


ABSTRACT
Background: Our purpose was to evaluate the efficacy of the extrapendicular approach for unilateral percutaneous vesselplasty in dealing with Kummell disease patients.
Methods: Twenty-seven patients undergoing vesselplasty at our institution were enrolled in the study. Vesselplasty was performed using percutaneous extrapendicular technique. Pain, restoration of vertebral body height, and cement leakage were evaluated in the process.
Results: Substantial pain relief was attained in all the patients. The visual analogue scale improved significantly from pre- to postoperation (P < .05), and remained unchanged at every follow-up. The anterior vertebral body heights were significantly corrected after operation (P < .05). No cement leakage was found.
Conclusion: This new technique of vesselplasty offers statistically significant benefits in Kummell disease patients. It also makes vesselplasty feasible, safe, and effective.
INTRODUCTION
Kummell disease is a rare type of vertebral avascular necrosis first described by Hermann Kummell in 1895.1 It is characterized by patients suffering a trivial spinal trauma, but developing a symptomatic, progressive, angular kyphosis after a symptom-free period of months to years. It is a complication of vertebral compression fractures (VCFs). Since the original description, multiple terms have been used to describe this pathology: vertebral osteonecrosis, pseudoarthrosis of vertebral fracture, VCF nonunion, intravertebral vacuum cleft, and delayed vertebral collapse.2–4 With the advent of radiographic technology, it was recognized that this uncommon spinal disorder represented posttraumatic vertebral fractures, which present with unobvious initial X-rays findings, but subsequent vertebral body collapse.5,6
Kummell disease occurs primarily in middle-aged and elderly patients, with a slight male predominance, suggesting that the prevalence will increase as the population ages. In the last half century, there have been very few published reports on cases that meet the criteria set by Kummell.6 Although the concept of Kummell disease is ambiguous, with the advancement of preoperative radiographic evaluations of vertebral status, in particular with the population of magnetic resonance imaging, more and more VCFs are found to be Kummell disease.7
The conventional management of symptomatic VCFs is medical therapy, which includes analgesics, bed rest, external bracing, and rehabilitation.8,9 These treatments are only partially effective and do not prevent kyphotic deformity.9 Moreover, bed rest accelerates bone resorption and leads to an increased risk of future fractures. Surgery is generally limited to cases of spinal instability or neurologic deficit.10–12 However, surgical fixation often fails because of the poor quality of osteoporotic bone.10 For these reasons, physicians have become interested in new methods for pain relief and functional restoration with the goal that patients may return to their activities of daily living.13
Vertebroplasty and balloon kyphoplasty are two minimally invasive percutaneous approaches developed for the treatment of symptomatic VCFs.
Percutaneous vertebroplasty (PVP) was first performed in 1984.14 It is an imaging-guided procedure in which polymethylmethacrylate (PMMA) is percutaneously injected into the vertebral body with the fracture. Although not well established, the most likely mechanism for pain relief after vertebroplasty treatment appears to be mechanical stabilization of the vertebral body. In most ex vivo studies, injection of cement into the vertebral body restored its stiffness and increased its strength.15 The main risks of this technique are leakage of PMMA into the venous system, with the possibility of pulmonary embolism, or into the spinal canal or neural foramina, precipitating neurologic disorders.
Percutaneous balloon kyphoplasty, a modification of vertebroplasty, involves inflation of a high-pressure balloon (KyphX Inflatable Bone Tamps, Kyphon) within the collapsed vertebral body followed by percutaneous injection of bone cement into the cavity created by the balloon.16 This procedure was devised and first performed in 1998.17 The risk of cement extravasation is reduced with balloon kyphoplasty because of the lower-pressure injection of high-viscosity cement into a previously formed cavity,18 with new bone margins created by the compressed trabeculae.
