


Article Figures & Data
Figures
- Figure 1
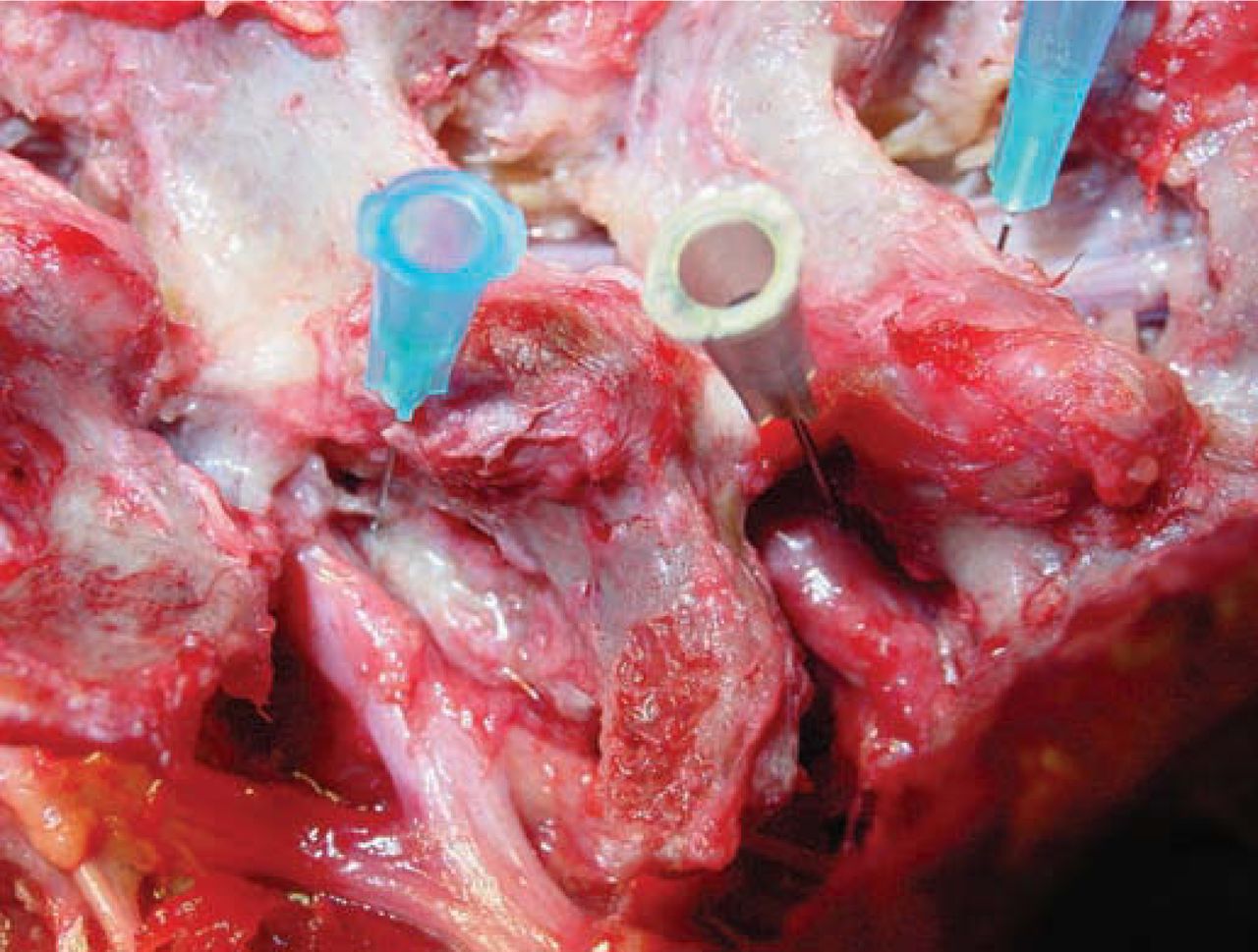
Foraminal view of cadaver dissection at L4–5 and L5–S1. Note the tiny furcal nerve branch speared by the blue hubbed needle that branches from exiting L4 nerve at L4–L5. The nerve seen in Figure 5b would be what a small furcal branch looks like, but in this instance, excisional biopsy confirmed by pathology slide revealed the nerve to be an autonomic nerve because of the ganglia seen on the slide. These furcal nerves in the “hidden zone” of MacNab vary in size and can cause postoperative dysesthesia. When the nerve is equivalent in size to the spinal nerve, it can be interpreted as a conjoined nerve if it cannot be traced back to its origin.
