


ABSTRACT
Background: Given the paucity of literature regarding compensatory mechanisms used by obese patients with sagittal malalignment, it is necessary to gain a better understanding of the effects of obesity on compensation after comparing the degree of malalignment to age-adjusted ideals. This study aims to compare baseline alignment of obese and nonobese patients using age-adjusted spino-pelvic alignment parameters, describing associated spinal changes.
Methods: Patients ≥ 18 years with full-body stereoradiographs were propensity-score matched for sex, baseline pelvic incidence (PI), and categorized as nonobese (body mass index < 30kg/m2) or obese (body mass index ≥ 30). Age-adjusted ideals were calculated for sagittal vertical axis, spino-pelvic mismatch (PI-LL), pelvic tilt, and T1 pelvic angle using established formulas. Patients were stratified as meeting alignment ideals, being above ideal, or being below. Spinal alignment parameters included C0-C2, C2-C7, C2-T3, cervical thoracic pelvic angle, cervical sagittal vertical axis SVA, thoracic kyphosis, T1 pelvic angle, T1 slope, sagittal vertical axis, lumbar lordosis (LL), PI, PI-LL, pelvic tilt. Lower-extremity parameters included sacrofemoral angle, knee flexion (KA), ankle flexion (AA), pelvic shift (PS), and global sagittal angle (GSA). Independent t tests compared parameters between cohorts.
Results: Included: 800 obese, 800 nonobese patients. Both groups recruited lower-extremity compensation: sacrofemoral angle (P = .004), KA, AA, PS, GSA (all P < .001). Obese patients meeting age-adjusted PI-LL had greater lower-extremity compensation than nonobese patients: lower sacrofemoral angle (P = .002), higher KA (P = .008), PS (P = .002), and GSA (P = .02). Obese patients with PI-LL mismatch higher than age-adjusted ideal recruited greater lower-extremity compensation than nonobese patients: higher KA, AA, PS, GSA (all P < .001). Obese patients showed compensation through the cervical spine: increased C0-C2, C2-C7, C2-T3, and cervical sagittal vertical axis (all P < .001), high T1 pelvic angle (P < .001), cervical thoracic pelvic angle (P = .03), and T1 slope (P < .001), with increased thoracic kyphosis (P = .015) and decreased LL (P < .001) compared to nonobese patients with PI-LL larger than age-adjusted ideal.
Conclusions: Regardless of malalignment severity, obese patients recruited lower-limb compensation more than nonobese patients. Obese patients with PI-LL mismatch larger than age-adjusted ideal also develop upper-cervical and cervicothoracic compensation for malalignment.
Level of Evidence: III
Clinical Relevance: Clinical evaluation should extend to the cervical spine in obese patients not meeting age-adjusted sagittal alignment ideals.
INTRODUCTION
In response to progressive sagittal malalignment, the body minimizes muscle energy expenditure and maintains balance through a chain of spinopelvic and lower-extremity compensatory mechanisms.1,2 In cases of anterior spinopelvic alignment, decreased lumbar lordosis (LL) drives forward truncal alignment and subsequent compensatory thoracic hypokyphosis, pelvic retroversion, knee flexion (KA), and ankle dorsiflexion, among other changes.3–5 Regardless of whether these changes in sagittal alignment are age-related or pathological, effective care for progressive anterior sagittal malalignment requires a full understanding of spinopelvic and lower-extremity compensation.
Patterns of spinopelvic and lower-extremity compensation secondary to progressive sagittal malalignment have previously been described in patients diagnosed with adult spinal deformity.6,7 Ferrero et al8 demonstrated differential recruitment of lower-limb compensatory mechanisms, particularly KA, among adult spinal deformity patients with varying T-1 spinopelvic inclinations. Another study assessing age-related differences in spinopelvic and lower-limb compensation among adult spinal deformity patients found differential recruitment of KA and ankle dorsiflexion in older patients with severe sagittal deformity.9 Unfortunately, differences in compensatory mechanisms between obese and nonobese patients are undercharacterized in the literature.
Recent research shows both obesity and advanced age as associated with changes in sagittal alignment.10–12 It follows, then, that patient-related factors of obesity and age should affect the recruitment of spinopelvic and lower-extremity compensatory mechanisms for sagittal malalignment. Indeed, a recent study found that obese patients with progressive sagittal malalignment recruit more lower-extremity compensation than nonobese patients, when controlling for age, sex, and baseline pelvic incidence (PI).13 This study was lacking, however, in its failure to stratify patient cohorts by age-adjusted spinopelvic alignment goals. As ideal sagittal alignment has been shown to vary with age, a complete comparison of compensatory mechanisms between obese and nonobese patients must take into account normal, age-related changes in sagittal alignment.14
The present study aims to compare the spinopelvic alignment of obese and nonobese patient cohorts using age-adjusted alignment parameters, describing how the cohorts differ in recruitment of compensatory mechanisms for progressive sagittal malalignment.