Vesselplasty is a new intriguing alternative to vertebroplasty and kyphoplasty. It was devised to obtain control of the volume of void created in the vertebral body, prevent the leakage of bone filler material, and restore vertebral body height. Designed by Jerry Lin, the chairman of A-Spine Holding Group Corporation (Taipei, Taiwan), vesselplasty was first performed in 2004 by Darwono (Darwono B, presented at the 2004 Triennial Asia Pacific Orthopedic meeting, Kuala Lumpur, Malaysia). Instead of using a balloon to create a cavity, vesselplasty uses a polyethylene terephthalate (PET) balloon container (Vessel-X, A-Spine Holding Group Corporation) to restore the height of the vertebral body. This receptacle serves as both a vertebral body expander and a bone cement container. It is introduced into the vertebra in its reduced configuration and, once positioned within the vertebra, is expanded by the injection of PMMA. Then, owing to the porous structure comprising the fibers of the PET vessel, a small amount of bone cement permeates through its wall and interdigitates within the vertebral body to increase its stability. Theoretically, this technique solves the problem of leakage of cement from the vertebral body, because most of the cement is contained by the expandable artificial vessel, providing a safe method to treat Kummell disease.
In this article, we describe performance of percutaneous vesselplasty via a unilateral extrapedicular approach to improve the syndrome in patients diagnosed with Kummell disease.
MATERIALS AND METHODS
Twenty-seven patients undergoing percutaneous vesselplasty to treat Kummell disease at Zhejiang Xin'an International Hospital from December 2014 to November 2016 were enrolled in our study. The mean age of the patients was 83 years old (Table 1). Each patient had severe back pain. Radiographs demonstrated a burst fracture with a vacuum phenomenon for each patient (Figure 1). Patients with previous spine surgery, infection, tumor, or neurological impairment were excluded.
Characteristics of patients.
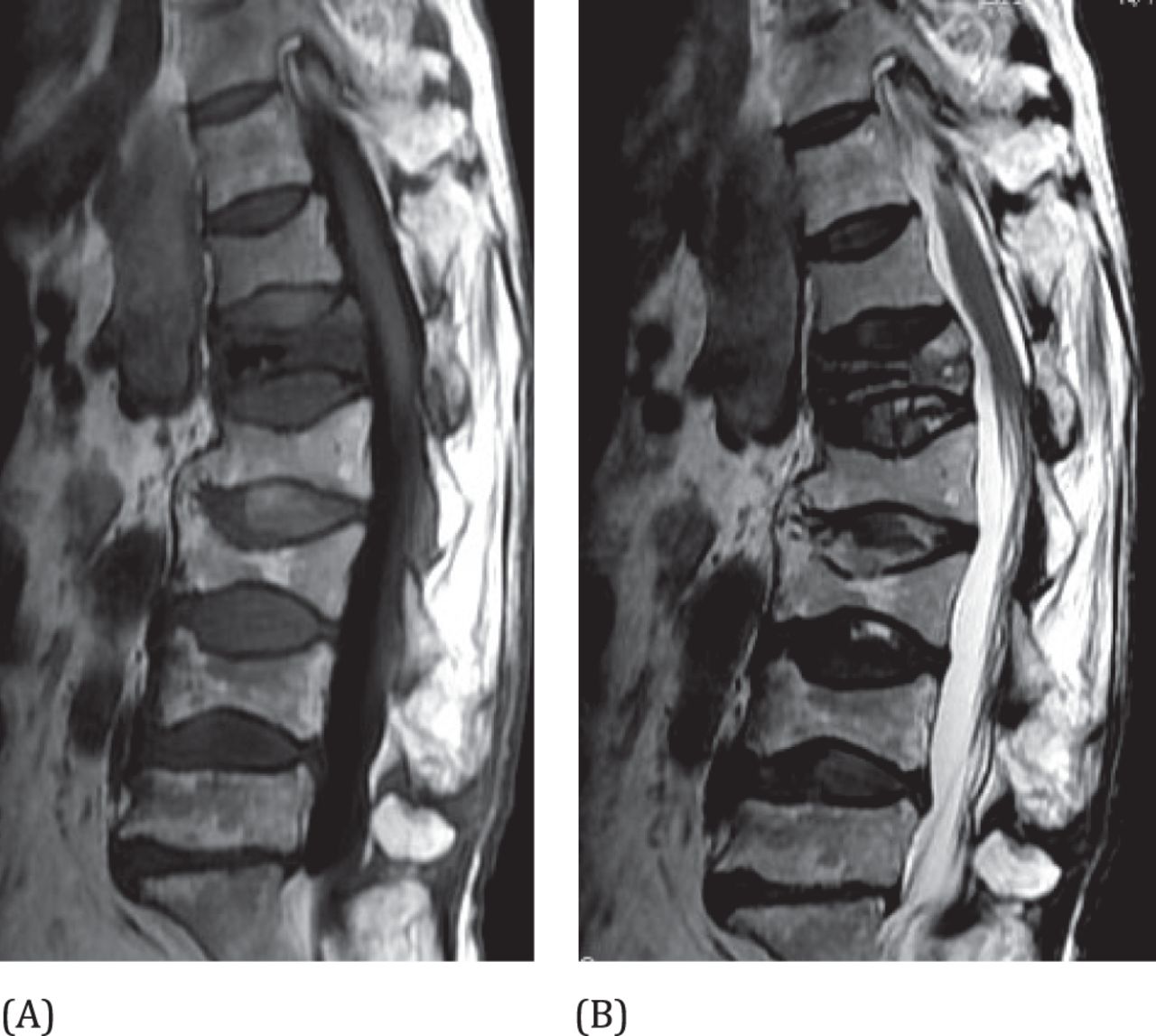
