


Article Figures & Data
Figures
- Figure 1
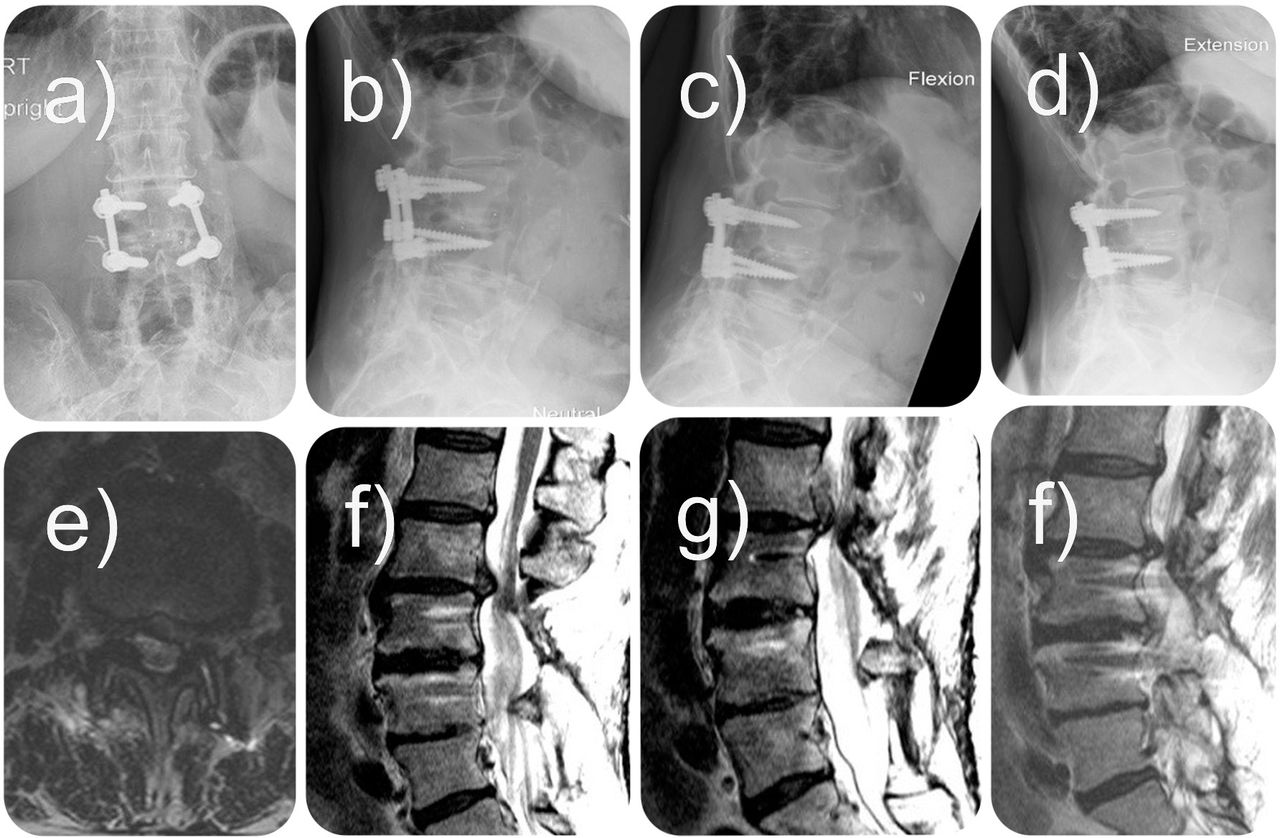
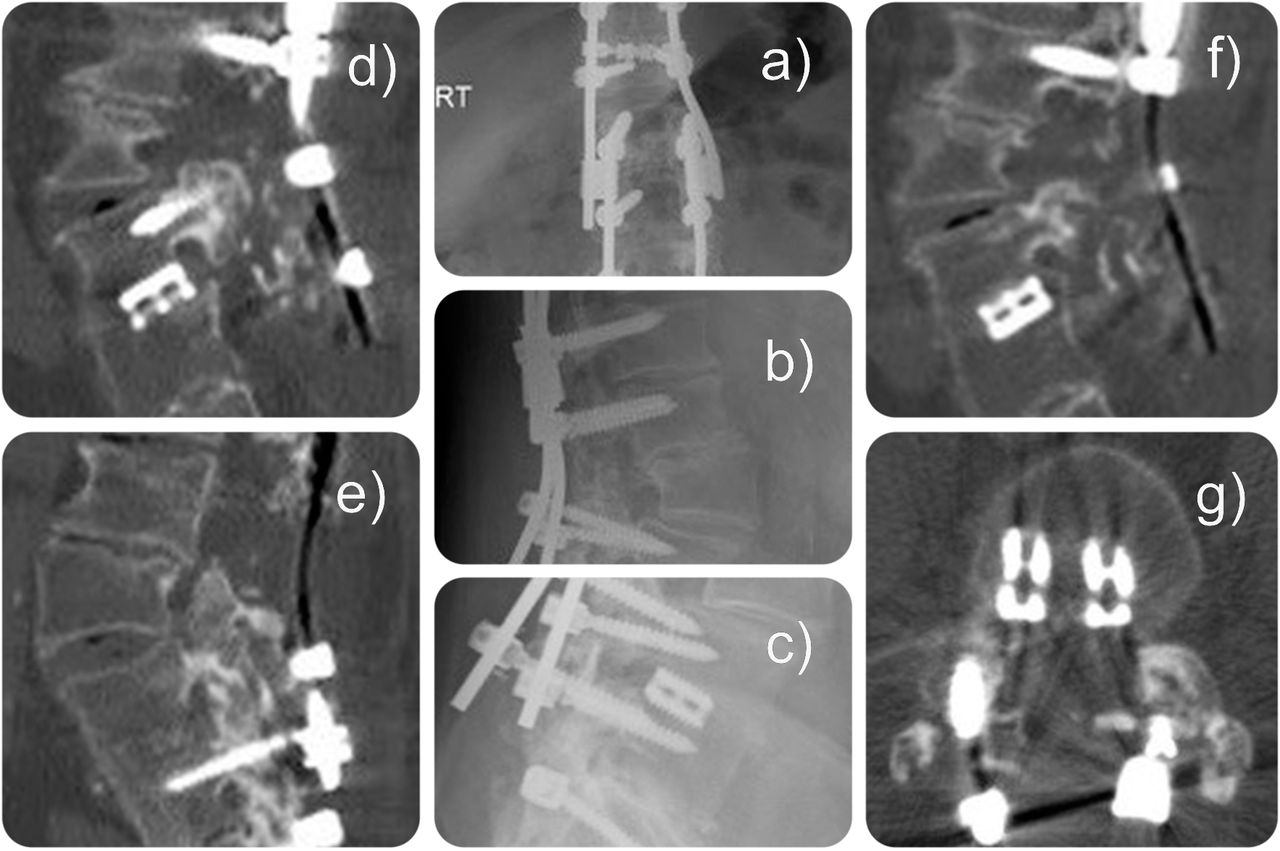
Plain film studies (a–d) and magnetic resonance imaging scans (e–h) of a 76-year-old female patient who underwent previous laminectomy followed by transforaminal interbody fusion (TLIF) at L3-4 years after her previous laminectomy. She presented with new onset of left-side inner thigh pain and neurogenic claudication symptoms 3 years following her TLIF. This patient was not interested in more open spinal surgery of any sort but opted for outpatient transforaminal decompression at L2-3 on the left side to treat the symptoms stemming from the adjacent segment disc herniation and resulting lateral recess stenosis surgically. She went home within an hour from surgery and her symptoms completely resolved immediately postoperatively. Her final follow-up visit was 30 months after secondary endoscopic outpatient decompression; she remained pain free.