MATERIALS AND METHODS
Data Collection
This study was a retrospective review of patients visiting a single academic center for spine-related complaints from 2013 to 2015. Data, including age, sex, and body mass index (BMI) were collected prospectively on consecutive patients. Inclusion criteria included patients ≥ 18 years with available full-body radiographs. Patients underwent full-body, biplanar stereographic imaging (EOS Imaging, Paris, France), positioned in a weight-bearing, free-standing position, arms flexed at 45° with fingers on the clavicles to avoid superimposition with the spine.15,16 This position optimizes view of spinal components without altering the patient's center of gravity.17 Institutional review board approval was obtained before study initiation.
Analysis of Radiographic Parameters
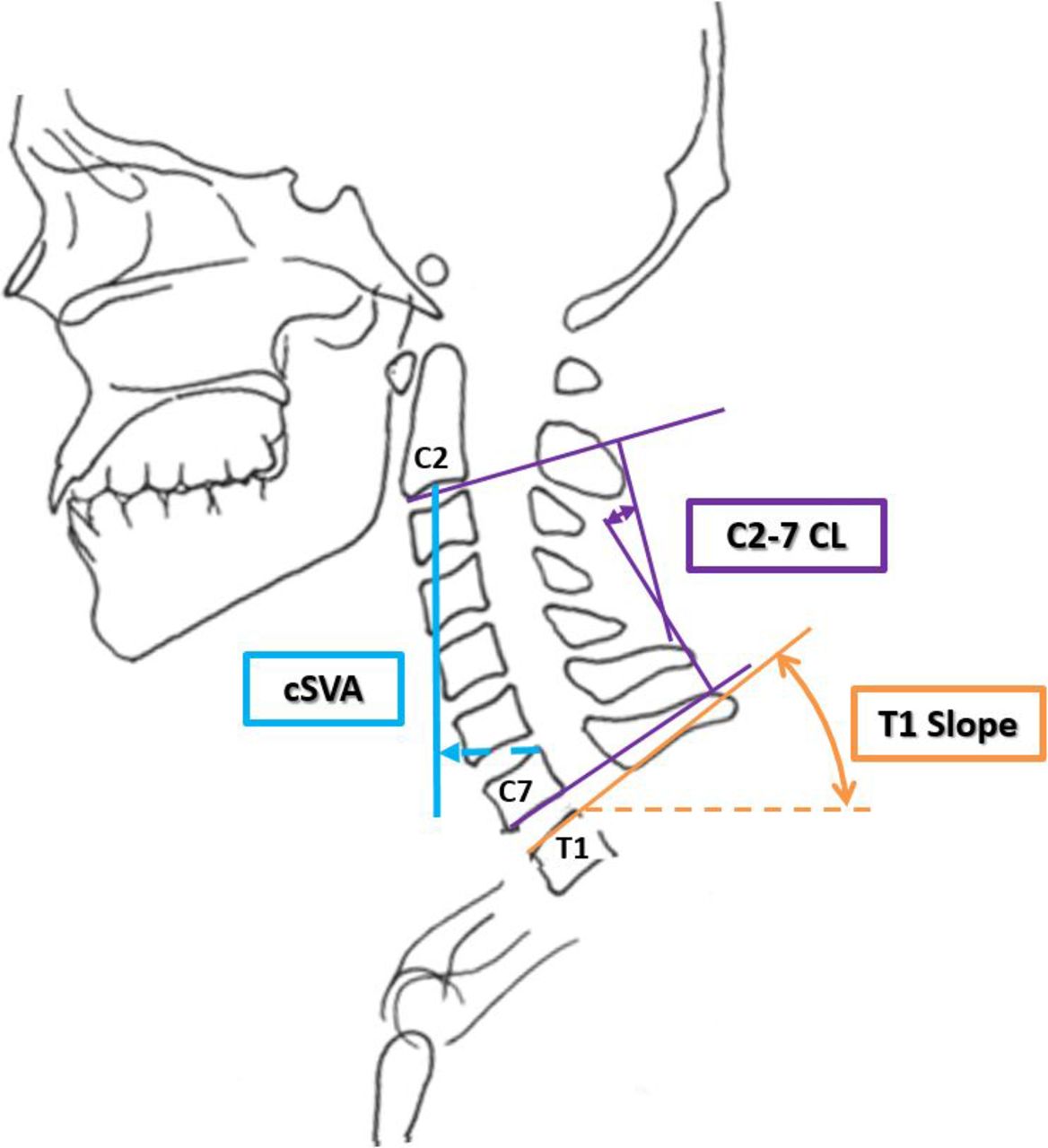
Alignment parameters were measured at a single center using validated software (Surgimap, Nemaris Inc., New York, New York).18 Cervical and cervicothoracic spinal alignment parameters assessed were C0-C2, C2-C7, and C2-T3 angles, cervical thoracic pelvic angle (angle between a line from the centroid of C2 to femoral heads and a line from femoral heads to centroid of C1), T1 slope (angle between horizontal and superior endplate of T1), and cervical sagittal vertical axis (cSVA: sagittal offset from plumb line extended from centroid of C2 to posterior superior aspect of C7; Figure 1).

Schematic of cervical alignment parameters.