Sagittal T1-weighted (A) and T2-weighted (B) magnetic resonance images of an 83-year-old woman with Kummell disease at the L1 level.
The efficacy of vesselplasty was evaluated using the visual analog scale for pain (VAS). In addition, radiographic data, including the anterior vertebral height and the leakage of bone cement were measured. Clinical examinations were performed prior to surgery and postoperatively (1 day, 3 days, and 1 month after vesselplasty).
Surgical Technique
Local anesthesia was administered to the patient prior to the surgery. The patient was placed in the prone position and injection needles were used to pass through the skin and puncture the edge of vertebra with a unilaterally external approach. A puncture needle 3.5 mm in diameter was advanced unilaterally through skin into the vertebral body. A C-arm machine monitored the needle inserted into the vertebral body center. The needle was exchanged for a working cannula over a K-wire 1.5 mm in diameter through which a drill trocar was advanced creating a channel for the PET balloon container. Before the balloon container was advanced into the vertebral body, the liquid had to be extracted. The drill trocar was removed and the inflatable balloon container was advanced into the anterior one-third of the vertebral body under C-arm machine monitoring. The balloon was inflated under C-arm machine guidance to no more than 200 psi. PMMA cement was injected into balloon container when it became doughy and could stand at the tip of the bone cement inserter. Injection of PMMA was performed under fluoroscopic guidance and continued until maximal expansion of the PET vessel. The volume of bone cement injected into the vertebra was a mean of 2 mL (Figure 2). The vessel introducer and the pushing rod were removed, followed by the cannula tube. Once these elements had been removed, the posterior opening of the PET balloon container was mostly sealed because of the cement's short solidification time. After the surgery, the patients were required to rest for 6 hours, and during this period the vital signs, neurology, sensory motor functions of the lower limbs were monitored.