- Figure 2
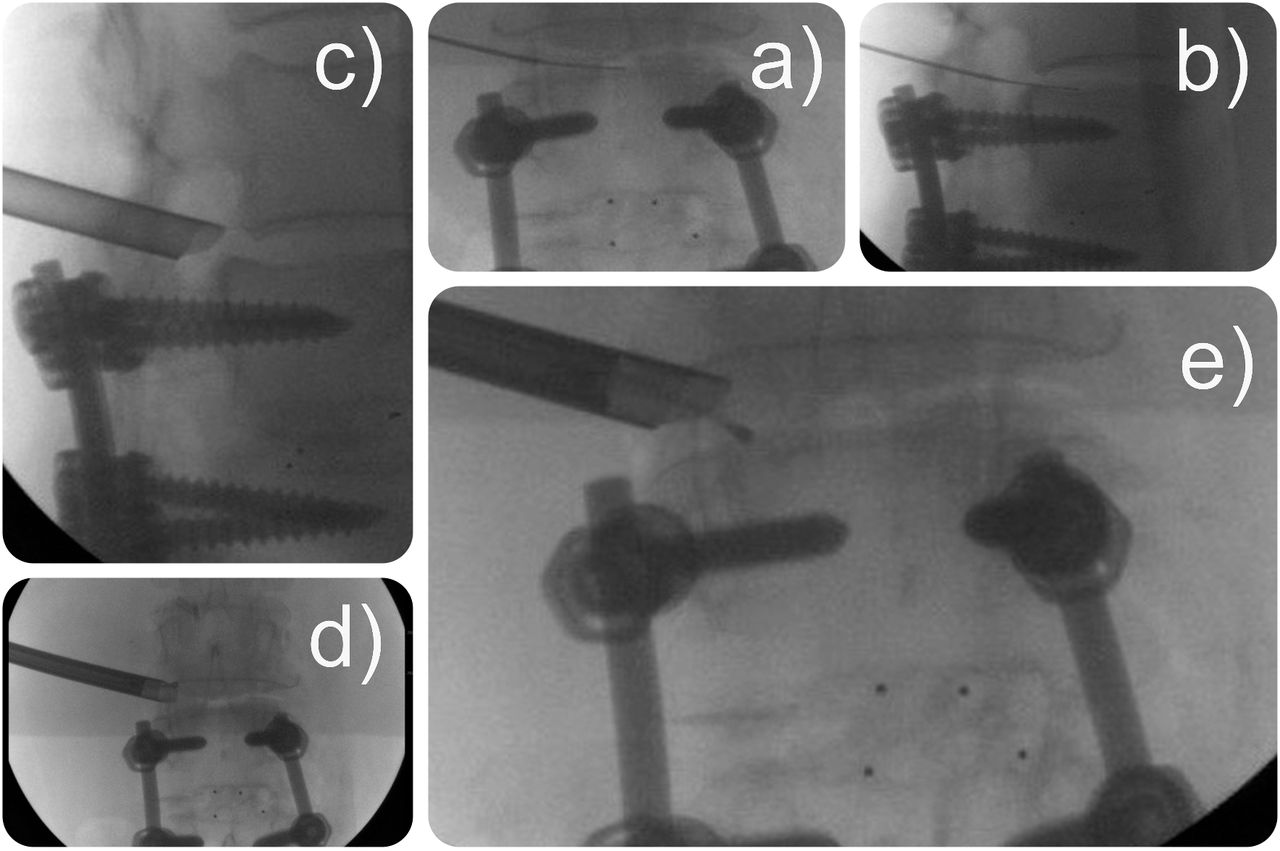
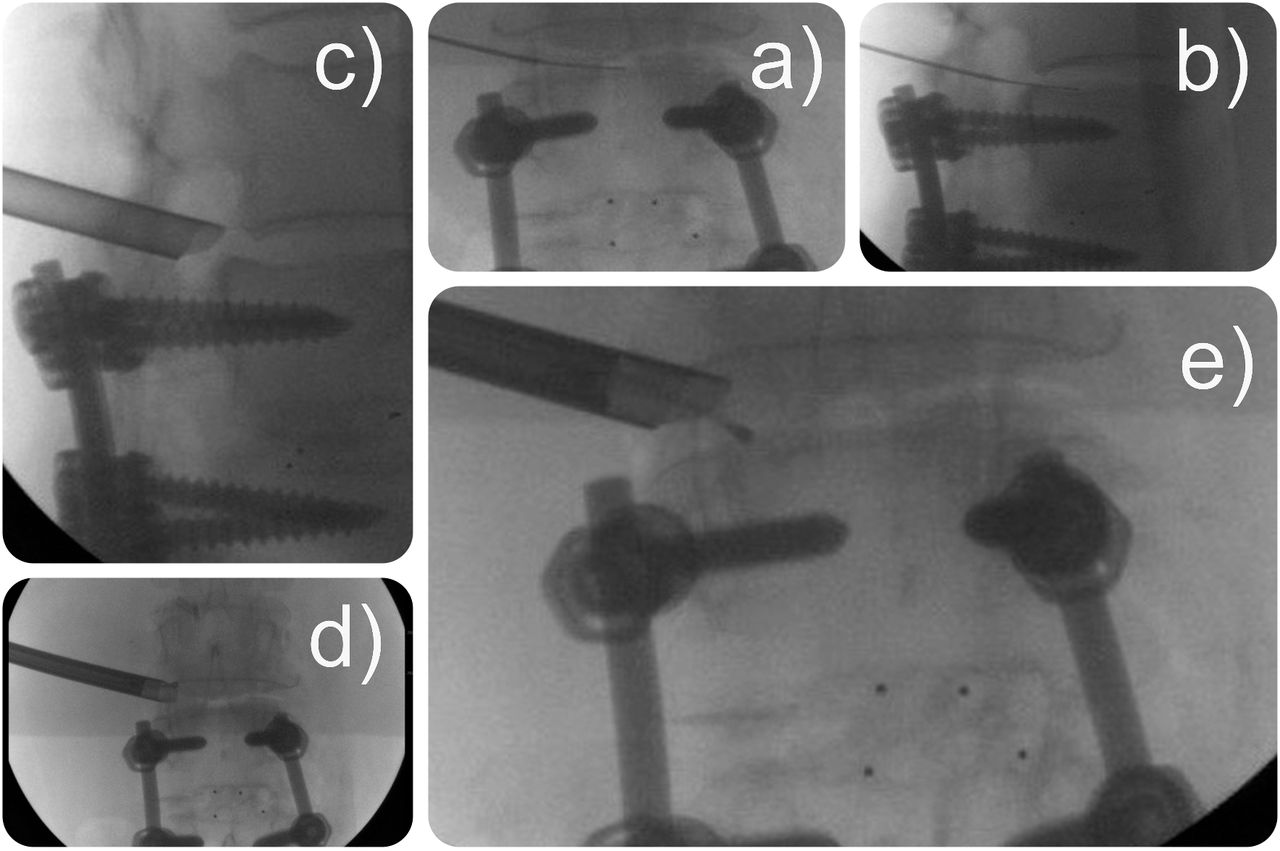
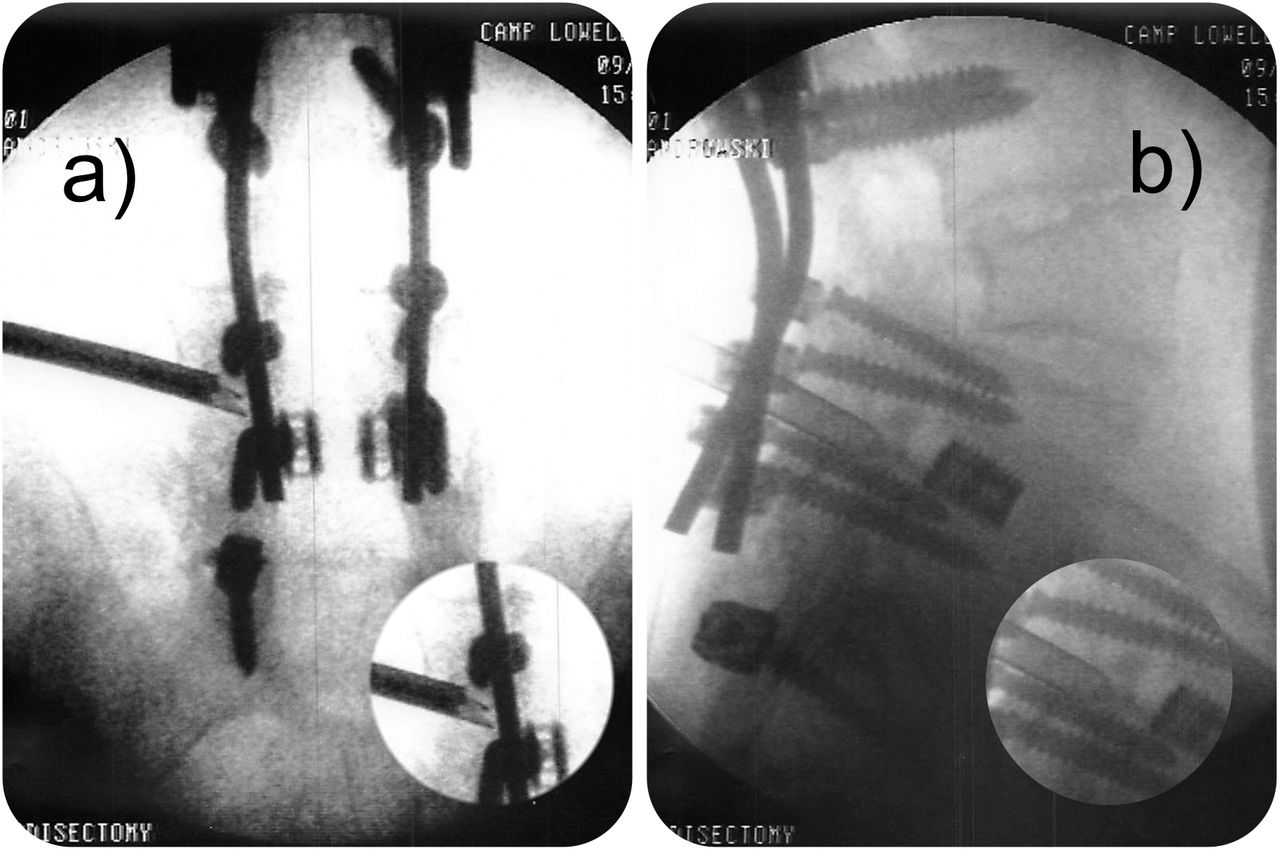
Intraoperative fluoroscopy images of a 76-year-old female patient who underwent previous laminectomy followed by transforaminal interbody fusion at L3-4 years after her previous laminectomy. (a and b) Placement of an 18-G, 8-inch guide wire. (c and d) Placement of the working cannula. (e) Placement of the flexible palpation probe into the lateral recess to check for free fragments and to assess the decompression.