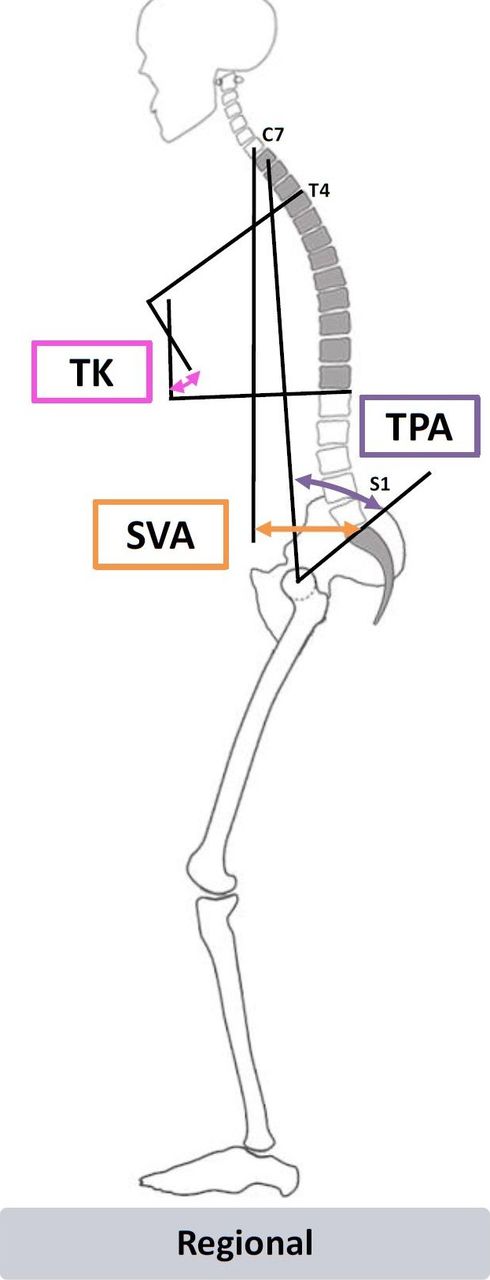
Figure 2 shows a schematic of regional parameters, including thoracic kyphosis (sagittal Cobb angle between upper endplate of T4 and lower endplate of T12), T1 pelvic angle (TPA: angle formed by the line between the center of T1 vertebral body and the bicoxofemoral axis and the line between the bicoxofemoral axis and the middle of S1 endplate), and sagittal vertical axis (SVA: horizontal distance between plumb line extended from C7 vertebral body and posterosuperior S1 vertebral corner).
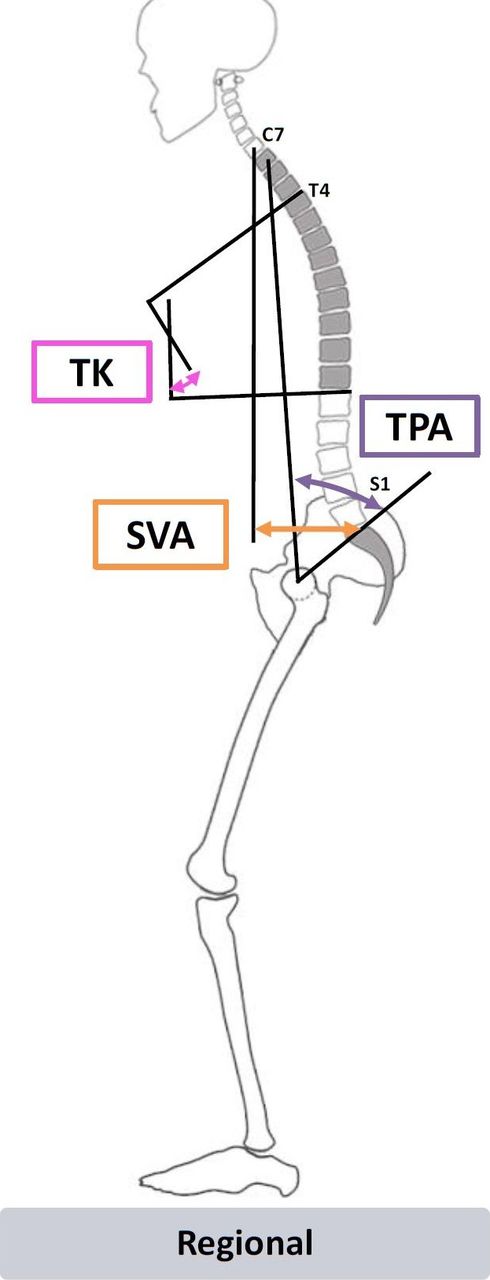
Schematic of regional alignment parameters.