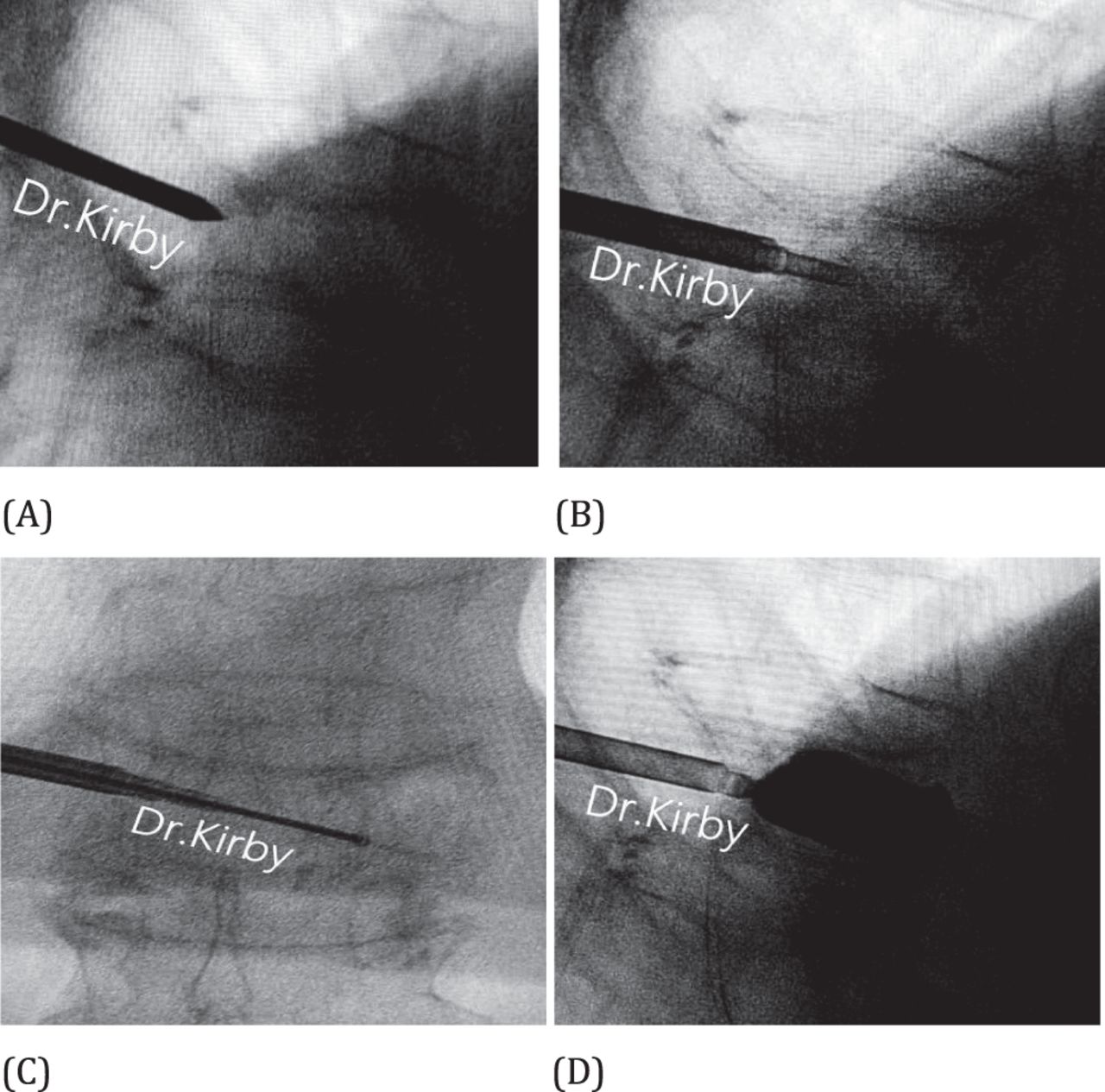
Photographs show percutaneous vesselplasty procedure with C-arm imaging; the cement is injected with an external approach to the vertebra.
We used VAS and anterior vertebral body height to evaluate the effects of our novel technique.
Statistical Analysis
Continuous data were expressed as the mean ± SD. A comparison of continuous variables pre- and postsurgery was performed using a one-way analysis of variance. P ≤ .05 was considered to indicate a statistically significant difference.
RESULTS
The percutaneous vesselplasty procedures performed on the patients with Kummell disease were successful and without severe complications. The success rate of the puncture surgery was 100%. The clinical assessments of the patients were performed at 24 hours, 3days, and 1month postsurgery.