- Figure 3
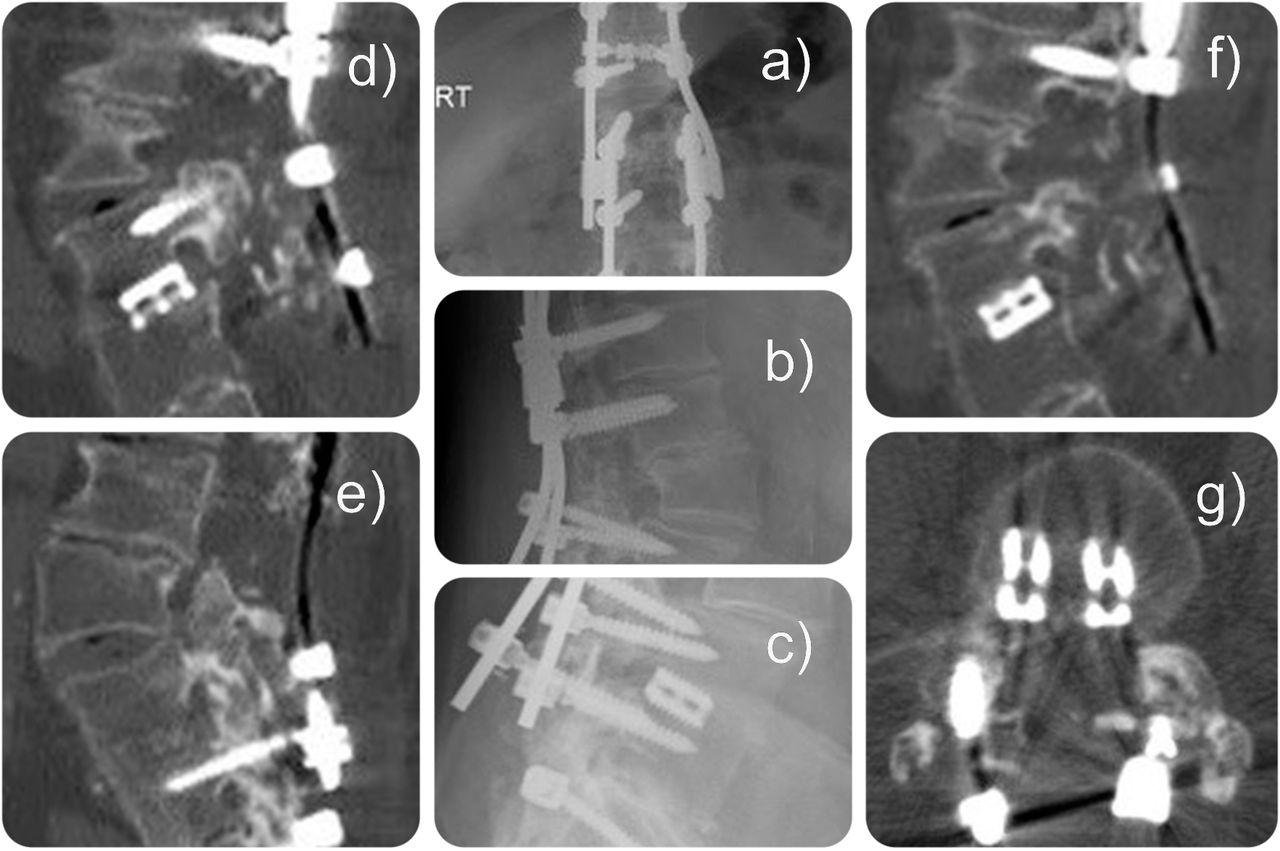
Plain film studies (a–c) and computed tomography scans (d–g) of a 69-year-old male patient. Patient underwent multiple previous lumbar surgeries and last pedicle subtraction osteotomy with residual foraminal and lateral recess stenosis at L4-5 with a slightly posteriorly translocated interbody fusion cage (shaded area in e–g), with some bone formation posteriorly to the cage (shown in f). Patient presented with persistent anterolateral thigh and calf pain and neurogenic claudication symptoms and failed interventional and supportive care. An outpatient transforaminal decompression at L4-5 on the symptomatic left side was performed in this complex situation, where postoperative complications because of an open revision surgery would have been likely. This patient went home within an hour from the outpatient surgery center and reported complete resolution of symptoms at 25 months postoperatively.
- Figure 4
Intraoperative fluoroscopy films (a and b) of a 69-year-old male patient. Patient underwent multiple previous lumbar surgeries and last pedicle subtraction osteotomy with residual foraminal and lateral recess stenosis at L4-5 and with a slightly posteriorly translocated interbody fusion cage. His symptoms of persistent anterolateral thigh and calf pain and neurogenic claudication were treated with an outpatient transforaminal decompression at L4-5. (a) The working cannula is placed under the fusion rod and in between pedicle screws. (b) Access to the lateral recess.
- Figure 5
The foraminal drill (a) and chisel (b) shown can be advanced directly to the inner working channel. The drill is attached to a power driver and can be used in forward and reverse directions. It is most suitable for expansile foraminoplasty around the inferior pedicle.
- Figure 6
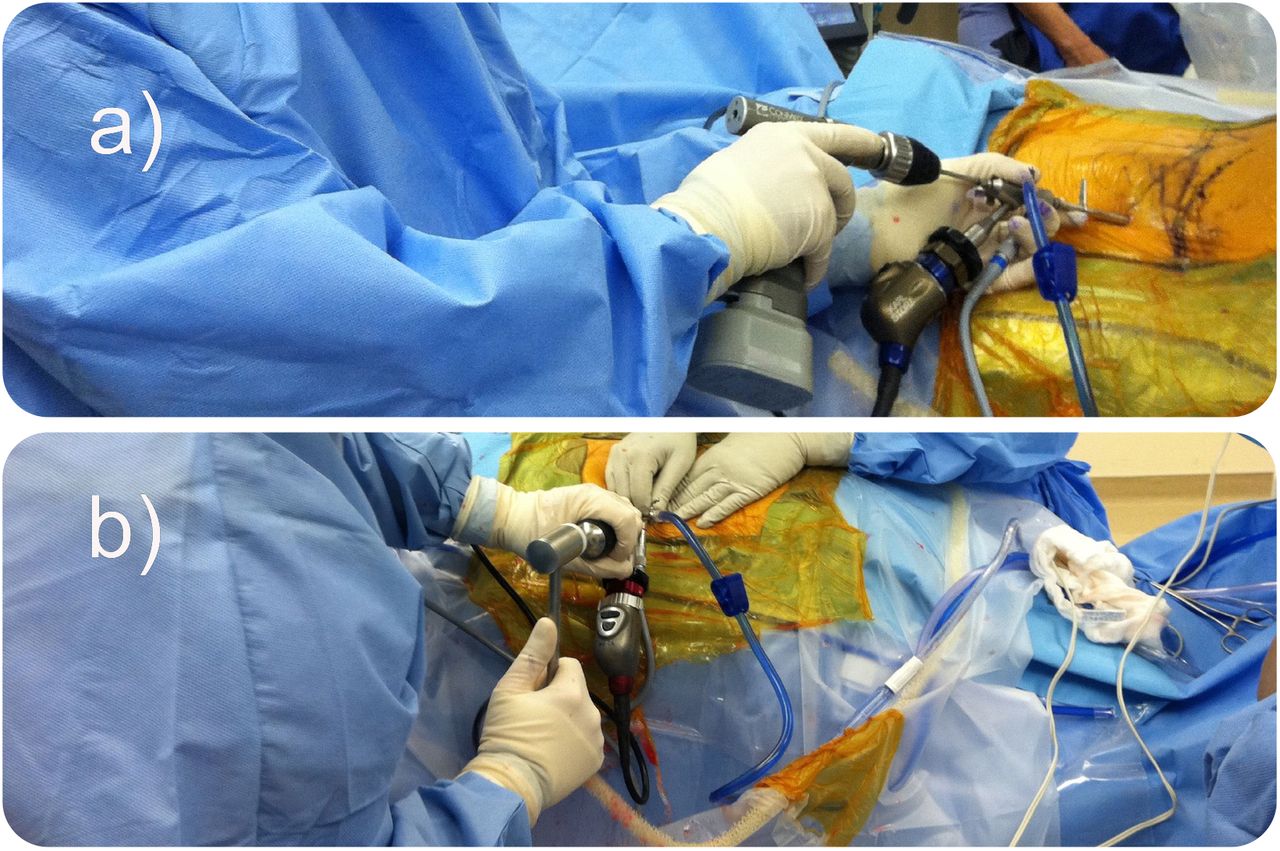
Lumbar endoscopic transforaminal decompression surgery here is shown with an endoscopic Kerrison rongeur (a) and power drill (b) that is advanced through the central working channel of the endoscope.