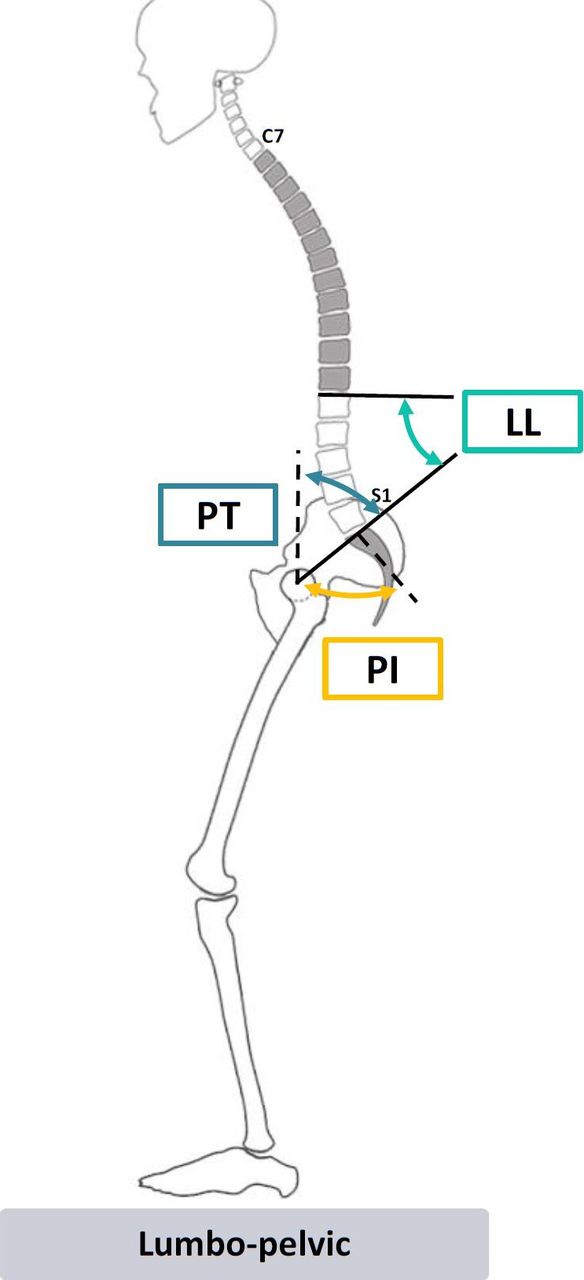
Lumbo-pelvic measurements are outline in Figure 3, and included lumbar lordosis (LL: angle between upper endplate of L1 the upper endplate of S1), pelvic incidence (PI: angle between vertical and line from the center of the bicoxofemoral axis to the midpoint of S1 endplate), pelvic tilt (PT: angle between vertical and line from the center of the bicoxofemoral axis to the midpoint of S1 endplate), and the mismatch between PI and LL (PI-LL).
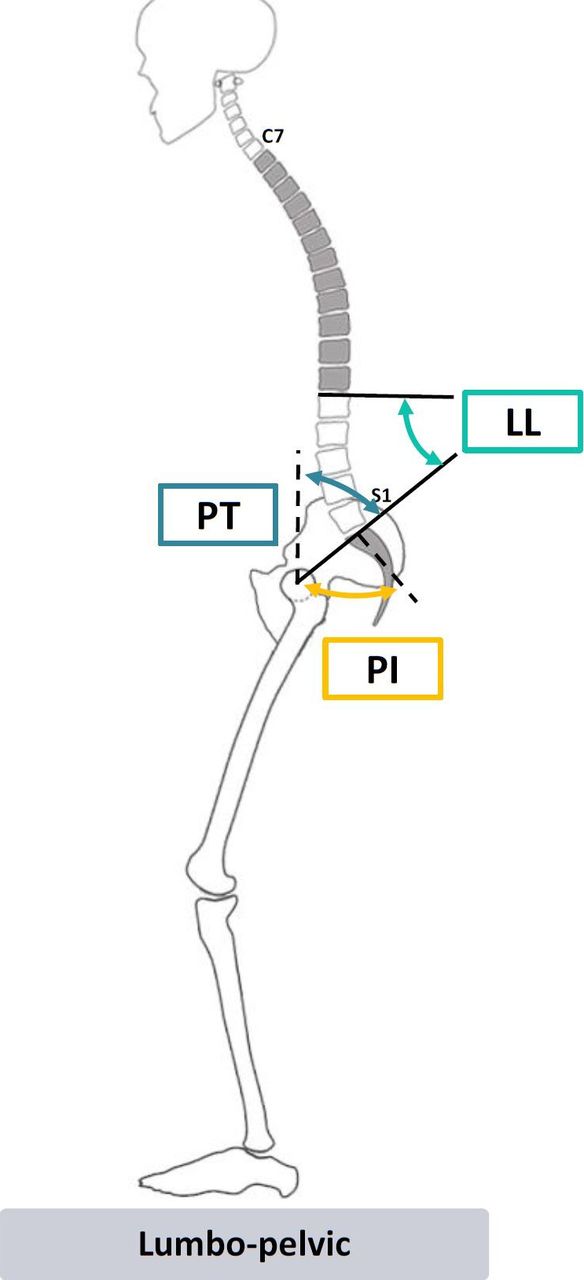
Schematic of lumbopelvic alignment.