- Figure 2
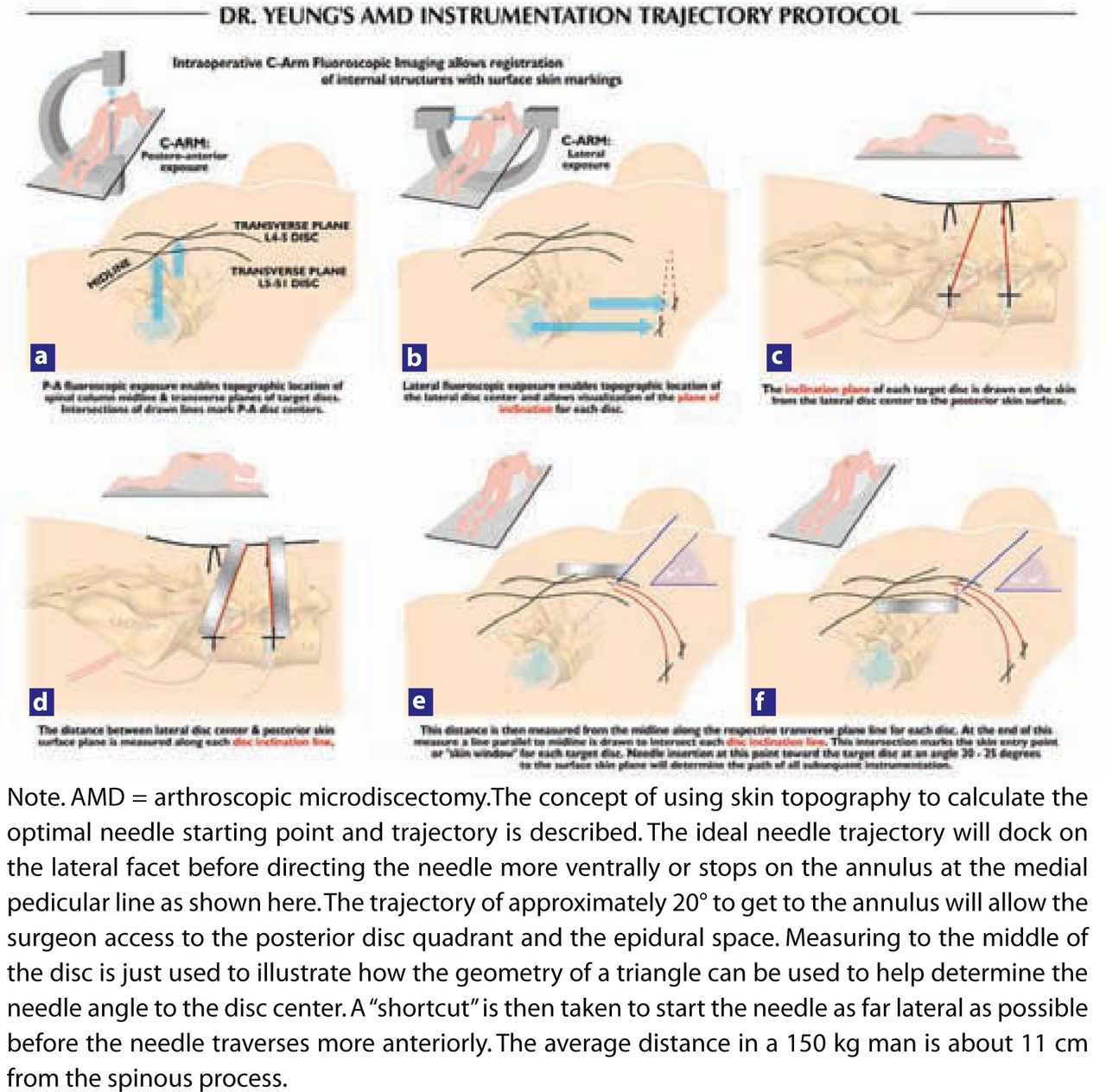
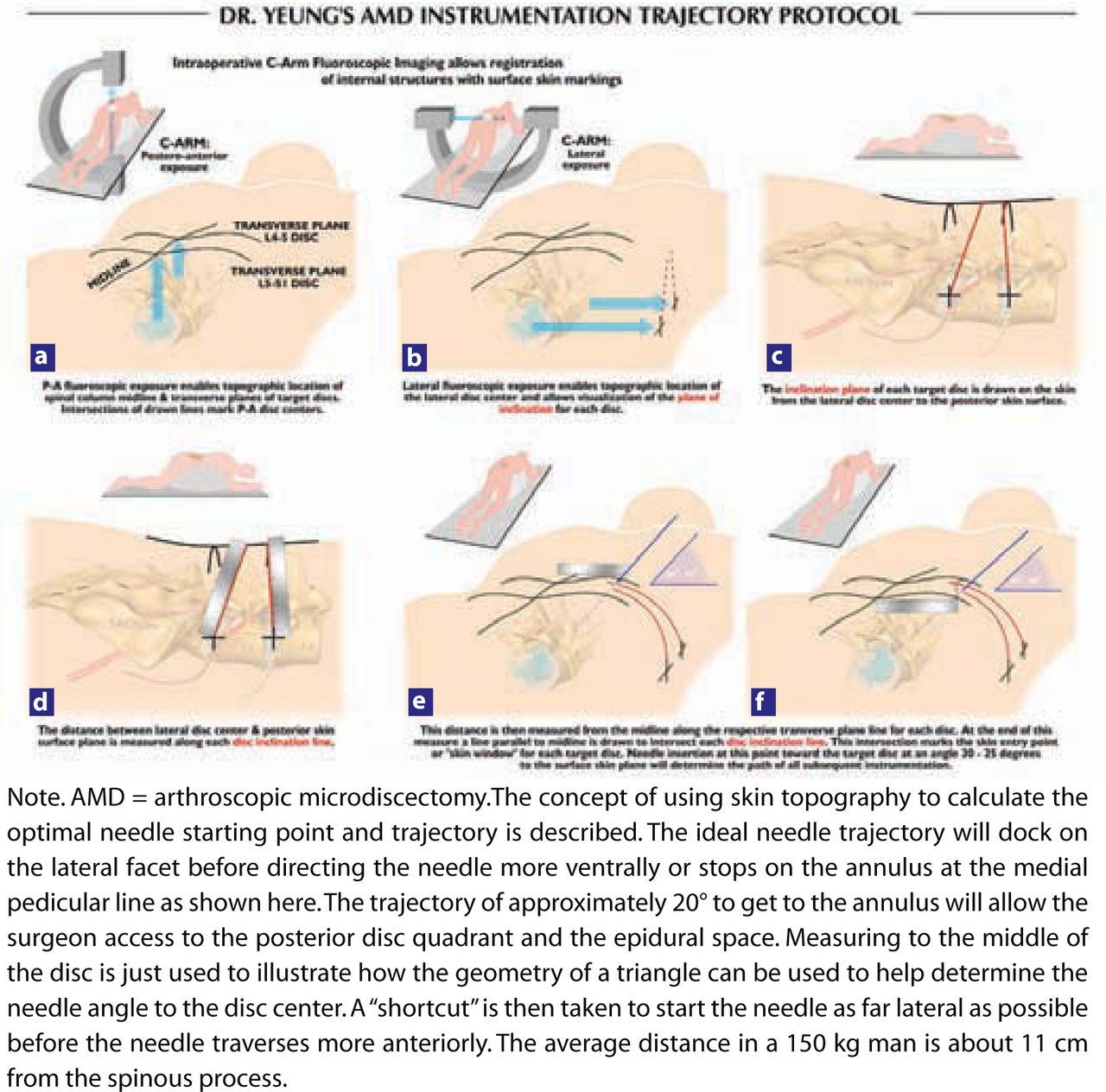
Protocol for drawing lines for optimal skin window in foraminal endoscopic surgery: (a–e) The procedure is carried out in an operating room under aseptic conditions, with use of only local anesthesia and conscious sedation. (Do not use propofol!) Free hand C-arm biplane guidance method is used. Two basic C-arm projected images are utilized, postero-anterior and lateral projections. Both views require parallelism of the X-ray beam to target the endplates. When the intervertebral disc is not perpendicular to the floor, the C-arm tube is tilted until the beam (dotted line) is parallel to the disc endplates, i.e., at L5–S1 (Ferguson view). The skin window is estimated by measuring the distance from the anterior disc to the skin or by placing the skin window as far lateral on the back as possible before the skin window goes directly anteriorly. (f) From the skin window aim the approach needle toward the posterior disc quadrant at approximately 20° in the frontal plane. The path is medial to the quadratus lumborum. This avoids inadvertent visceral penetration. The trajectory places the posterior third of the disc and the epiannular space within reach of the operating tools. Use a more vertical angle if an epidural procedure is not needed. Enter the disc through the annular window and place the needle tip in the midline. In the lateral projection, the needle need not pass the midpoint of the disc. Evocation contrast or indigo carmine discography is performed in this position.
