


Abstract
Background A retrospective study of patients treated by transforaminal lumbar interbody fusion (TLIF) with local bone graft alone for single-level isthmic spondylolisthesis (IS) between April 2009 and July 2014 in a single facility.
Methods Demographic and operative data, complications, preoperative and postoperative clinical records, and radiographs were revised. The Visual Analogue Scale (VAS) and Denis Work Scale were used for clinical and functional assessment. Modified Lee et al. classification was used for assessment of union.
Results Twenty-three patients with mean age of 45.04 ± 7.19 years had single-level TLIF with local bone graft alone for symptomatic IS with mean follow-up period of 28.39 ± 4.01 months and mean operative time of 170.09 ± 11.22 minutes. The VAS and Denis Work Scale improved from 8.48 ± 0.58 and 4.67 ± 0.47 preoperative to 2.91 ± 1.25 and 1.33 ± 0.58 at the latest follow up, respectively. Anterior vertebral translation improved from 27.22 ± 9.54% preoperatively to 8.38 ± 3.63% postoperatively and 10.39 ± 3.49 at the latest follow up. Disc space height was 9.67 ± 5.55% preoperatively, 21.60 ± 4.11% postoperative, and 16.24 ± 4.02% at the latest follow up. Lumbar lordosis improved from 29.39 ± 10.33° to 45.13 ± 6.84° postoperatively and 39.96 ± 7.52° at the latest follow up. Eighteen patients had definitive union, 4 patients with possible union, 1 patient with possible pseudoarthrosis.
Conclusions Transforaminal lumbar interbody fusion with local bone graft alone is an appropriate option for single-level IS, yet we do not recommend it for higher grades of slippage with anterior vertebral translation more than 25%.
INTRODUCTION
Various surgical techniques have been advocated to deal with symptomatic isthmic spondylolisthesis (IS) in adults. However, selection of the optimal approach and fusion technique is a matter of debate.1,2 Interbody fusion techniques have been developed to provide solid fixation of spinal segments while maintaining load bearing capacity and proper disc space height.3 The ability to reconstruct the anterior column after disc removal is important because 80% of the compressive, torsion, and shear forces are transmitted through the anterior column3; however, the choice between different techniques using interbody cages or bone grafts and whether the graft is autogenic or allogenic is also a wide area of controversy.4–6 Although there are several studies reporting the transforaminal