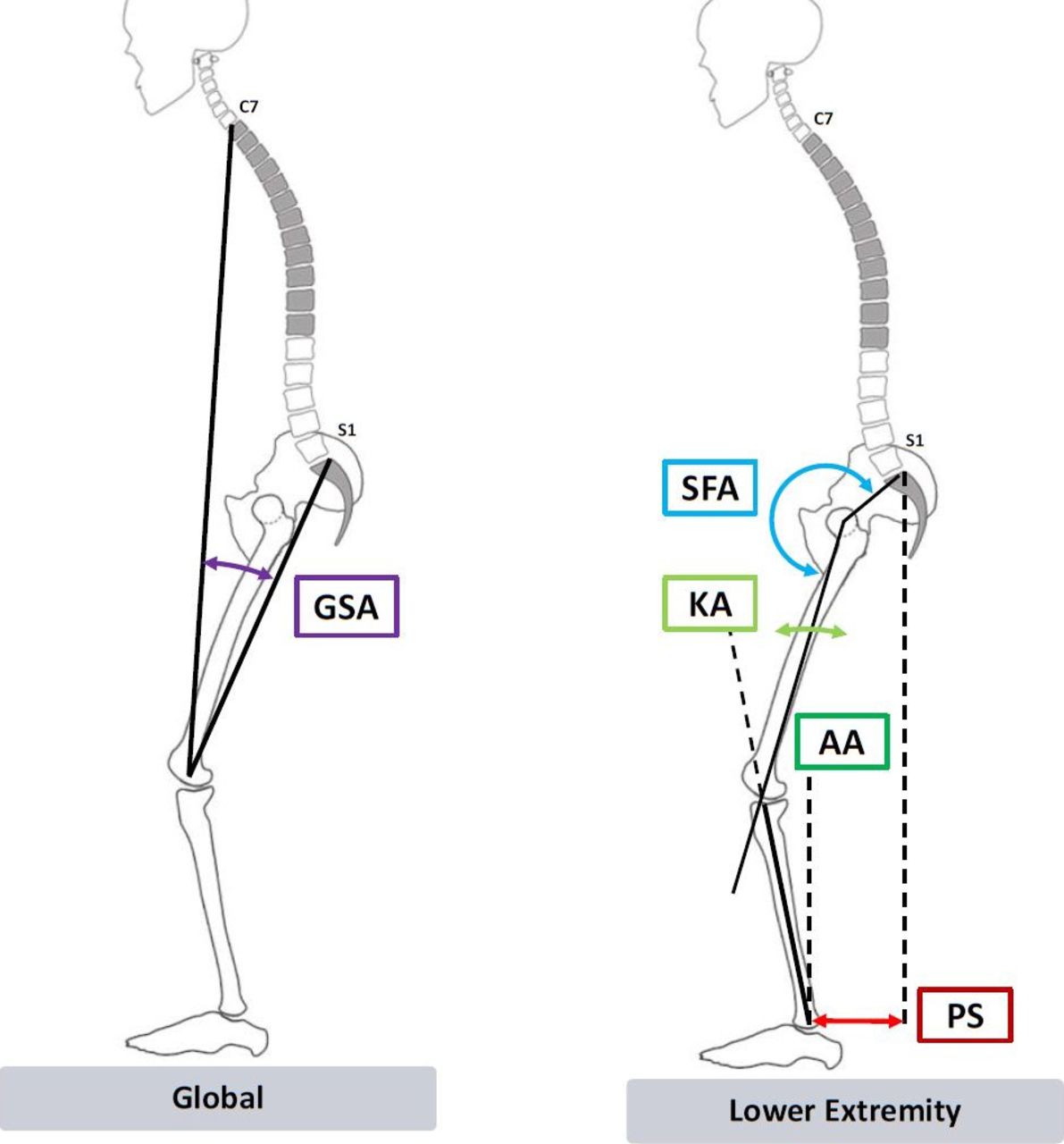
Figure 4 details global and lower-extremity parameters, including sacrofemoral angle (angle formed by the line from the middle of S1 endplate to the bicoxofemoral axis and the line between the bixocofemoral axis and the femoral axis), KA (angle between mechanical axis of the femur and mechanical axis of tibia), ankle flexion (AA: angle between vertical and mechanical axis of tibia), pelvic shift (PS: sagittal offset between posterosuperior corner of the sacrum and anterior cortex of distal tibia), and global sagittal angle (GSA: angle of the line between the middle of C7 vertebral body to the knee, to the midpoint between the 2 femoral condyles and the line extended from this point to the posterosuperior aspect of S1).
