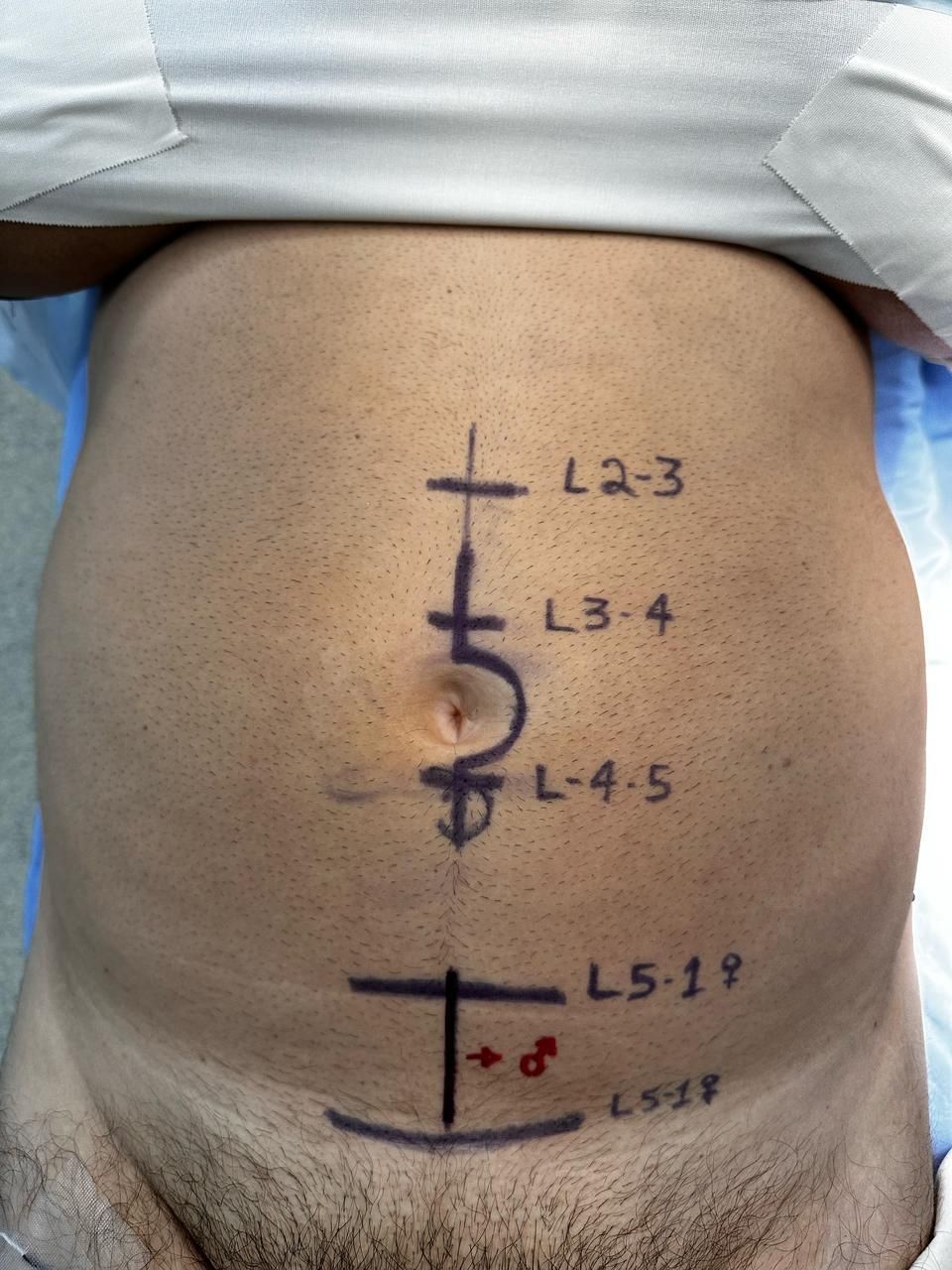
For ALIF surgery with cage removal, the patient is positioned in the supine position under general anesthesia, with arms crossed over the chest to facilitate the positioning of the fluoroscopy arm. A cushion is also placed under the thighs to relax the psoas muscles, and intermittent pneumatic compression and electroneural electromyographic monitoring are used when indicated. The technique employed by the IAAD involves a median longitudinal incision to avoid damaging nerves and vessels in the abdominal wall. An exception is made for women undergoing surgery at the L5 to S1 level, where a Pfannenstiel incision—a transverse suprapubic incision—is preferred for better aesthetic outcomes. The approach is typically performed on the left side of the patient, except for isolated surgeries at L5 to S1, which are performed on the right side (Figure 2).9,10,14

Median longitudinal incisions in the abdomen for anterior lumbar interbody fusion (ALIF).