All the patients in our study showed that the VAS and anterior vertebral height significantly improved at 1 day postoperatively (P < .05), and the improvement was sustained before discharge. Cement leakages were zero in all the patients. The mean preoperative VAS score was 8.7 ± 0.3. Substantial pain relief was achieved with each patient. The mean postoperative VAS score reduced to 2.3 ± 0.5 at 1 day postprocedure. The effect of pain control was persistent. The average VAS changed slightly at every follow-up (Table 2).
Mean change in visual analog scale for pain (VAS).
Mean improvement of anterior vertebral body height.
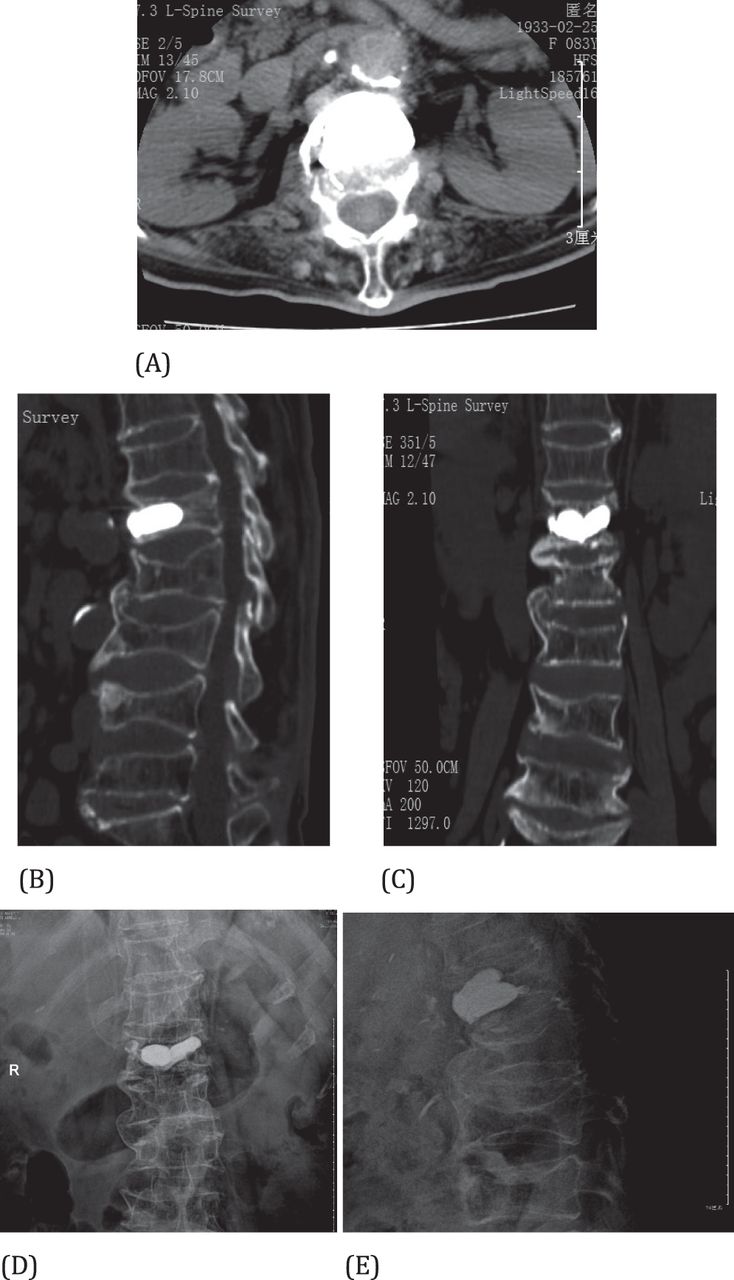
The mean postoperative anterior vertebral body heights were significantly increased compared with preoperative heights (Figure 3; Table 2). There were no significant differences between the immediate postoperative and follow-up assessments. No cement leakage into the spinal canal and no further dislodging of the posterior vertebral body fragments occurred.