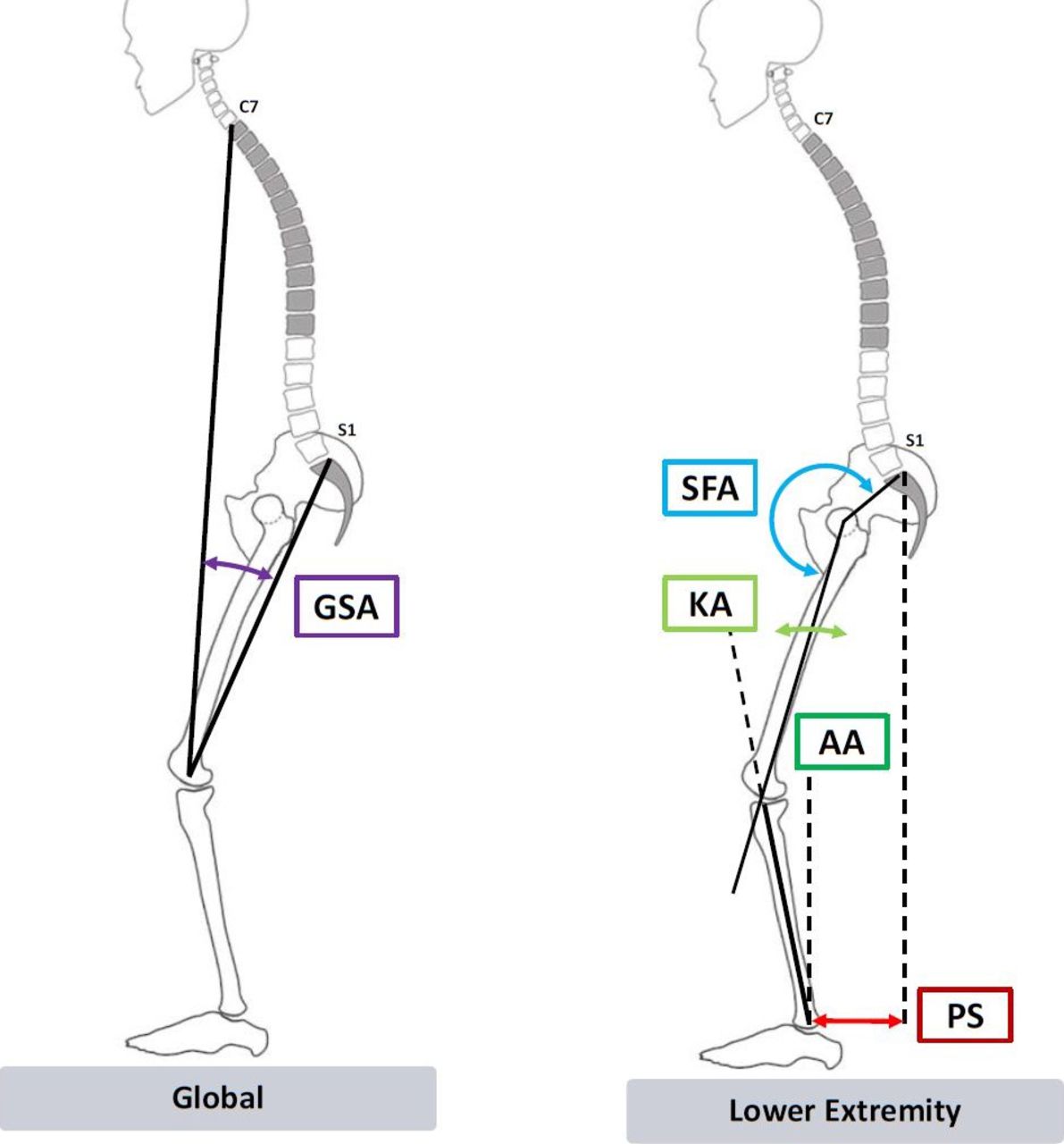
Schematics of global (left) and lower extremity (right) alignment parameters.
Statistical Methods
All statistical tests were performed using SPSS software (v21.0, Armonk, NY, USA). Included patients were grouped into 2 cohorts according to BMI at first visit: obese (BMI ≥ 30 kg/m2) and nonobese (BMI < 30 kg/m2). Obese and nonobese cohorts were propensity-score matched for the potentially confounding covariates of sex and baseline PI, as previously described in the literature.13 Age-specific alignment ideals were established for SVA, PI-LL, PT, and TPA, based on previously published values14:

Patients meeting alignment ideals within a ± 10-year window of their age were considered matches for age-specific alignment. Obese and nonobese cohorts were then stratified by patients who matched age-specific alignment ideals, patients below age-specific alignment ideals, and patients above age-specific alignment ideals. Baseline radiographic parameters were compared between matched cohorts for each age-specific alignment category using independent samples t tests. Statistical significance was set P < .050.
RESULTS
Cohort Overview
Following propensity-score matching, 1600 patients met inclusion criteria (obese = 800, nonobese = 800). The overall cohort had a mean age of 56.5 ± 19.4 years, mean BMI of 29.6 ± 7.1 kg/m2, and was comprised of 51.7% females. Among the most common overall diagnoses were scoliosis (20.9%), lower back pain (11.4%), stenosis (9.3%), and spondylolisthesis (6.5%). There were no significant differences in patient sex between obesity cohorts. Compared to the nonobese cohort, the obese cohort reported significantly inferior health-related quality of life scores on the SRS-22 questionnaire (3.6 ± 0.8 and 2.8 ± 0.7, respectively, P < .001) and the Oswestry Disability Index (29.6 ± 21.9 and 42.8 ± 21.0, respectively, P < .001). Obese patients had significantly larger forward sagittal alignment as measured by SVA and TPA (Table 1, both P < .001), and showed significantly less lumbar lordosis (P < .001) than nonobese patients. On average, obese patients adopted significantly more C0-C2 extension than nonobese patients (P < .001), and had larger cSVAs (P = .011). All patients recruited lower-extremity compensation in sacrofemoral angle (P = .004), KA, AA, PS, and GSA (all P < .001).
Overall comparison of baseline sagittal spino-pelvic and lower-extremity radiographic parameters between obese and nonobese patient cohorts. P values for significant differences between means set to P < .05; bold type indicates significance at P < .05.