The incision is performed in planes, sequentially opening the skin, subcutaneous tissue, and the rectus abdominis muscle sheath. The aponeurosis of the external oblique muscle and the anterior layer of the aponeurosis of the internal oblique muscle are opened. The rectus abdominis muscle is identified and retracted anterolaterally using modified Langenbeck retractors adapted by Aécio Dias (Figure 3). The epigastric vessels are identified and retracted anteriorly along with the rectus abdominis muscle, avoiding the need for ligation. Blunt dissection is performed cranially through the posterior layer of the aponeurosis of the internal oblique muscle until its insertion into the muscle. Access to the retroperitoneum is achieved through sectioning of the posterior rectus sheath, with careful reflection of the peritoneum and intraperitoneal structures to avoid injury.9 At this stage, the psoas muscle, common iliac artery, and ureter are exposed.14

Aecio Dias retractors positioned for the L4 to L5 levels.
For the L5 to S1 level, the promontory is palpated to locate a space between the iliac vessels. This space is dissected, and the middle sacral vessels, typically 1 artery and 1 or 2 veins, are ligated to improve exposure. The ureter, which crosses the anterior surface of the common iliac artery at its bifurcation, is carefully preserved. The Aécio Dias retractors are positioned using 3-mm Steinmann/Kirschner wires at L5 (lower quadrant) and S1 (upper quadrant) to provide wide access to the L5 to S1 disc. If Aécio Dias retractors are unavailable, long Langenbeck retractors secured with elastic bands or Steinmann wires alone can be used for thinner individuals.9,14
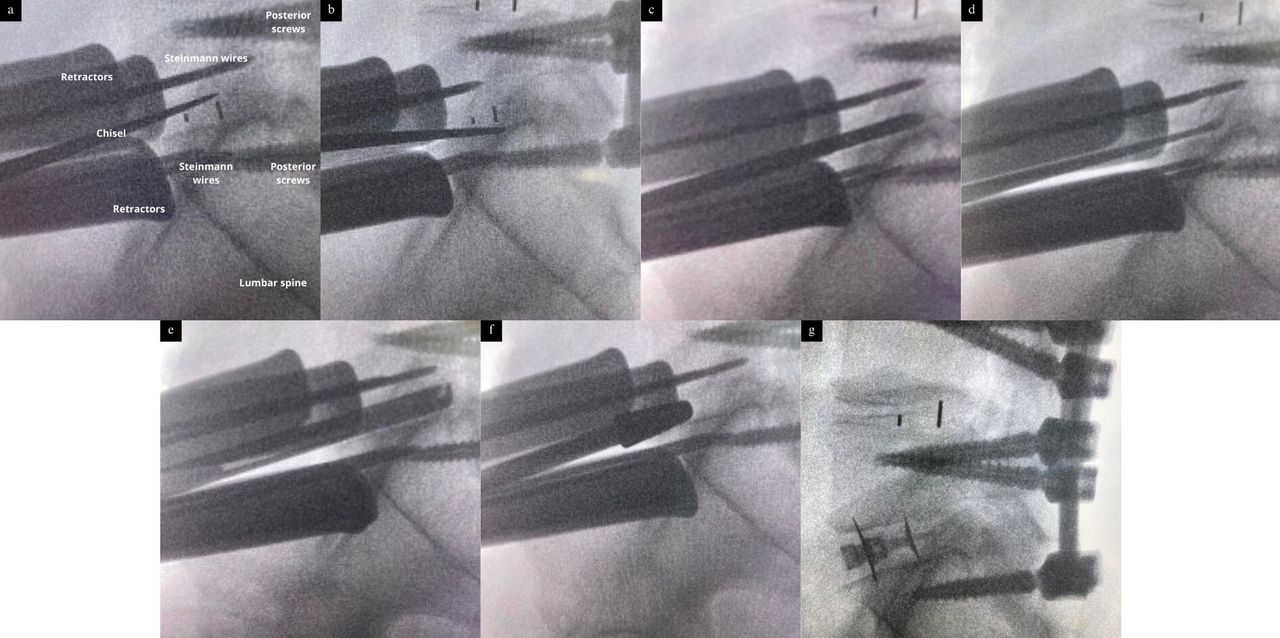
At L4 to L5 and more cranial levels, access is achieved on the left side of the distal abdominal aorta and the left common iliac artery. Dissection is performed laterally to the left common iliac vein, left common iliac artery, and abdominal aorta. These vessels are carefully displaced medially to avoid injury to the arteries, veins, ureters, and sympathetic fibers. The iliolumbar vein is identified and ligated if necessary, especially when accessing the L4 to L5 level.2 Once the levels are exposed, the anterior longitudinal ligament (ALL) is sectioned, followed by excision of the fibrous ring and nucleus pulposus using curettes and forceps. The TLIF/PLIF cage, often attached by fibrotic bands, is identified and released by carefully chiseling around its edges. The device is removed from its bed using a gouge, after which the disc space is thoroughly cleaned. The wider surgical field achieved through the anterior approach allows for the placement of an ALIF cage under fluoroscopic guidance. The procedural steps are outlined in Figure 4.14 The surgery concludes with a hemostatic review and closure of the anterior rectus abdominis sheath, subcutaneous tissue, and skin (Figure 5).