lumbar interbody fusion (TLIF) technique,7,8 these studies were confusing; that is, several diseases such as degenerative spondylolisthesis, IS, lumbar canal stenosis, and disc herniation were mixed. The current study is focusing on patients with adult IS only and presenting the long-term clinical and radiologic results of TLIF with local bone graft alone for single-level IS.
PATIENTS AND METHODS
This is a retrospective cohort, institutional review board-approved study. All patients who underwent a single-level instrumented TLIF procedure wherein only local bone pieces collected from laminectomy were used for spinal fusion between April 2009 and July 2014 at our hospital were included. Patients considered for surgical treatment had persistent symptoms of low back pain with neurological manifestations in the form of sciatica or neurological intermittent claudication refractory to conservative treatment for at least 3 months. Exclusion criteria included multilevel IS, traumatic spondylolisthesis, tumors, infection, previous lumbar spine surgery, and patients with incomplete follow up. Data reported included demographic information, operative time, complications, as well as preoperative and postoperative clinical records and radiographs. The clinical results were evaluated according to the back pain Visual Analogue Scale (VAS; 0 as no pain to 10 as maximal pain)9 and Denis Work Scale.10
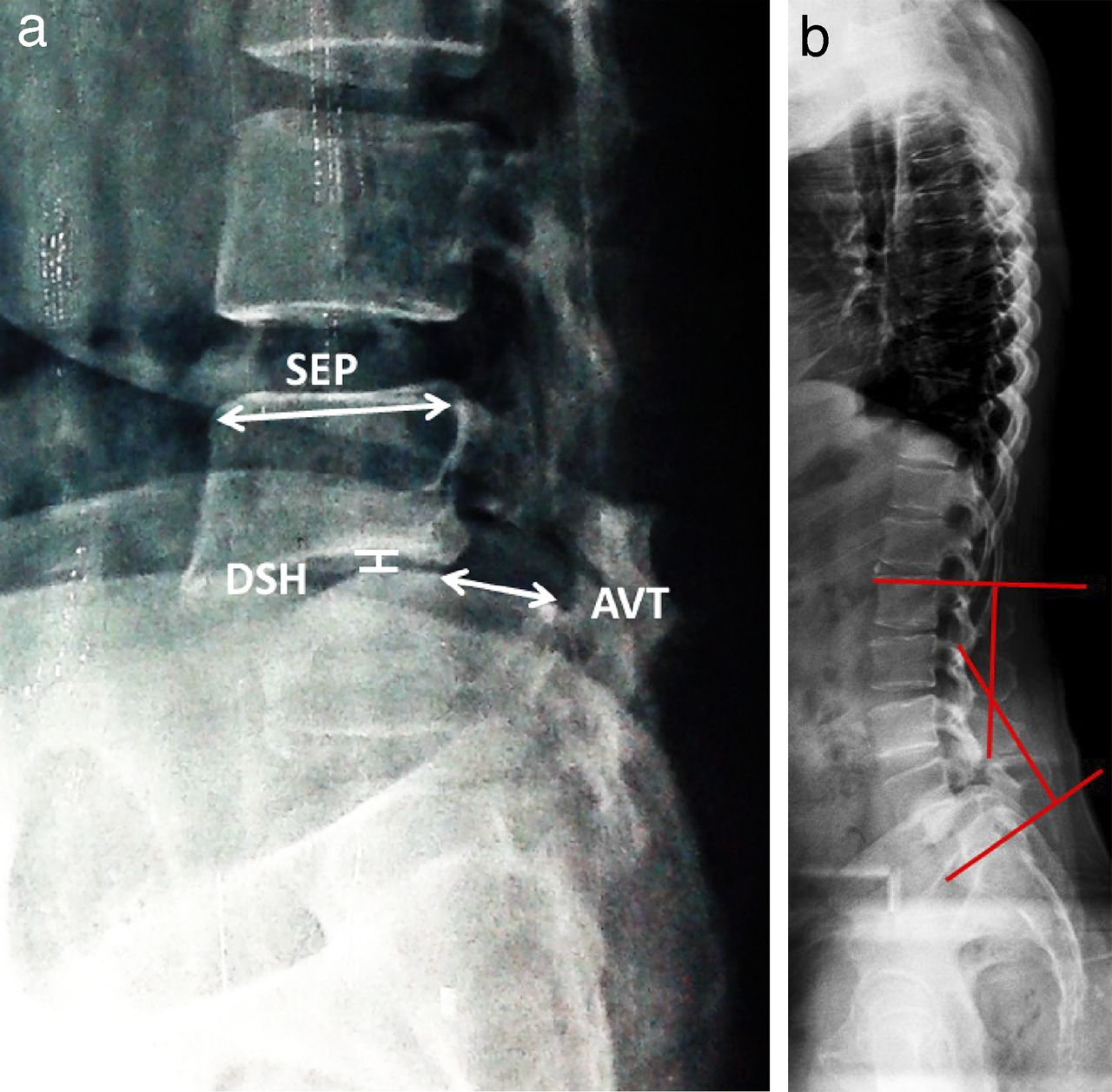
All subjects had radiographic spinal evaluation preoperatively, postoperatively, and at latest follow up with each subject in a comfortable standing position and the knees fully extended with 36-inch lateral, flexion, and extension views. Anterior vertebral translation and the disc space height were presented as percentages of the anteroposterior diameter of the superior end plate of the slipped vertebra to avoid the magnification errors (Figure 1a). Furthermore, the well-known Meyerding classification lacks accuracy in the case of IS, since hypoplasia of the spondylolytic vertebrae is not taken into consideration.11 Lumbar lordosis was measured from the superior end plate of L1 to the superior end plate of S1 (Figure 1b). Modified Lee et al.12 classification was used for assessment of union; the classification depends on the presence or absence of bridging bony trabeculae or gap at the graft host interface and movement (≥3°) on dynamic x-ray (Table 1). Each image was blinded and evaluated by 2 spine surgeons.