Comparison of Radiographic Parameters by Age-Adjusted PT Category
Table 2 shows that in all age-adjusted PT categories, obese patients compensated for sagittal malalignment through pelvic retroversion, adopting significantly greater PI-LL and PT than nonobese patients (all P < .050). All obese cohorts similarly adopted greater TPA, T1 slope, and SVA than corresponding nonobese cohorts. Obese patients with PT mismatch greater than age-adjusted ideal (P = .001) adopted more upper-cervical C0-C2 compensation than nonobese patients. Significant differences in lower-extremity compensatory mechanisms were also observed in patients across all 3 age-adjusted PT categories, with all obese cohorts adopting higher KA, AA, PS, and GSA than corresponding nonobese cohorts (all P < .040). That said, controlling for age-adjusted differences in TPA, SVA, and PI-LL, there were no significant differences in the recruitment of lower-extremity KA, AA, PS, and GSA compensatory mechanisms between obese and nonobese patients with PT mismatch greater than age-adjusted ideal (all P > .050).
Comparison of baseline sagittal spino-pelvic and lower-extremity radiographic parameters between obesity cohorts of age-adjusted pelvic tilt (PT) alignment ideal categories. Bolded values indicate statistical significance to P < .05.
Comparison of Radiographic Parameters by Age-Adjusted SVA Category
Table 3 shows differences in spino-pelvic and lower-extremity compensatory mechanisms between obesity cohorts across all 3 age-adjusted SVA categories. Notably, obese patients with baseline SVA greater than age-adjusted ideal demonstrated more cervical and cervicothoracic compensation than nonobese patients, indicated by higher C0-C2, C2-C7, and C2-T3 (all P < .010). Obese patients meeting age-adjusted expectations for SVA also showed higher C0-C2 (P = .015) and C2-T3 (P = .043) compensation than nonobese patients. Obese patients with SVA mismatch higher than age-adjusted ideal and obese patients with SVA mismatch lower than age-adjusted ideal showed greater global compensation by the metrics of TPA and T1 slope (all P < .04) as compared to corresponding nonobese cohorts. Obese patients across all 3 categories of age-adjusted SVA recruited greater lower-extremity compensation in KA and PS (all P < .01). Controlling for age-adjusted differences in PT, PI-LL, and TPA, there were no significant differences between obese and nonobese cohorts in their recruitment of compensatory C0-C2 lordosis for patients with SVAs matching age-adjusted ideals (P > .050). Still, across all 3 SVA age-adjusted categories, obese patients had significantly higher KA and PS than nonobese patients (P < .025).
Comparison of baseline sagittal spino-pelvic and lower-extremity radiographic parameters between obesity cohorts of age-adjusted sagittal vertical axis (SVA) alignment ideal. Bolded values indicate statistical significance to P < .05.
Comparison of Radiographic Parameters by Age-Adjusted PI-LL Category
Table 4 shows increased recruitment of lower-extremity compensatory mechanisms for obese patients across all 3 age-adjusted PI-LL categories. In all age-adjusted PI-LL categories, obese patients showed higher KA and GSA compared to nonobese patients (all P < 0.020). Compared to nonobese, obese patients with PI-LL mismatch greater than age-adjusted ideal showed recruitment of upper-cervical and cervical compensatory mechanisms: C0-C2 (P < .001), cervical thoracic pelvic angle (P = .030), cSVA (P = .042). Obese cohorts in which PI-LL mismatch was greater than age-adjusted ideal and in which PI-LL mismatch was lower than age-adjusted ideal showed less lumber lordosis (P < .001 and P = .004, respectively) and had significantly larger TPA values (both P < .001) than corresponding nonobese cohorts. Controlling for age-adjusted differences in PT, SVA, and TPA, there were no significant differences between obese and nonobese patients that matched age-adjusted PI-LL ideal in recruitment of lower-extremity compensatory mechanisms (all P > .050); however, obese patients with PI-LL mismatch greater than age-adjusted ideal and obese patients with PI-LL mismatch less than age-adjusted ideal showed increased KA and PS compensation (all P < .030) as compared to corresponding nonobese patients.
Comparison of baseline sagittal spino-pelvic and lower-extremity radiographic parameters between obesity cohorts of age-adjusted pelvic incidence–lumbar lordosis (PI-LL) alignment ideal categories. Bolded values indicate statistical significance to P < .05.
Comparison of Radiographic Parameters by Age-Adjusted TPA Category
Across all 3 categories for age-adjusted TPA, obese patients had greater lower-extremity compensation in KA, PS, and GSA than nonobese patients (Table 5, all P < .001). Similarly, obese cohorts in all 3 age-adjusted TPA categories had larger mean SVAs than corresponding nonobese cohorts (all P < .001). Obese patients with TPA mismatch greater than age-adjusted ideal also showed increased cervical compensation as compared to nonobese patients, with larger C0-C2 lordosis (P < .001).
Comparison of baseline sagittal spino-pelvic and lower-extremity radiographic parameters between obesity cohorts of age-adjusted T1 pelvic angle (TPA) alignment ideal categories. Bolded values indicate statistical significance to P < .05.