- Figure 3
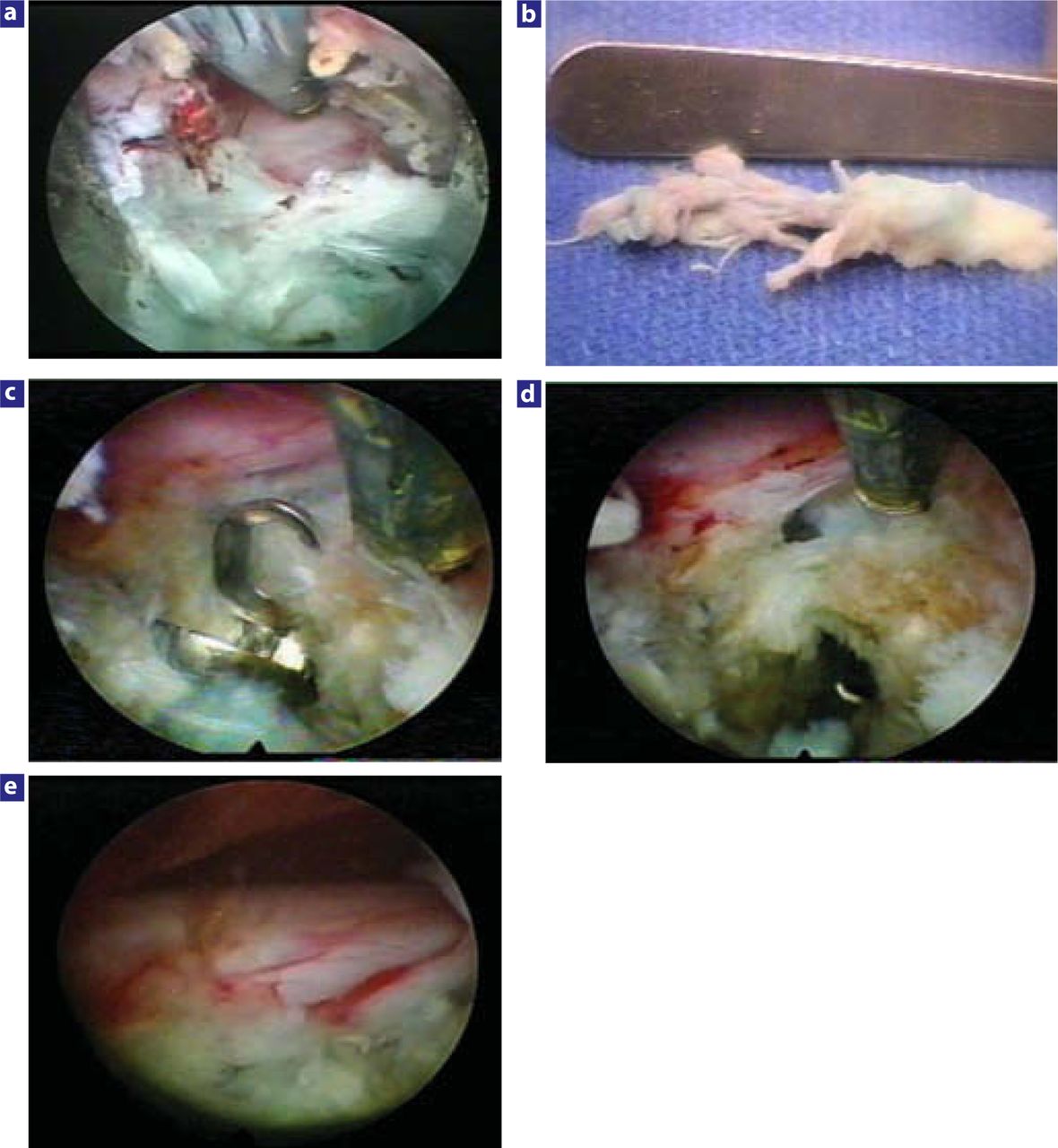
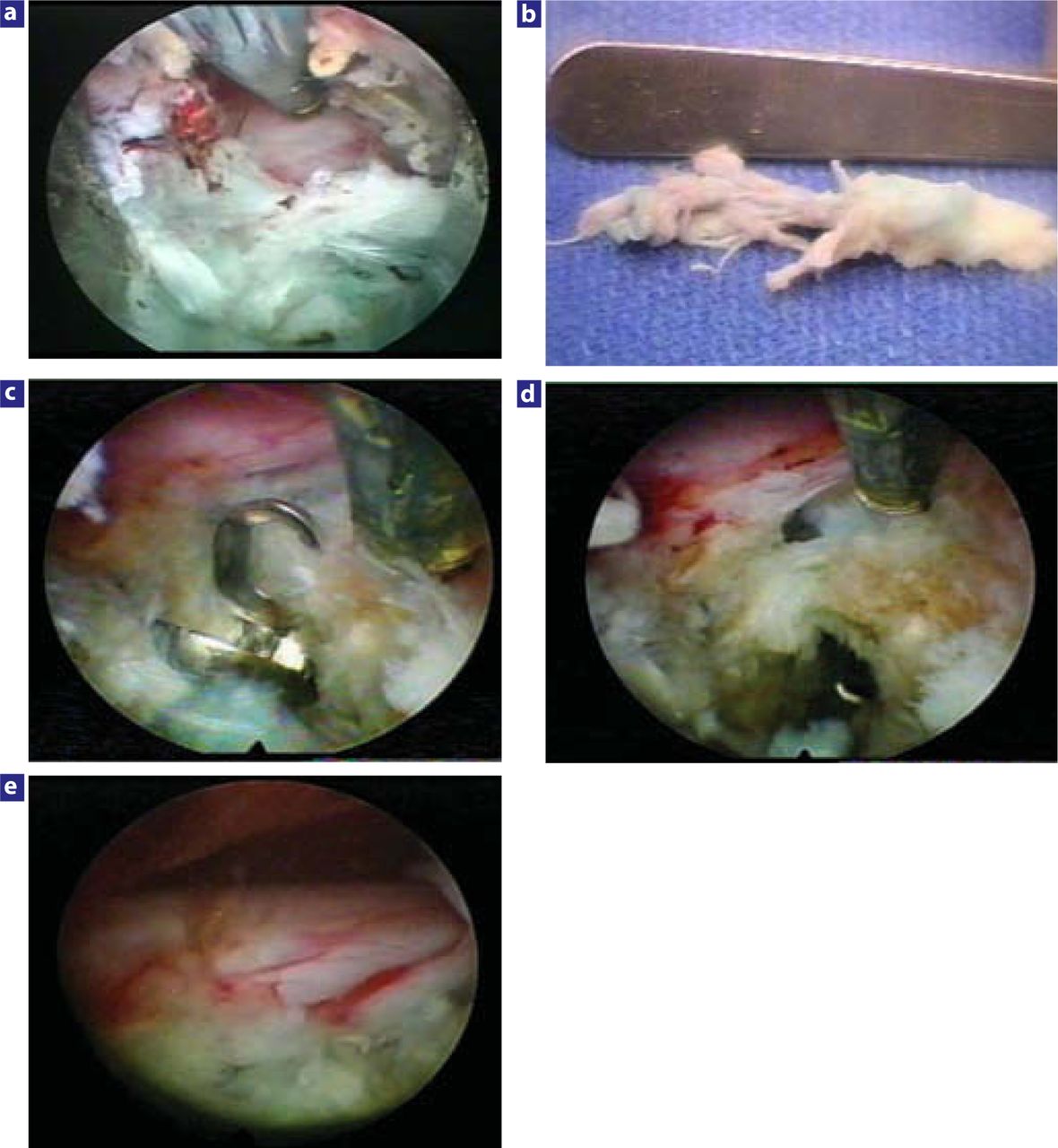
Examples of nerve decompression for extruded disc herniations with the uniportal and biportal technique: (a) Foraminal view of the decompressed L5 nerve after endoscopic extraction of a large extruded disc fragment at L4–L5. The posterior longitudinal ligament and posterior annulus are still shielding the ventral aspect of the traversing nerve. (b) Foraminal fragment extracted from beneath and lateral to the traversing L5 nerve seen in Figure 3a. The fragment was extracted through a uniportal approach, but large paracentral and central herniations are indications for a biportal approach. (c) Biportal removal of a paracentral herniated nucleus pulposus with a flexible pituitary forceps. (d) Probing an additional residual sequestered subligamentous fragment beneath the traversing nerve in this same patient. It is possible to probe the epidural space and the nerves with flexible instruments. (e) Final inspection of a completely decompressed traversing nerve in this same patient.
- Figure 4
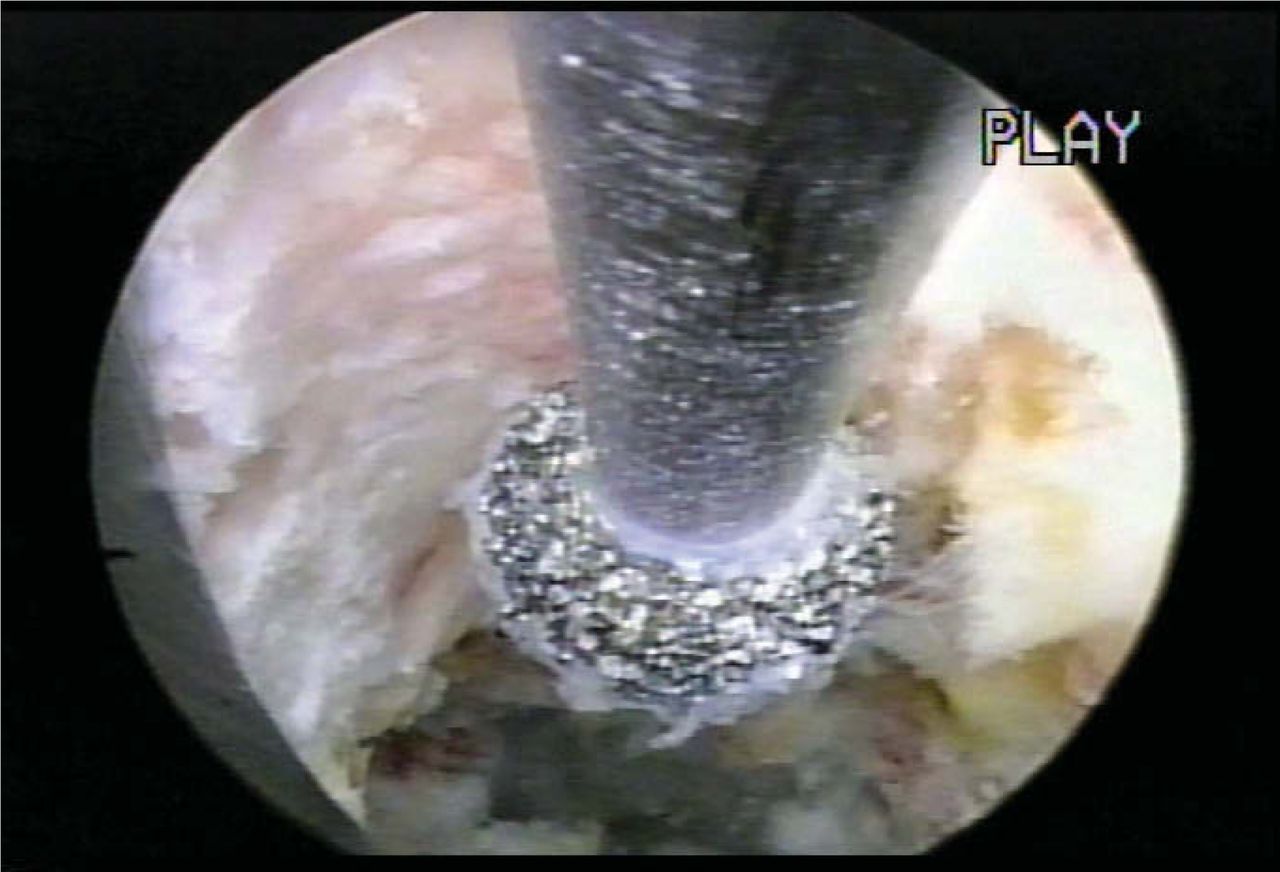
Endoscopic foraminal decompression of the superior facet with a diamond burr.
- Figure 5
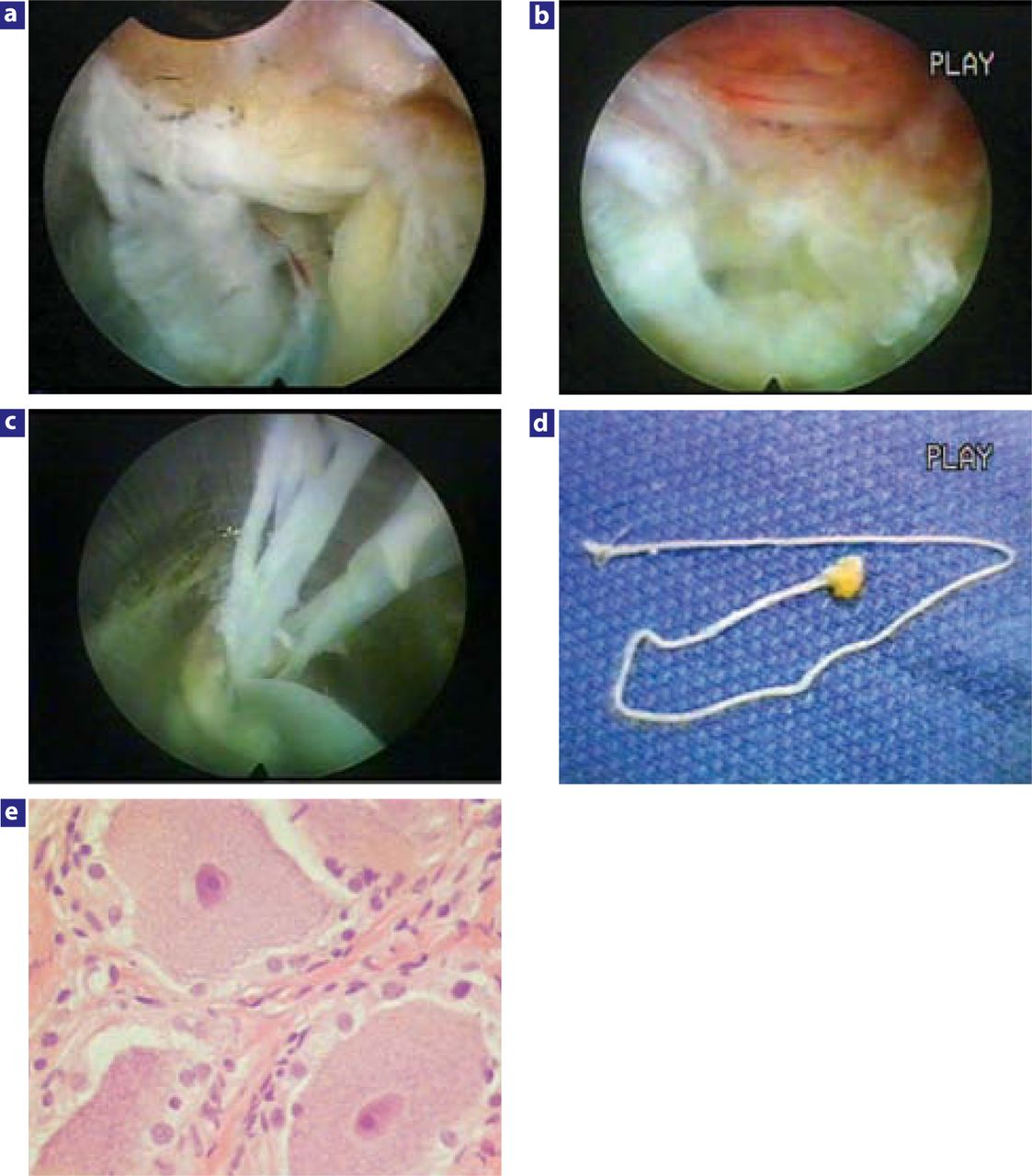