(a) Radiographic measurement of anterior vertebral translation (AVT) and disc space height (DSH). Both are expressed as a percentage of the superior endplate diameter (SED) of the slipped vertebra. (b) Measurement of lumbar lordosis.
Modified Lee et al.12 classification.
Surgical Technique
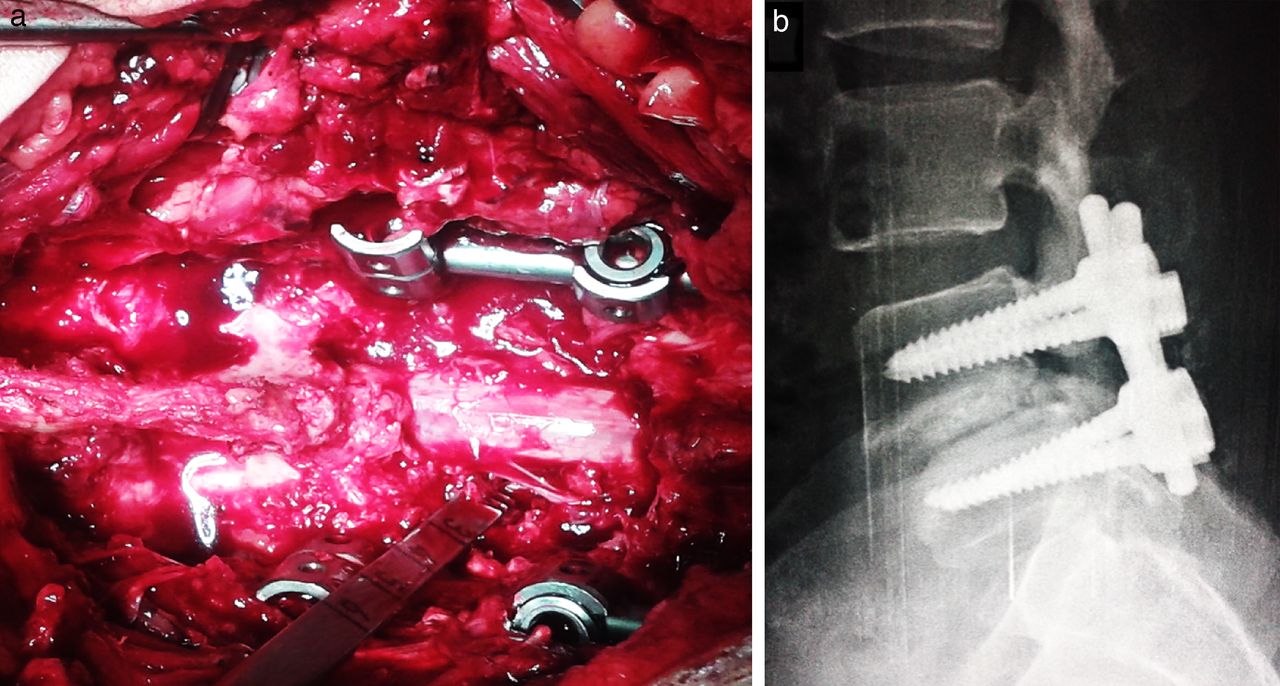
Under general anesthesia in prone position with both hips extended, the posterior elements of the spine are exposed to the bases of the transverse processes. Two reduction screws in the slipped vertebra and 2 monoaxial pedicle screws in the distal vertebra were inserted under fluoroscopic control, followed by complete laminectomy and decompression of the nerve roots bilaterally. The disc space is exposed transforaminal lateral to the nerve root; disc space height restoration was done by gradual distraction on the contralateral screws. Complete discectomy with preparation of the end plates was performed using curettes, rongeurs, and rasps (Figure 2a). Morsellized bone chips obtained from laminectomy and facetectomy were packed in the disc space followed by final tightening of the screws (Figure 2b). Drains were removed when blood collection was <50 mL per 24 hour. Bending, sitting, squatting, and lifting light weights were allowed at 3 months. Brace support was recommended for 6 weeks after surgery.