- Figure 7
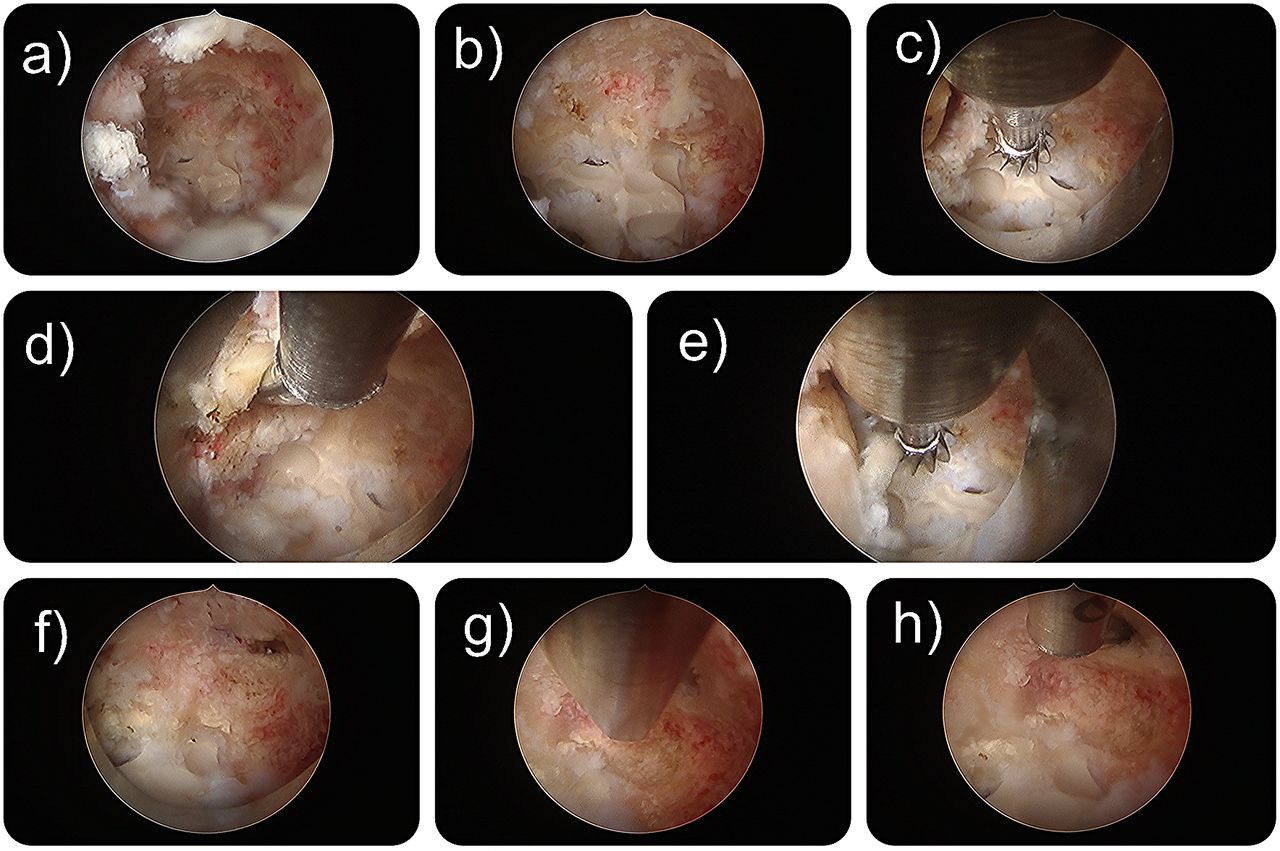
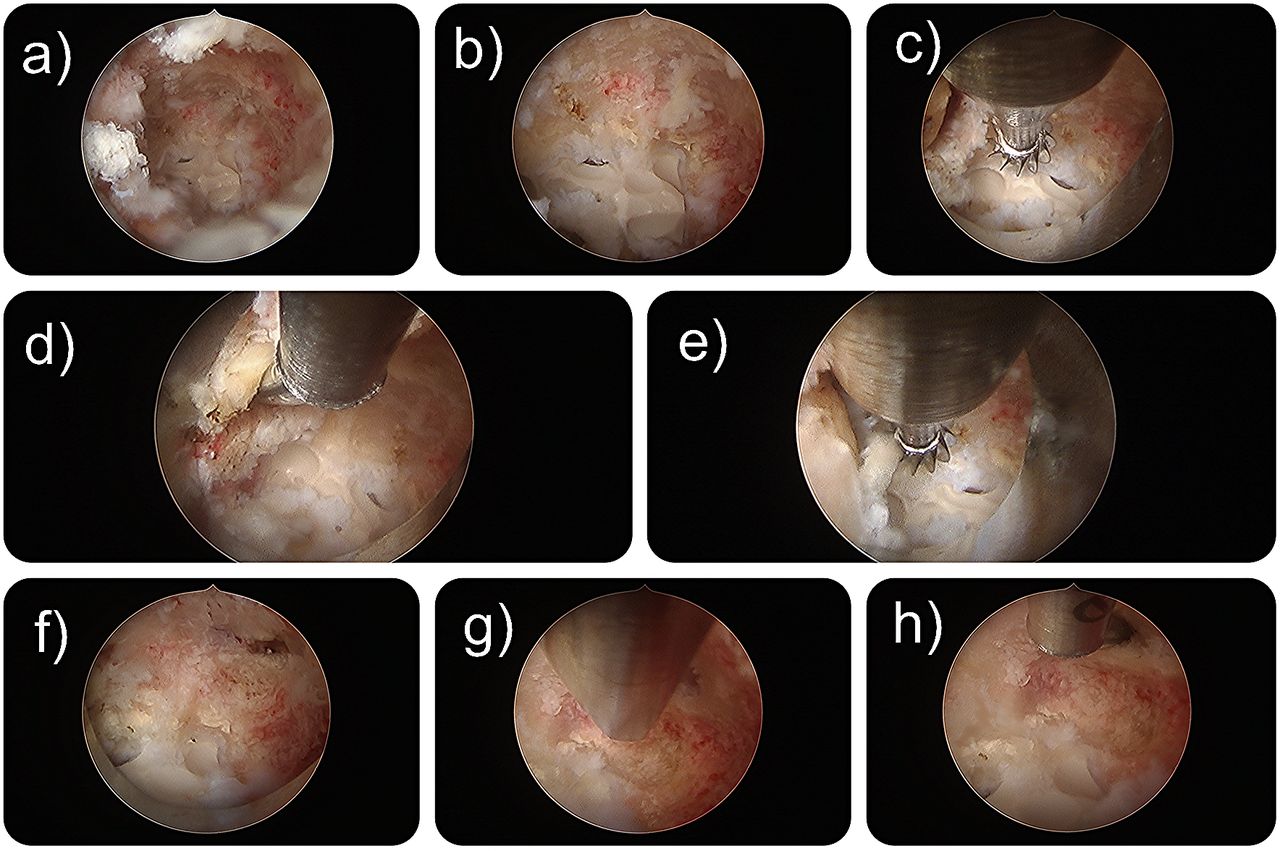
Video-endoscopic photos taken during the transforaminal out-side in endoscopic foraminal and lateral recess decompression in a 76-year-old male patient with multiple previous fusion surgeries. Patient developed heterotopic bone formation behind the interbody fusion cage that was filled with rh-BMP-2 during his index surgery. (a and b) Creation of an access channel through the posterolateral fusion mass that was also grafted with rh-BMP-2. (c) The PEEK interbody fusion cage is exposed. The lateral recess is accessed in the axilla between the exiting