DISCUSSION
Obesity is an urgent public health issue that presents many challenges for healthcare providers. As obesity has been associated with higher perioperative complication rates and poorer long-term surgical outcomes, there is a need for increased understanding, monitoring, and care for obese patients undergoing spine surgery.19–21 Improving postoperative outcomes for obese patients with pathological sagittal malalignment requires a comprehensive preoperative plan that effectively distinguishes the causes of malalignment from the compensatory mechanisms. As such, it is important to understand the compensatory mechanisms used by both obese and nonobese patients with sagittal malalignment, taking into account both patient age and patient-specific morphologies.
Recent research has identified a number of factors that drive sagittal malalignment, including hypertrophic facet joints, arthritis, degenerative disc disease, and age-related atrophy of paraspinal muscles.22,23 In cases of anterior sagittal malalignment, compensation typically begins proximal to the affected area of the spine in an effort to restore lumbar lordosis.3 When spinal physiological and energetic reserves are exhausted, the chain of compensation continues into the pelvis, resulting in increased PT and posterior pelvic shift, and later into the lower extremities.8,24 While compensation for sagittal malalignment is well understood in patients with spinal deformity, there are few studies investigating differences in compensatory mechanisms between obese and nonobese patients. Of note, a recent study found significant differences in patterns of compensation for sagittal malalignment between obese and nonobese patients, with obese patients demonstrating increased posterior pelvic shift and KA.13 That said, the study did not use age-specific spinopelvic alignment goals to compare cohorts. The use of age-adjusted spinopelvic alignment ideals in preoperative planning for sagittal malalignment correction is critical, as normal, nonpathologic sagittal malalignment has been shown to increase with age.14,25
To account for age-related variation in spinopelvic alignment, this study stratified obese and nonobese cohorts as either meeting, exceeding, or falling short of age-adjusted alignment ideals for SVA, PI-LL, PT, and TPA. Our study found that regardless of age-adjusted alignment category, obese patients recruited more lower-extremity compensation than nonobese patients, particularly increased KA and ankle dorsiflexion. These results make sense, given the decreased LL and higher PI-LL mismatch observed in the obese patient cohort. The relationship between KA and LL is well characterized in the literature, as is the relationship between obesity and lumbar hypolordosis.12,26,27 That said, as studies have shown loss of LL as secondary to degeneration of the knee, the results of the present study suggest the need for clinical evaluation of both spinal alignment and KA in obese patients with sagittal malalignment.28
Our results also show that obese patients with PI-LL mismatch larger than age-adjusted ideal developed upper cervical and cervicothoracic junction compensatory mechanisms. Specifically, as compared to nonobese patients, obese patients with PI-LL mismatch larger than age-adjusted ideal showed increased cervical extension, as made evident by significantly larger C0-C2 lordosis, cSVA, and cervical thoracic pelvic angle. This is consistent with previous studies showing the cervical spine as playing a critical role in the maintenance of horizontal gaze in patients with sagittal malalignment.29–31 Indeed, a recent study showed spontaneous postoperative improvement of cervical alignment in patients undergoing surgical correction for positive sagittal malalignment, underscoring the importance of distinguishing between drivers of sagittal malalignment and the compensatory mechanisms that indirectly resolve following direct surgical correction of the drivers.32 Our results show value in careful clinical evaluation of the cervical spine for obese patients with anterior sagittal malalignment.
Further support for thorough clinical cervical spine evaluation in obese patients who do not meet age-adjusted ideals for sagittal alignment comes from the present study's finding of increased cervical compensation in obese patients with SVA measurements larger than age-adjusted ideal. Previous research shows that increased BMI retroverts the sacrum, leading to larger anterior pelvic tilt.33 Thus, it is possible that such biomechanical changes in the spines and pelvises of obese patients could contribute to larger SVA measurements, and consequently more severe anterior sagittal malalignment and compensatory cervical extension.
Limitations
This analysis did not track distribution of adipose tissue, which could affect patterns in recruitment of compensatory mechanisms. Furthermore, our analysis dichotomized patient groups into obese (BMI ≥ 30) and nonobese, without investigating the relationship between morbid obesity (BMI ≥ 40) and sagittal alignment. As the prevalence of morbid obesity has increased over the past 4 decades, future research should further investigate the relationship between BMI ≥ 40 and sagittal compensation for sagittal malalignment.34 Additionally, this study did not control for type of sagittal deformity, the heterogeneity of which may also affect patterns of compensation. The radiographic analysis in this study was also limited to the sagittal plane, not taking into account deformities in the coronal plane that could have affected sagittal alignment. Despite these factors, the large sample size, propensity-score-matched patient cohorts, and age-adjusted radiographic analysis lend our results broad generalizability.
CONCLUSIONS
Obese patients recruit more lower-limb compensation than nonobese patients, regardless of sagittal malalignment severity. Additionally, obese patients with anterior displacement of sagittal balance, as measured by PI-LL and SVA, demonstrate more cervical and upper-cervical compensation than nonobese counterparts. In comparing the age-adjusted sagittal parameters of obese and nonobese cohorts, this study permits a more comprehensive assessment of the compensatory mechanisms recruited by obese patients, and allows for more effective preoperative planning for obese patients with sagittal malalignment.
Footnotes
Disclosures and COI: The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
Ethics Review Committee Statement: Institutional Review Board approval was obtained for this study, prior to patient enrollment.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.