Step-by-step process of cage removal. (a) Release of the upper plateau cage with a chisel. (b) Release of the lower plateau cage with a chisel. (c) Cleaning of the disc space with forceps. (d) Cleaning of the disc space with a curette. (e) Cleaning of the disc space with Kerrison forceps. (f) Positioning the trial. (g) Positioned cage.

Final result of the removal of transforaminal lumbar interbody fusion (TLIF)/posterior lumbar interbody fusion and placement of anterior lumbar interbody fusion (ALIF) cage. (a) Visualization of the ALIF cage. (b) Visualization of the ALIF cage after removal of retractors from the major vessels. (c) TLIF cage removed.
Data Collection
Pertinent demographic and clinical data, such as age, sex, body mass index, and primary indications for surgery, were retrieved from the institute’s database. Primary outcomes assessed intraoperative complications, such as vascular injuries, retroperitoneal or intraperitoneal organ damage, and neural injuries involving the dural sac or nerve roots. Secondary outcomes included surgical duration, measured from skin incision to wound closure, and estimated blood loss, determined through gauze weight differentials and aspirator volume calculations. These metrics were rigorously documented to ensure reliability.
Statistical Analysis
This study employed descriptive statistics to summarize the operative outcomes of ALIF procedures. Measures of central tendency (mean and median) and dispersion (SD and interquartile range) were calculated for continuous variables, while absolute and relative frequencies were used to describe categorical variables. All analyses were performed using the Jamovi software (version 2.3.28.0). Results are presented in tables and figures to ensure clarity and facilitate interpretation.
Ethical Considerations
This study was approved by the Prevent Senior Research Ethics Committee (approval number: 85722024.0.0000.8114), which ensures compliance with ethical standards for research involving human subjects. Informed consent was waived due to the retrospective nature of the study and the use of anonymized data.
Results
Study Characteristics
A total of 135 patients who underwent ALIF procedures for the extraction of TLIF/PLIF cages were included in the evaluation. The group comprised 68 men and 67 women, with a median age of 47 years and an age range of 15 to 78 years. Body mass index categories for these patients are outlined in Table 1.