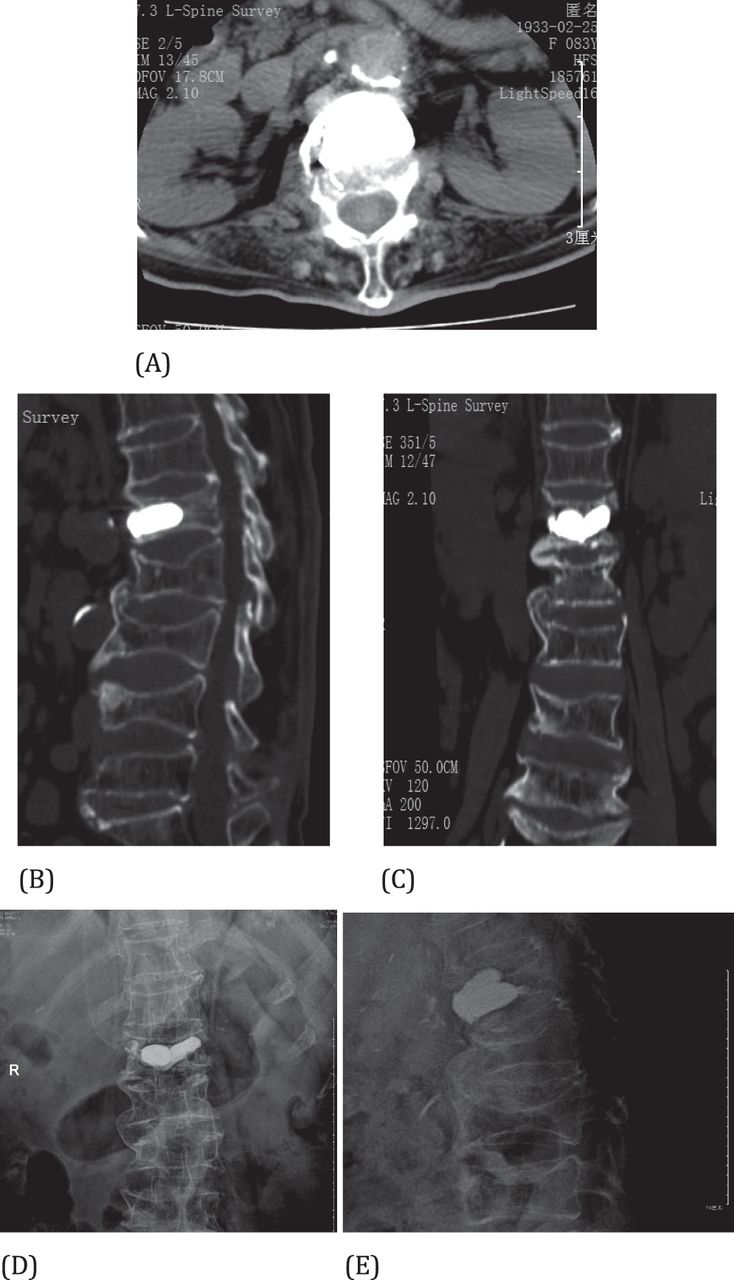
A 82-year-old woman with Kummell disease at the L1 level on computed tomography and X-ray. Coronal (A), sagittal (B), and axial (C) computed tomography images showed the position of bone cement after operation. Postoperation AP (D) and lateral (E) radiographs of the lumbar spine demonstrate high-density bone cement within the anterior 2/3 of the vertebral body post–percutaneous vesselplasty.
DISCUSSION
Kummell disease is defined as delayed posttraumatic vertebral collapse and often occurs in patients with osteoporosis, extensive spondylosis, or advanced age, or those undergoing long-term steroid therapy. Involvement of a single vertebral body is most common. The fractured and necrotic vertebral body typically is located in the thoracic or lumbar spine with the T12 vertebral body being the most commonly affected.19
Treatment for Kummell disease remains controversial. Although early reports were centered on conservative treatment such as bracing and bed rest, more recent reports favor surgical intervention. Heini reported that 36% of VCFs are progressive, and conservative treatment is not effective for these aging cases with cord compression.20 For the aged patients, long-term lying in bed can induce many complications, some of which are fatal. Surgical intervention is necessary for such conditions. There are some significant clinical challenges and disputes when performing surgical treatment for osteoporotic vertebral collapse with neurological deficits.21–23 The advantages of surgery include earlier patient ambulation and correction of the kyphotic deformity. However, extensive surgical intervention in the early stages remains challenging because of medical comorbidities or fixation complication secondary to osteoporosis. Early disease can be treated effectively by PVP or percutaneous kyphoplasty (PKP), allowing mobilization earlier than that by conventional open techniques. However, PVP has been reported to have a higher risk of cement leakage than PKP.24 Our study evaluated the effectiveness of vesselplasty for treating patients with Kummell disease. To our knowledge, this study is the first of its kind about this procedure.