Anomalous nerves in the foramen. (a) Large bifurcation of the right L4 exiting nerve in the foramen at L4–L5. The head is cephalad at 3 o'clock. This size furcal nerve will cause complications of dysesthesia, profound weakness, and numbness if resected or ablated. Ablation or removal of smaller furcal nerves 1 mm or smaller will only produce temporary dysesthesia. Gradual improvement should then occur because the main nerve is still intact. Surgeons must recognize furcal nerves in the foramen and avoid cutting them if more than a millimeter in size, but sometimes it is not possible to get into the disc without affecting these furcal nerve branches. Surgeons who use the transcanal approach for decompression of the subarticular and lateral recess may be removing furcal nerves without realizing it. (b) Anomalous autonomic nerve in foraminal zone. This anomalous autonomic nerve in the foraminal zone is easy to mistake for a furcal nerve. (c) Surgical removal of the nerve shown in Figure 5b during visualized removal of the foraminal herniation. (d) Excisional biopsy of this nerve identified it as an autonomic nerve. Autonomic nerves can be part of an anomalous trunk of nerves that to my knowledge has not been identified in the foramen or mentioned previously in the peer-reviewed literature. This anomalous nerve was extracted inadvertently from the axilla between the exiting and traversing nerve in the patient in Figure 5b during the removal of a foraminal disc herniation. The nerve was lateral to the traversing nerve and away from the dura and could not have been cauda equina. The patient had dysesthesia, but