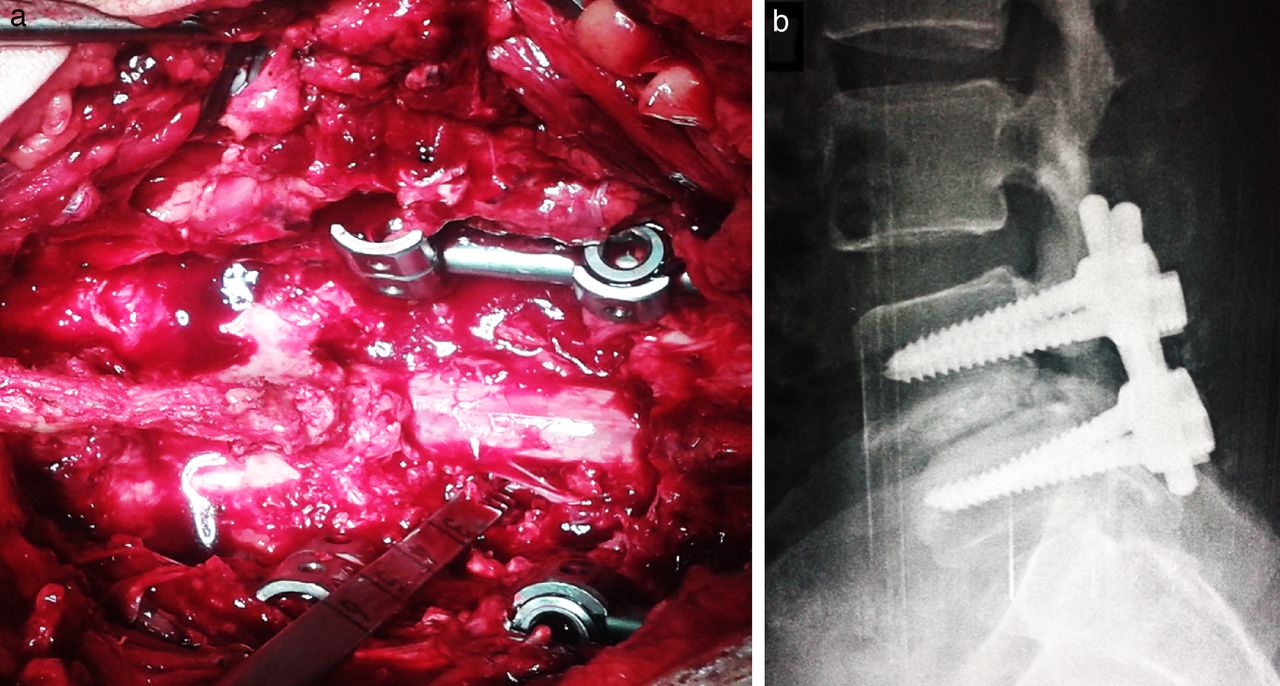
(a) Complete discectomy and end plate preparation. (b) Postoperative x-ray.
Statistics
Data were statistically analyzed using SPSS software (SPSS, Chicago, Illinois). The measurements were expressed as means ± SD. Paired sample t test was used for statistical comparisons. P value < .05 was considered statistically significant.
RESULTS
Twenty-three patients (11 males and 12 females) fulfilling the inclusion criteria were enrolled in this study. Mean age was 45.04 ± 7.19 years. Fusion level was L4-L5 in 9 patients (39%) and L5-S1 in 14 (61%) with mean follow-up period of 28.39 ± 4.01 months. The mean operative time was 170.09 ± 11.22 minutes.
The back pain VAS significantly improved from 8.48 ± 0.58 preoperatively to 2.91 ± 1.25 at the latest follow up (P = .047). The functional outcome according to the Denis Work Scale improved from 4.67 ± 0.47 to 1.33 ± 0.58; 5 patients who were not engaged in a specific job before surgery were excluded (Table 2).
Patient characteristics, operative, clinical and radiological data.