Effects of PKP in treating osteoporotic VCFs have been demonstrated in many studies.25–30 Due to disadvantages of longer operation time, more surgical trauma, and higher doses of radiation exposure, traditional bilateral PKP has gradually been replaced by unilateral approach.31
Complications of PKP include cement extravasation, fractured transverse processes or ribs, dural tears, infection, hematomas, and subsequent VCF.32,33 The most common complication is cement extravasation, typically, into epidural, foraminal, intradiscal, and paravertebral veins. Cement leakage into the spinal canal is a devastating complication resulting in spinal cord injury.
Treatment of symptomatic Kummell disease depends on the severity of the patient's pain and the presence of any neurological deficits. Both PVP and PKP have been shown to restore vertebral height and alleviate pain markedly. Pain relief is thought to be due to the filling the entire cleft with cement is important to ensure a pain-free postoperative period.34,35 Pain was markedly relieved in all the patients in our study at 1 day postoperatively.
In this study, at 1 day postoperatively, we found the restoration of the anterior vertebral height was from 17.72 to 27.48 mm. For Kummell disease, the vertebral height varies with postural changes because of the cleft and thus the anterior vertebral height can be significantly corrected in an extended posture.
In Kummell disease with severe spinal canal stenosis, the posterior vertebral wall is always collapsed, which increases the potential risk of cement leakage into the spinal canal and further spinal canal compromise during PVP or PKP.36,37 Concerning the higher rate of cement leakage in PVP than PKP, our study chose the unilateral extrapedicular approach of percutaneous vesselplasty and no obvious cement leakage or neurological deterioration were found.
As patients with Kummell disease may have had an empty space surrounded by fibrotic tissues, the cement leakage may be reduced by those fibrotic tissues. In order to distribute the cement more viscously, Greene et al designed an eggshell technique, which included another balloon placement once the cement had been inserted.38
In most of the procedures reported in this work, the percutaneous vesselplasty approach was the best one for Kummell disease treatment. This surgical method is intended to avoid the risk related to leakage of cement. The absence of symptomatic complication in our study population attests to the safety of the vesselplasty procedure. To our knowledge, this new technique used in Kummell disease has not been reported in the literature, so there are no studies with which to compare our results.
Pain, mobility, and vertebral heights improved significantly after vesselplasty in our study (P < .05). Neurological function improvement can be maintained during the follow-up period for the patients. The extrapendicular approach of percutaneous vesselplasty needs only a short operation time, and is accomplished without much bleeding. So it is suitable for these patients who are not good in general health and cannot endure a spinal-shortening procedure. It can relieve pain quickly and stabilize a fractured vertebral body instantly. Besides, it's worth mentioning that our novel technique requires a lower cost and lower doses of radiation exposure compared with other techniques. Nonetheless, its long-term outcome still needs further clinical observation.
The present research still has some limitations for a small number of patients, which possibly affected the statistical power. Another, the study had a only a short follow-up period. Therefore, additional prospective studies may aid in gathering more definitive evidence.
In summary, the results of our novel technique prove that it offers statistically significant benefits in the improvement of pain, mobility, and the anterior vertebral body heights in patients with Kummell disease. The extrapendicular approach of percutaneous vesselplasty is an effective, minimally invasive procedure for the treatment of Kummell disease that can achieve equal biomechanical strength with less bone cement and lower doses of radiation exposure.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.