and traversing nerve roots with a probe to confirm decompression. (e) The exiting nerve root is completely decompressed. (f–h) The lateral recess is decompressed and probed.
- Figure 8
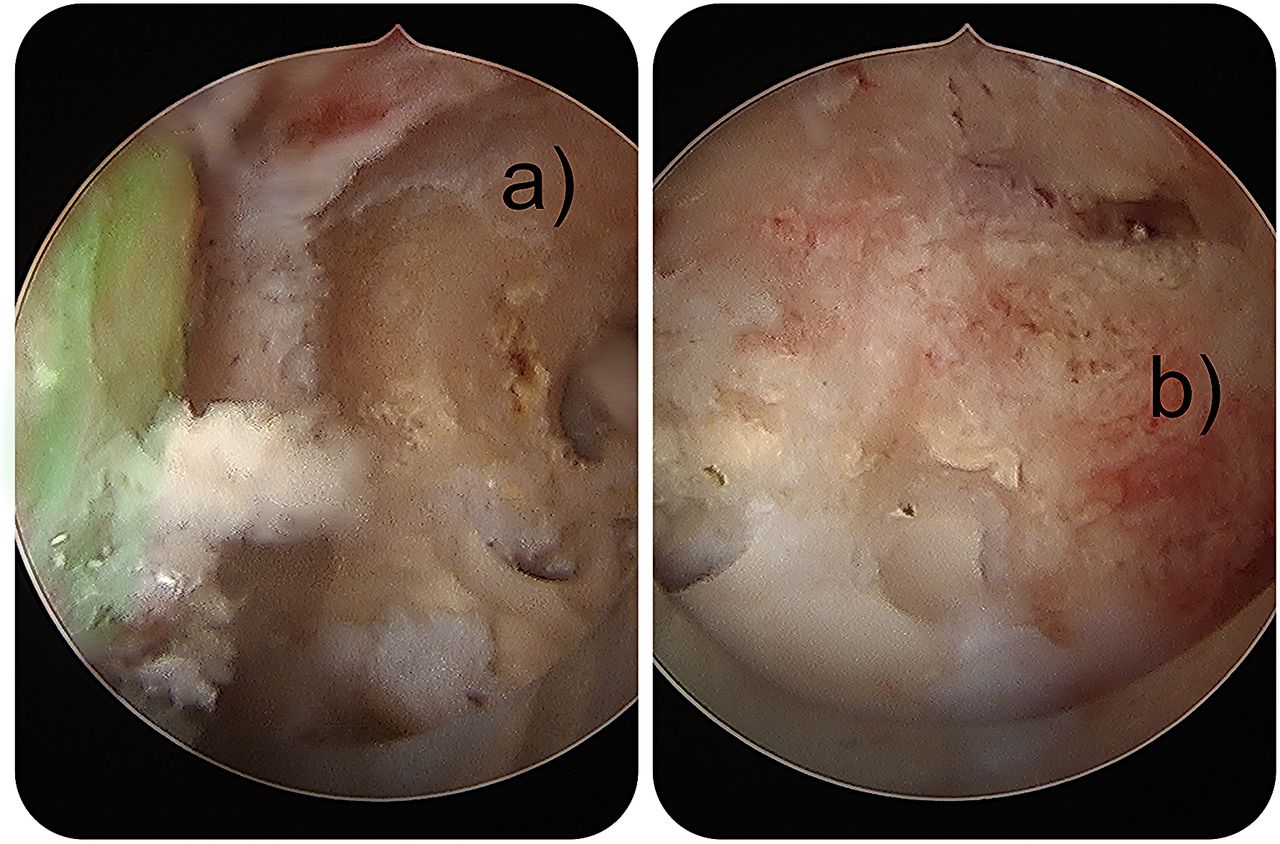
Video-endoscopic photos taken during the transforaminal out-side in endoscopic foraminal and lateral recess decompression in a 76-year-old male patient with multiple previous fusion surgeries. Patient developed heterotopic bone formation behind the interbody fusion cage that was filled with rh-BMP-2 during his index surgery. (a and b) Decompression of the exiting (shaded in green in a) and the traversing (b) nerve root.