Baseline demographic and clinical characteristics of patients undergoing ALIF for TLIF/PLIF cage removal (N = 135).
The primary surgical indications included pseudarthrosis (107 patients, 79.3%), cage migration or compression (23 patients, 17%), and infection (5 patients, 3.7%). Patient-reported symptoms included axial low back pain and sciatic pain, which was present in 74 patients. Axial pain alone was reported in 57 patients, while 4 patients experienced only sciatic pain. The levels operated ranged from 1 to 4, with single-level procedures being the most frequent. Detailed information about operated levels is summarized in Table 1.
Intraoperative Findings
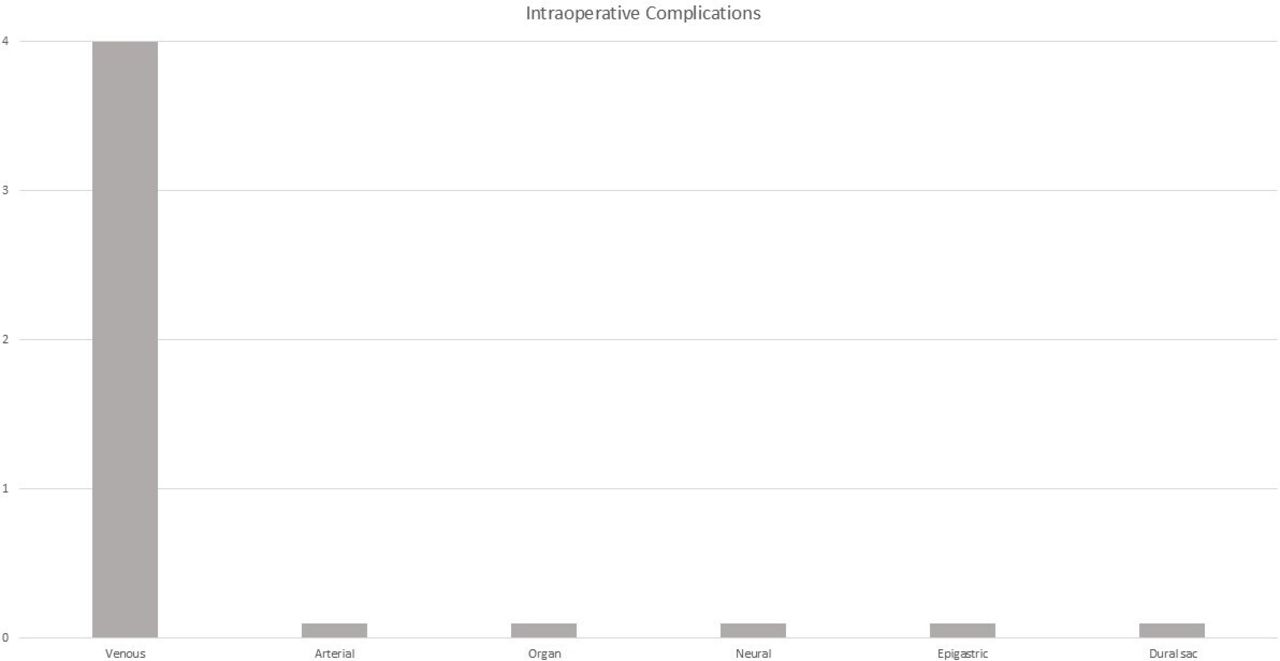
Intraoperative complications were infrequent, with only 4 vascular injuries reported, all involving lacerations of the left iliac vein during dissection. Three cases were managed with sutures, while 1 case achieved hemostasis using a barrier hemostat. There were no injuries to arteries, epigastric vessels, intraperitoneal or retroperitoneal organs, dural sacs, or nerve roots.
Operative times ranged from 50 to 210 minutes, accompanied by blood loss values of 20 to 520 mL. Table 2 offers a comprehensive breakdown of these metrics alongside intraoperative complications, visually highlighted in Figure 6.

Intraoperative complications in anterior lumbar interbody fusion for transforaminal lumbar interbody fusion/posterior lumbar interbody fusion cage removal.