responded to foraminal epidural blocks and sympathetic blocks. Dysesthesia is usually temporary, but residuals are possible. Removal of these small nerves cannot always be avoided and is a known risk of foraminal surgery. (e) Photomicrograph of the nerve shown in Figure 5b. This nerve, thought to be a furcal nerve, contained ganglion cells. The presence of ganglion cells differentiates an autonomic nerve from a myelinated furcal or conjoined nerve.
- Figure 6
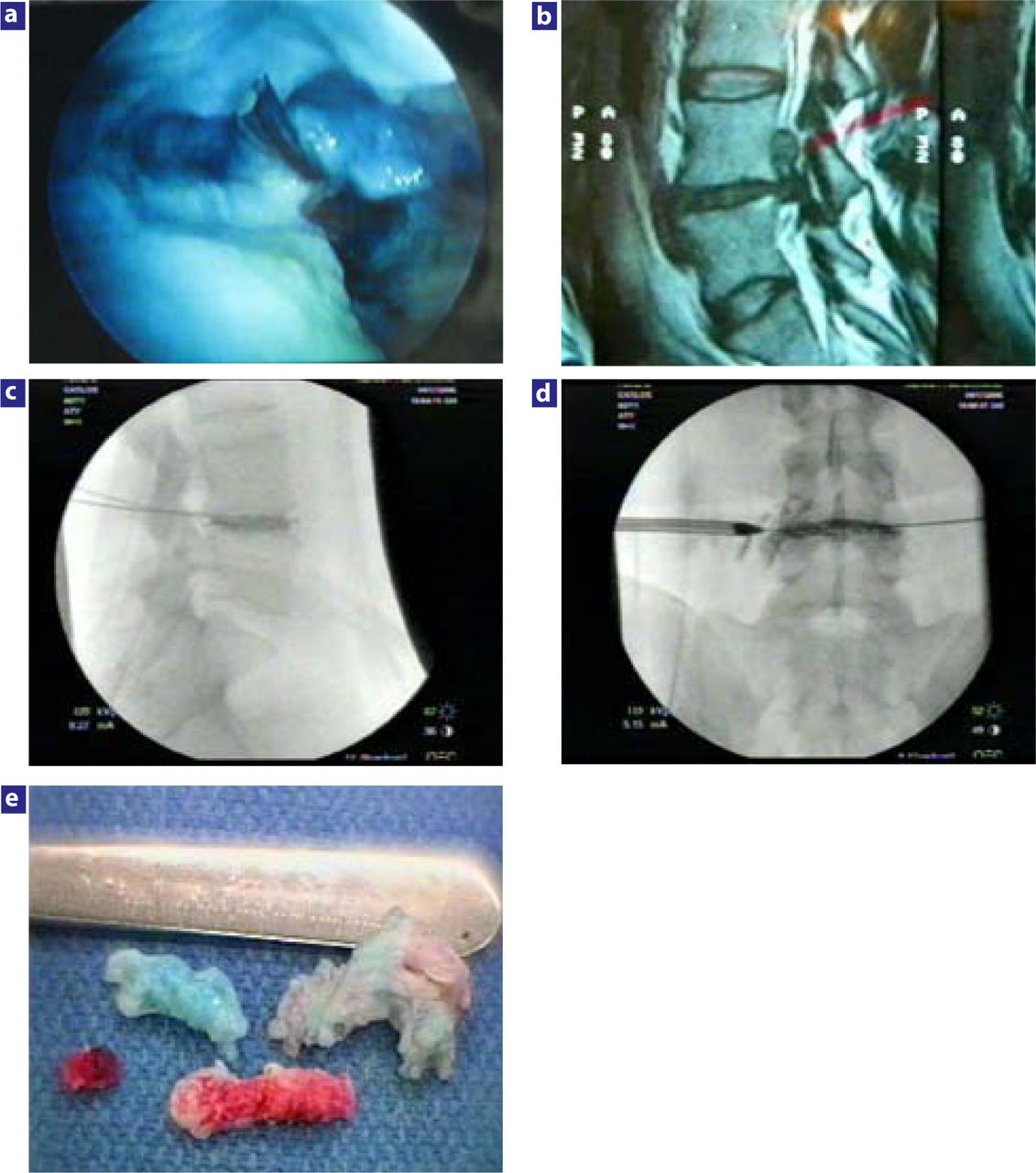
The effect of chymopapain on nucleus pulposus. (a) A biportal technique was used to inject 1000 units of chymopapain into the indigo carmine–stained nucleus pulposus before endoscopic shavers were used to evacuate the partially digested nucleus pulposus. Note the presence of the spinal needle used to inject the chymopapain, and that some of the nucleus is still stained by the indigo carmine dye. The consistency of the nucleus pulposus was made softer and easier for the shaver to evacuate the nucleus, leaving the cavity shown. To perform a thorough nuclectomy, however, the surgeon must also include manual discectomy with pituitary forceps. In selective endoscopic discectomy, the goal is to remove as much of the loose fragments that are stained blue as feasible. More-normal disc tissue will resist staining. The use of chymopapain to help with nuclectomy may play an important role in some nucleus replacement implants, because