The anterior vertebral translation significantly improved from 27.22 ± 9.54% preoperatively to 8.38 ± 3.63% postoperative (P = .039) and 10.39 ± 3.49 at the latest follow up. Disc space height was 9.67 ± 5.55% preoperatively, 21.60 ± 4.11% postoperatively (P = .022), and 16.24 ± 4.02% at the latest follow up. Lumbar lordosis improved from 29.39 ± 10.33° to 45.13 ± 6.84° postoperatively (P = .036) and 39.96 ± 7.52° at the latest follow up (Table 3). The loss of correction at the latest follow up was significant in the 3 radiological parameters (P < .001; Table 3).
Comparison of radiological parameters.
According to modified Lee et al.12 classification, there were 18 patients with definitive union, 4 patients with possible union, 1 patient with possible pseudoarthrosis, and no patient with definitive pseudoarthrosis. There was no patient with the pedicle screw loosening and implant failure. There were 3 cases (13%) of dural tear which were primarily sutured and the wound closed water tight with no postoperative manifestations of meningitis or cerebrospinal fluid leakage, 2 cases (8.6%) of superficial wound infection which were managed successfully with parenteral antibiotics, and 2 cases of pedicle screw misplacement were detected postoperative; however, none of the cases had neurological deficit or reoperation.
DISCUSSION
It is well established that the goals of surgical treatment of spondylolisthesis are fusion of as few motion segments as possible, reduce the forward translation of the slipped vertebra, decompress the neural elements, and restore the disc space height and sagittal balance of lumbar spine.3
Posterior lumbar interbody fusion (PLIF) has been associated with higher incidence of neurological complications, up to 13.6% permanent neurologic lesions, increased intraoperative blood loss, postoperative epidural fibrosis, and arachnopathy.13 Moreover, PLIF is limited to fusions of L3-S1 to avoid the risk of nerve damage during retraction.14 The TLIF approach runs through the far lateral portion of the vertebral foramen to access the disc space, providing a safe corridor for fusion procedure that may reduce many of the risks and limitations associated with PLIF.14,15
For the fusion technique, different cages were used for interbody fusion to restore disc space height; however, the implantation of cages decreases the contact area for bony fusion which should be more than 30%.16 Moreover, the visualization and assessment of spinal fusion status becomes difficult in the presence of interbody cages.17 The differing modulus of elasticity of cages and bone may precipitate cage sinking in the vertebral end plate, especially in osteoporotic bone.18 Last but not least, the high cost of cages cannot be neglected.
Autologous iliac bone graft has been considered the gold standard to achieve solid bone fusion, yet donor site complications are high including hematoma formation, infection, sensory deficit, reoperation, and chronic pain.6 Allograft and artificial bones have less ability for bone healing. and allograft may also have a risk for blood borne disease transmission.5,19 Many of these complications and disadvantages can be circumvented by the use of local bone chips obtained from the laminectomy.20,21
In the current series, the TLIF procedure with local bone graft alone improved anterior vertebral translation, disc height, and lumbar lordosis. A proper surgical technique with adequate discectomy and facetectomy would contribute greatly to the improvement of the radiological parameters; however, this improvement was not maintained at the latest follow up (Table 3). This can be explained by the fact that corticocancellous bone chips do not provide immediate mechanical support; however, in the presence of pedicle screws, the fixation becomes a fairly rigid construct adequate for spinal fusion to occur. This fact is supported in our series, where we had neither definite pseudoarthrosis nor implant failures. Both clinical and radiologic outcomes are considered to be satisfactory with low complication rate, although it was not compared with a control group. Given these considerations, it would seem that the use of TLIF with local bone graft alone is a good option for single-level IS; however, care should be taken in managing cases with high mechanical demands such as high grade listhesis, as these cases need efficient anterior column support beside the biological properties of the local bone graft for fusion.
CONCLUSION
Transforaminal lumbar interbody fusion with local bone graft alone is a good option for single-level IS, with low complication rate and favorable clinical and radiological results. However, we do not recommend this technique for high-grade listhesis with anterior vertebral translation more than 25%. Further prospective comparative studies with bigger cohort and longer follow up are needed.
Footnotes
Disclosures and COI: Institution review board approval was obtained. No conflict of interest.
- ©International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}