Summary of intraoperative outcomes (N = 135).
Discussion
Principal Findings
This case series evaluated the intraoperative outcomes of ALIF in revision surgeries involving the removal of TLIF or PLIF cages. The findings revealed low complication rates, efficient surgical durations, and minimal intraoperative blood loss. Only 4 vascular injuries were observed, all involving the left iliac vein, and each was successfully managed intraoperatively. No neural, organ, or additional vascular injuries were documented. Operative times ranged from 50 to 210 minutes, with blood loss ranging from 20 to 520 mL. These results highlight ALIF as a safe and effective surgical option for addressing complications such as pseudarthrosis, cage migration, and infection following TLIF/PLIF procedures.
Vascular and Neural Injuries
Vascular injuries, particularly involving the left iliac vein, are a recognized challenge in ALIF due to the vessel’s proximity to the surgical field. This study’s venous complication rate aligns with prior literature reporting rates of 0.8% to 4.3%, highlighting the importance of meticulous surgical technique.2 Effective management of vascular complications, facilitated by preoperative planning and surgical precision, contributed to the low morbidity observed. Arterial injuries were not encountered in this study, which is consistent with other reports demonstrating their relative rarity.10
In revision cases, inflammatory responses and adhesions involving the ALL, presacral fascia, and major vessels are notable challenges. Such adhesions often involve neural structures like the dural sac and nerve roots, necessitating careful dissection and tailored surgical strategies to minimize risks and ensure successful outcomes.15 Although we did not objectively quantify inflammation and adhesions involving the ALL, our experience suggests that they were present in most cases.
Other Complications
Neural and dural sac injuries were not observed in this study, corroborating prior reports of ALIF’s safety in minimizing neural manipulation due to its anterior approach. Fortunately, the vast majority of cages are made of PEEK, an inert material that does not adhere to these adjacent planes. Additionally, organ injuries, such as ureteral or intra-abdominal damage, were not documented, supporting the procedure’s safety when performed with meticulous surgical planning and technique.11
The surgical efficiency observed in this case series aligns with existing literature, with operative times ranging from 50 to 210 minutes and blood loss predominantly below 150 mL.14 These findings reflect the benefits of standardized surgical protocols and experienced teams in optimizing intraoperative outcomes.6,15
Clinical Implications
These findings substantiate ALIF as a practical and reliable technique for complex revision cases. The anterior approach provides direct access to the lumbar spine, enabling the removal of failed cages and placement of new interbody devices while minimizing risks associated with posterior scarring and neural complications. The expertise of access surgeons is particularly critical in these procedures. Their specialized skills in navigating vascular anatomy and managing adhesions involving the presacral fascia and major vessels play a central role in minimizing complications and enhancing procedural efficiency.6
Tips and Tricks
In revision ALIF cases requiring TLIF removal, proper planning and technique are essential to optimize outcomes. One key preoperative step is ensuring that the primary surgeon fully mobilizes the TLIF using an osteotome. Even when the TLIF appears loose, residual fixation points often remain, requiring additional release to prevent complications. A common concern is the potential migration of the cage into the spinal canal during mobilization, but when performed correctly, the technique is both safe and effective.
Intraoperatively, proper fluoroscopic alignment is crucial. Immediately after the anterior discectomy and initial curettage, a lateral x-ray should be obtained to align the vertebral endplates. The osteotome should be positioned superiorly and inferiorly to the TLIF in 3 directions: medial, right oblique, and left oblique. This ensures a thorough release before attempting extraction. To preserve endplate integrity, the osteotome should be carefully positioned along the superior and inferior cage borders. Once the TLIF is removed, the remaining discectomy should start at the lateral disc space, as these areas are less affected by subsidence and provide stronger endplate support.
If the TLIF is positioned posteriorly or laterally, adhesion to neural structures such as the dura and nerve roots is more likely, increasing the risk of injury. In such cases, the use of an operating microscope can aid in careful dissection. Additionally, significant subsidence can make cage extraction more challenging, as the implant may be deeply embedded within the endplates.