- Figure 9
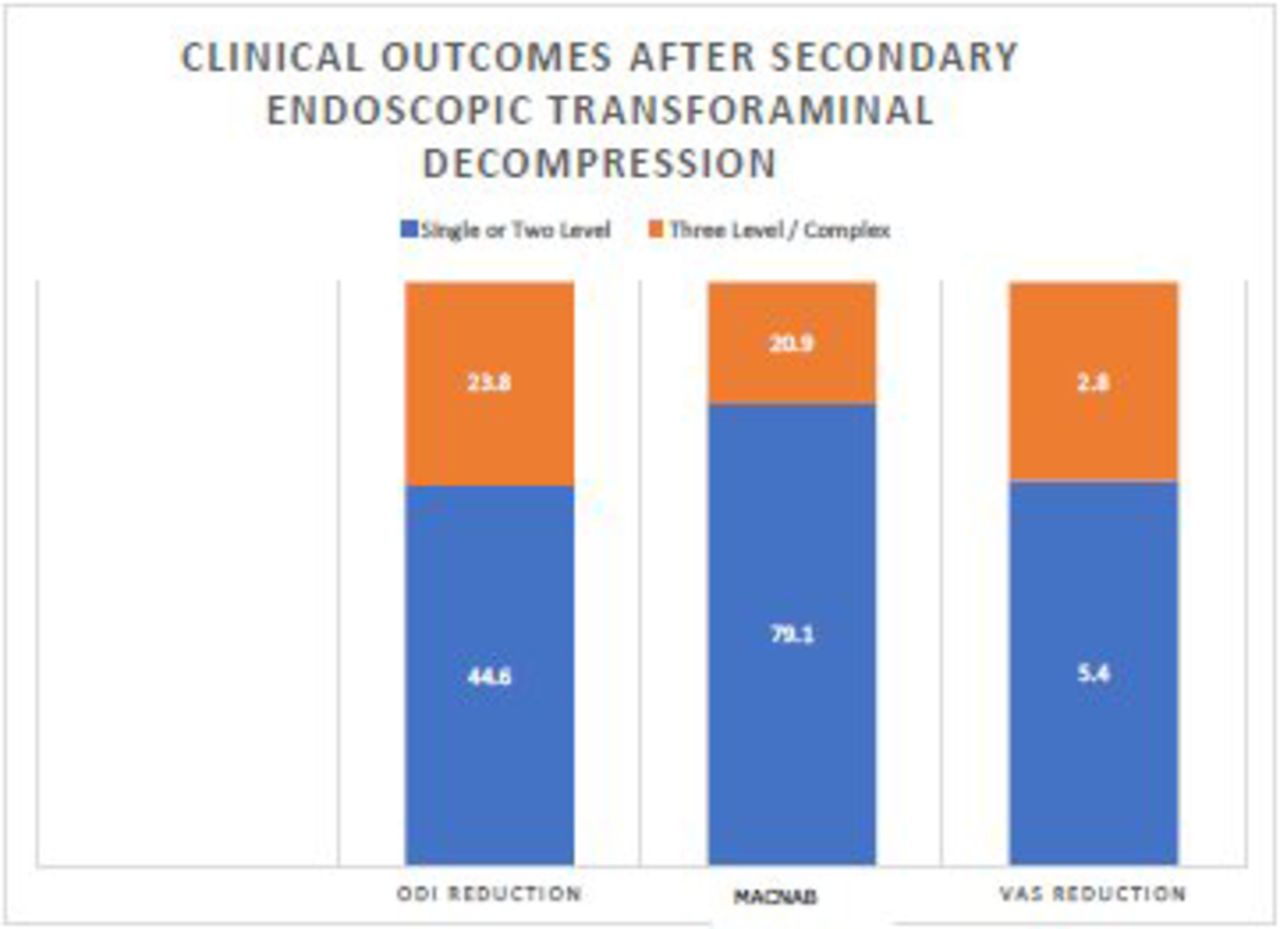
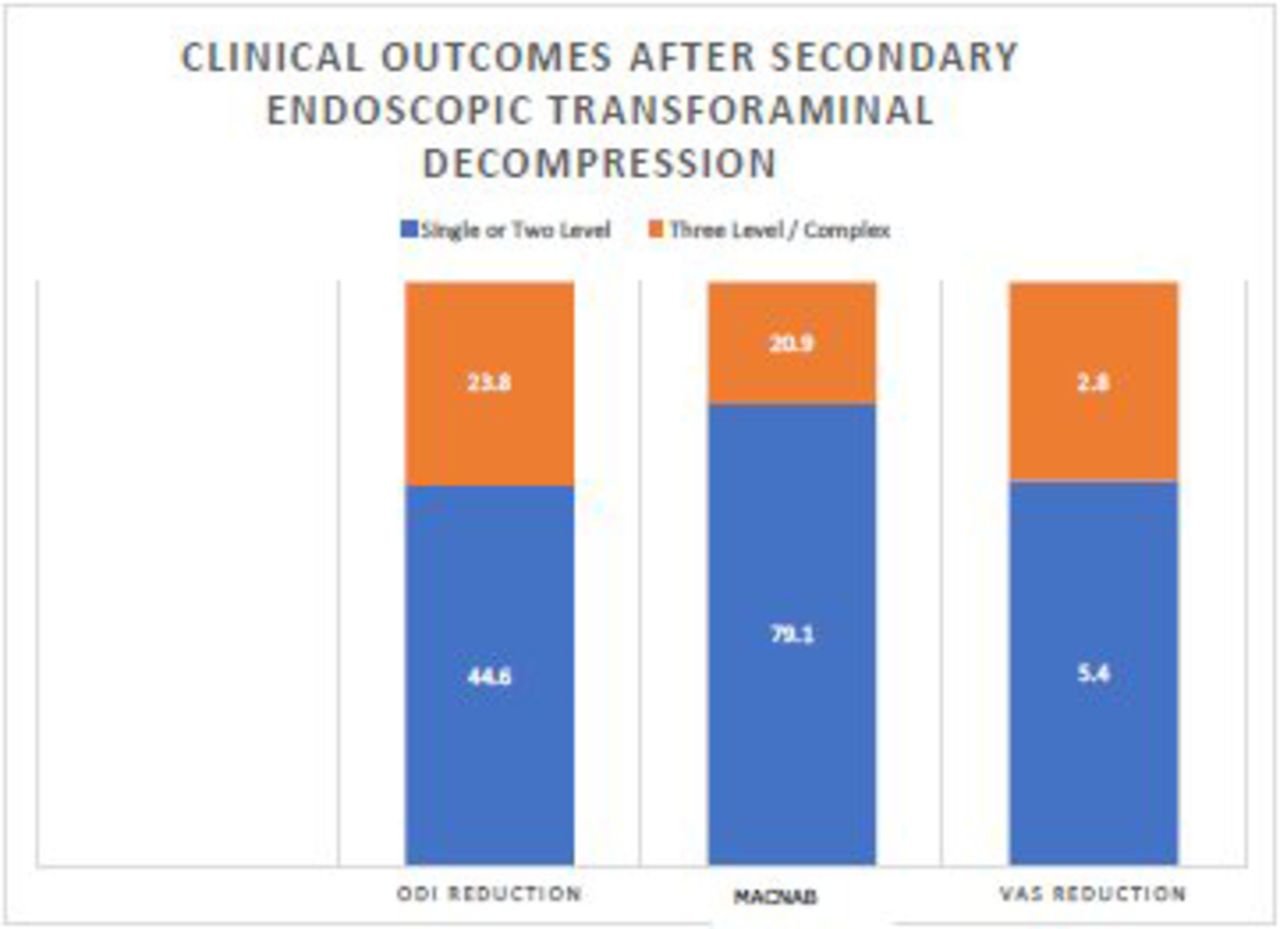
Postoperative ODI (44.6 vs. 23.8) and VAS (5.4 vs. 2.8) score reductions were much greater in patients with single- or 2-level secondary surgeries, respectively. Most patients (79.1%) with single- to 2-level secondary surgeries also had “excellent” to “good” outcomes according to Macnab criteria, whereas “fair” to “poor” outcomes were reported almost exclusively by patients with 3-level or complex prior surgeries.
- Figure 10
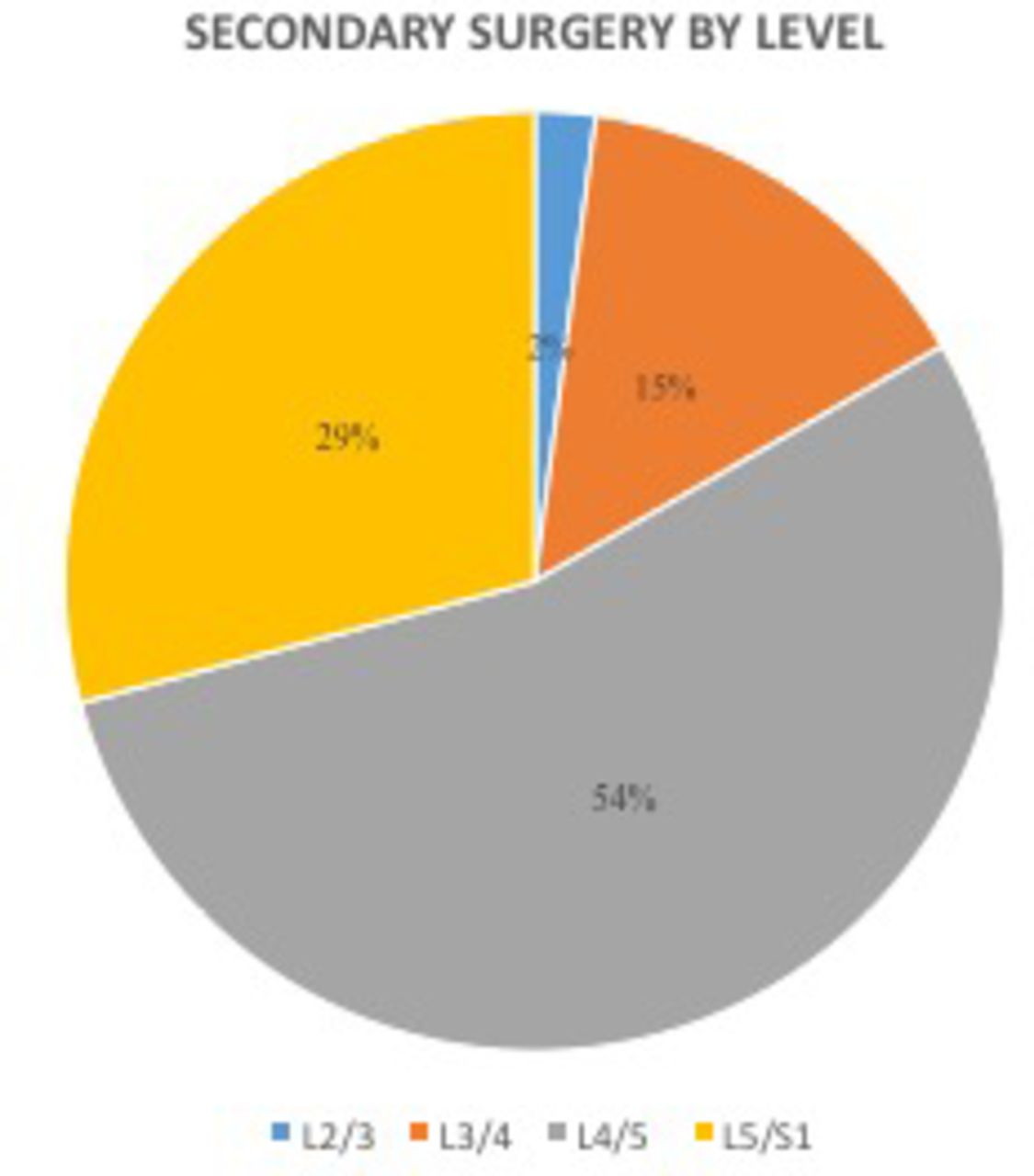
Secondary surgery by lumbar level via endoscopic transforaminal decompression surgery.






Tables
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Magnetic Resonance Imaging Documentation of Approach Trauma With Lumbar Endoscopic Interlaminar, Translaminar, Compared to Open Microsurgical Discectomy
- Is Decompression and Partial Discectomy Advantageous Over Decompression Alone in Microendoscopic Decompression Of Monosegmental Unilateral Lumbar Recess Stenosis?
- Minimal Clinically Important Difference in Patient-Reported Outcome Measures with the Transforaminal Endoscopic Decompression for Lateral Recess and Foraminal Stenosis