residual normal noncollagenized nuclear material may be more difficult to remove mechanically with traditional tools. If used in conjunction with mechanical discectomy, the chymopapain-treated nucleus is slippery, aiding its manual extraction, especially if the fragment is also bathed by chymopapain that has leaked out of the annular defect. (b) This extruded sequestered disc herniation is aided by the injection of chymopapain into the disc before manual extraction. When chromodiscography follows, the discogram pattern helps the surgeon target the disc fragment(s) to be removed. The chymopapain treated is softer and more slippery, making it easier to remove from the epidural space. (c, d) Chromodiscography demonstrates that the dye and extruded fragment are likely extruded and can be found in the axilla between the traversing and exiting nerve, making removal of the extruded fragment(s) probable. In the lateral view there is a void in the discogram pattern suggestive of a collagenous fragment and the lateral view demonstrates leakage of dye to the exiting nerve. The combined pattern suggests fragments in the axilla and epidural space. This is confirmed by the fragments removed. (e) Fragments visualized and extracted from the foramen with the endoscope. Note the differential staining, including the inflamed fragment(s) from the epidural space. The blue-stained fragment was found mostly inside the disc, whereas the partially stained fragment was partially trapped in the annular defect and the unstained inflamed fragment was loose in the epidural space. Chymopapain, when used as an adjunctive procedure, helps the surgeon with mechanical extraction and will help digest any small extruded fragment inadvertently left behind.
- Figure 7
Thermal annuloplasty sealing an annular tear with a bipolar high frequency flexible probe. (a) Annular tear visualized with a 20-degree spine endoscope. Note bleeding coming from the tear in the posterior annulus paracentrally after extraction of nuclear material that was keeping the tear open. (b) Bipolar flexible radiofrequency probe thermally shrinking the annular tear under direct vision. A biportal approach is utilized here. (c) Sealed annular tear. Clinical result was excellent. At 1-year follow-up, the patient still had complete resolution of sciatica and back pain. Single quadrant tears respond very well with thermal annuloplasty, whereas 360° tears in a degenerated, narrowed disc may still get relief, but back pain may eventually increase.




Tables
Assessment Definition Excellent No pain, no functional restrictions Good Occasional back/leg pain, brief or slight functional restriction Fair Improved overall function, permanent work and activities of daily living restrictions Poor No improvement in pain/functional level or reoperation at index level
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.