Preoperative imaging plays a vital role in planning. If the TLIF appears highly anterior and close to major vessels, computed tomography angiography or magnetic resonance angiography should be performed to assess vascular risk. Additionally, computed tomography scans and dynamic radiographs are essential to evaluate pseudarthrosis and endplate condition, as these factors influence surgical strategy.
The step-by-step approach for TLIF removal during ALIF follows a standard sequence: after initial discectomy, the TLIF is mobilized using a Cobb elevator or osteotome, with a curette to release any residual adhesions. The cage is then extracted using a long, thin rongeur or curette to minimize force. Once removed, the discectomy is completed as in a routine ALIF.
To optimize outcomes, surgeons should prioritize complete TLIF mobilization, ensure precise fluoroscopic alignment, consider microscope use when facing severe adhesions, and obtain preoperative imaging to assess vascular proximity and pseudarthrosis. Additionally, all procedures in our study were performed with the assistance of an access surgeon. Based on our experience, their presence was of paramount importance in ensuring surgical success and played a key role in the low morbidity observed in our series. The access surgeon’s expertise contributed to safer vascular manipulation, improved exposure, and overall procedural efficiency, reinforcing the value of a multidisciplinary approach in complex revision cases.
Defining an appropriate strategy for managing posterior instrumentation is essential when performing anterior removal of interbody cages. A frequent question is whether the pedicle screw-rod construct should be released prior to the anterior approach. The answer depends on the surgical indication. In cases where the primary diagnosis is pseudarthrosis—especially at levels that still retain some disc height—there is no need for prior release of the posterior fixation, and the anterior approach can be performed first. On the other hand, in patients whose indication for cage removal is due to its migration into the vertebral canal or foramen, without signs of pseudarthrosis and with significantly reduced or absent disc space, it is advisable to release the posterior instrumentation before the anterior approach. This facilitates safe implant removal and helps prevent additional injury.
Strengths and Limitations
This study’s primary strength lies in its robust dataset, providing detailed insights into intraoperative outcomes in revision surgeries. The inclusion of a large case series enhances statistical reliability and relevance. The study was conducted at a high-volume center where a multidisciplinary team, including vascular and spine surgeons, played a central role in minimizing complications and ensuring consistent outcomes. These collaborative efforts contributed to procedural efficiency, particularly in addressing the anatomical challenges and vascular risks inherent to ALIF.6
However, certain limitations must be acknowledged. The retrospective design precludes the evaluation of long-term outcomes, such as fusion rates and functional recovery, and relies on data previously recorded in the institutional database. Additionally, the focus on a single specialized center may restrict the generalizability of these findings to settings with differing surgical practices and case volumes. Future studies should address these limitations by including broader populations and multicenter data.15
Future Directions
Future research should prioritize prospective, multicenter studies to validate these findings in diverse clinical settings and evaluate long-term outcomes, including fusion success and patient-reported recovery. A key area for further exploration is the management of vascular adhesions and neural complications, particularly in patients with prior surgeries, where anatomical alterations increase procedural complexity. Additionally, the absence of randomized controlled trials evaluating the safety and efficacy of ALIF highlights a significant gap in the literature that future studies should aim to address. Such investigations would provide higher-quality evidence to refine surgical strategies and optimize outcomes in both primary and revision ALIF procedures.15
Conclusion
This study addresses a critical gap in spinal surgery research by analyzing the role of ALIF in revision surgeries requiring TLIF or PLIF cage removal. The findings affirm ALIF’s safety and feasibility in managing complex spinal conditions while preserving essential anatomical structures. A critical factor contributing to these favorable outcomes is the multidisciplinary approach, where the collaboration between access and spine surgeons ensures meticulous handling of anatomical and vascular challenges. The expertise of these teams not only minimizes intraoperative morbidity but also enhances procedural efficiency and patient safety.
Through a detailed assessment of a large patient group, this research underscores the utility of ALIF in addressing unique challenges associated with revision surgeries. Future research should focus on long-term fusion success and recovery metrics to further optimize ALIF as a preferred method for revision spinal procedures.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.